Você também pode gostar
- 2155 9864 S4 002Documento6 páginas2155 9864 S4 002amaliakhaAinda não há avaliações
- Diabetic FootDocumento14 páginasDiabetic FootRini Oyien WulandariAinda não há avaliações
- ECM and Collagen: Structure and Role in Connective TissueDocumento24 páginasECM and Collagen: Structure and Role in Connective TissueFrinciaAinda não há avaliações
- Guideline Evolution for Diagnosis and Management of DengueDocumento35 páginasGuideline Evolution for Diagnosis and Management of DengueFrinciaAinda não há avaliações
- Vaginal Birth After CaesarianDocumento2 páginasVaginal Birth After CaesarianNina FauziaAinda não há avaliações
- Guideline Evolution for Diagnosis and Management of DengueDocumento35 páginasGuideline Evolution for Diagnosis and Management of DengueFrinciaAinda não há avaliações
- System Musculo Skeletal: Simbar SitepuDocumento22 páginasSystem Musculo Skeletal: Simbar SitepuFrinciaAinda não há avaliações
- Atopic Dermatitis and Erythema MultiformeDocumento2 páginasAtopic Dermatitis and Erythema MultiformeFrinciaAinda não há avaliações
- How Often Is A Low Apgar Score The ResultDocumento11 páginasHow Often Is A Low Apgar Score The ResultFrinciaAinda não há avaliações
- Risk Factors of Caesarean Section Due To CPD PDFDocumento7 páginasRisk Factors of Caesarean Section Due To CPD PDFFrinciaAinda não há avaliações
- GCS PDFDocumento1 páginaGCS PDFFrincia100% (1)
- Anorectal Malformation PDFDocumento13 páginasAnorectal Malformation PDFFrinciaAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Internship 3Documento4 páginasInternship 3Hirschmann Andro BoquilaAinda não há avaliações
- Ten Tips For First Year of RecoveryDocumento5 páginasTen Tips For First Year of RecoveryTratament DependenteAinda não há avaliações
- RGUHS Nursing Dissertation Titles 2015Documento7 páginasRGUHS Nursing Dissertation Titles 2015Vanitha Urubailu100% (11)
- Hong Kong Rehabilitation Programme Plan ReviewDocumento121 páginasHong Kong Rehabilitation Programme Plan Reviewbeck827Ainda não há avaliações
- Cucurmin and Fennel For Parasite Infection, Cancer, Lugols EnemasDocumento4 páginasCucurmin and Fennel For Parasite Infection, Cancer, Lugols Enemaspaulxe100% (1)
- Clinician's Guide To ADHD Comorbidities in Children and Adolescents Case Studies 2019 PDFDocumento148 páginasClinician's Guide To ADHD Comorbidities in Children and Adolescents Case Studies 2019 PDFfadel bilondatu100% (3)
- The U&ME-A Programme Sounds Like It Might Be A Fit For My Needs. What Next?Documento2 páginasThe U&ME-A Programme Sounds Like It Might Be A Fit For My Needs. What Next?Georgie SAinda não há avaliações
- Zambia National Formulary Committee RecommendationsDocumento344 páginasZambia National Formulary Committee RecommendationsHampson MalekanoAinda não há avaliações
- TM S Fusion Device Trabecular Metal Technology Cervical Solutions Surgical Technique GuideDocumento24 páginasTM S Fusion Device Trabecular Metal Technology Cervical Solutions Surgical Technique GuideTiến Khổng MinhAinda não há avaliações
- Evaluating Lawyer-Client Communication with International Research ProjectDocumento29 páginasEvaluating Lawyer-Client Communication with International Research ProjectabctandonAinda não há avaliações
- ECG Recording RulesDocumento11 páginasECG Recording RuleszorgglubAinda não há avaliações
- Guide To Med Device ClassificationDocumento15 páginasGuide To Med Device ClassificationTracy TreacherAinda não há avaliações
- Abdominal Compartment SyndromeDocumento24 páginasAbdominal Compartment SyndromePrateek Vaswani100% (1)
- Mmpi Lampiran Manual InggrisDocumento75 páginasMmpi Lampiran Manual Inggriskris100% (4)
- Picot Presntation 2Documento18 páginasPicot Presntation 2api-650274498Ainda não há avaliações
- Fendo 13 967102Documento9 páginasFendo 13 967102Vilma Gladis Rios HilarioAinda não há avaliações
- NBS for Haemoglobinopathies in Najran RegionDocumento17 páginasNBS for Haemoglobinopathies in Najran RegionSaifeldein ElimamAinda não há avaliações
- Hiperakusis 2015Documento20 páginasHiperakusis 2015Abdur ShamilAinda não há avaliações
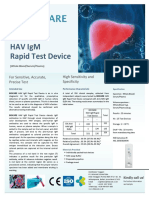
- Brosur BIOCARE HAV IgM Rapid Test Device OKDocumento1 páginaBrosur BIOCARE HAV IgM Rapid Test Device OKAlfarizi Julistyo S.Ainda não há avaliações
- Kidney Function and Electrolyte Test ResultsDocumento4 páginasKidney Function and Electrolyte Test ResultsBrix ValdrizAinda não há avaliações
- 11.multisystem Process Disorders 5 Blocks @eduwaves360Documento1.060 páginas11.multisystem Process Disorders 5 Blocks @eduwaves360AbigailAinda não há avaliações
- List of Empanelled (South)Documento14 páginasList of Empanelled (South)Ilam BaruthiAinda não há avaliações
- 6 Metronidazole Drug StudyDocumento4 páginas6 Metronidazole Drug Studyshadow gonzalezAinda não há avaliações
- Clinical Manual of Oriental Science PDFDocumento1.031 páginasClinical Manual of Oriental Science PDFlijke100% (2)
- Resultados de Búsqueda: Artículos Académicos para Vocal Function Exercises Stemple PDFDocumento3 páginasResultados de Búsqueda: Artículos Académicos para Vocal Function Exercises Stemple PDFleandro__scribdAinda não há avaliações
- Orthodontic Books CollectionDocumento4 páginasOrthodontic Books CollectionRamzi ghalipAinda não há avaliações
- Chronic PeriodontitisDocumento21 páginasChronic PeriodontitisPrathik RaiAinda não há avaliações
- Denial Codes 05aug2020Documento9 páginasDenial Codes 05aug2020naharmampillyAinda não há avaliações
- TG226 IGRT Commissioning PDFDocumento15 páginasTG226 IGRT Commissioning PDFmarkAinda não há avaliações
- Letter For Participation in Internship Manila CampusDocumento4 páginasLetter For Participation in Internship Manila CampusSEAN MELNOR LOSBAÑESAinda não há avaliações