Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Immunisation History Statement 3Documento2 páginasImmunisation History Statement 3Fordham JessAinda não há avaliações
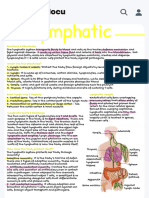
- Handwritten Lympathic - Functions & Structures The Lymphatic System Transports Fluids To Blood - StudocuDocumento1 páginaHandwritten Lympathic - Functions & Structures The Lymphatic System Transports Fluids To Blood - StudocuAllyssa MarieAinda não há avaliações
- Classification and General Properties of Medically Important HelminthesDocumento51 páginasClassification and General Properties of Medically Important HelminthesErdem AltunAinda não há avaliações
- Hiv AidsDocumento18 páginasHiv Aidskerema BadasaAinda não há avaliações
- Human Defence PDFDocumento13 páginasHuman Defence PDFDarrell CalabiaAinda não há avaliações
- TSA WinS Booklet Deworming PRINT 20181031Documento28 páginasTSA WinS Booklet Deworming PRINT 20181031GEORGIE GUMAWIAinda não há avaliações
- Mao Na NiDocumento15 páginasMao Na NiZe SubridaAinda não há avaliações
- Science - November 7, 2014Documento140 páginasScience - November 7, 2014Nicoleta Andreea TudoseAinda não há avaliações
- Immunization ScheduleDocumento2 páginasImmunization ScheduleTracy100% (1)
- Vaccination Exemption Pursuant To Wisconsin Statute 252.04Documento2 páginasVaccination Exemption Pursuant To Wisconsin Statute 252.04DonnaAinda não há avaliações
- Pediatric SmleDocumento59 páginasPediatric SmleMoayad Zeyad M100% (1)
- Acute Respiratory InfectionDocumento9 páginasAcute Respiratory InfectionStephen FoxAinda não há avaliações
- The Zombie FilesDocumento6 páginasThe Zombie FilesVincent TomasinoAinda não há avaliações
- Skin Diseases Affecting The VulvaDocumento7 páginasSkin Diseases Affecting The VulvaNoraAinda não há avaliações
- Bovine Viral Diarrhoea: BVD Is A Sub Acute, Acute or INAPPARENT Contagious Disease Characterized byDocumento27 páginasBovine Viral Diarrhoea: BVD Is A Sub Acute, Acute or INAPPARENT Contagious Disease Characterized byhari krishnaa athotaAinda não há avaliações
- CircumcisionDocumento8 páginasCircumcisionJoan Marie BelegaAinda não há avaliações
- Who Edl 2018 PDFDocumento30 páginasWho Edl 2018 PDFanggoenzAinda não há avaliações
- Renukaprasad Ys - Medicine - Thesis NewDocumento110 páginasRenukaprasad Ys - Medicine - Thesis NewLokesh ChopraAinda não há avaliações
- Student Exploration: Virus Lytic CycleDocumento5 páginasStudent Exploration: Virus Lytic CycleBryce Mattox100% (1)
- S87 - Sector-12 Sonipat-Cc Shop No 25, Mainmarket Sec-12 (Part-2) Sonipat-131001, Mob No:-09812905359Documento2 páginasS87 - Sector-12 Sonipat-Cc Shop No 25, Mainmarket Sec-12 (Part-2) Sonipat-131001, Mob No:-09812905359Dhruv KuchhalAinda não há avaliações
- Drug StudyDocumento7 páginasDrug StudyJoseph Angelo Fortuna CarmonaAinda não há avaliações
- Yellow Fever Brochure PubDocumento2 páginasYellow Fever Brochure Pubapi-358102097Ainda não há avaliações
- A. Photoorganotrophs: MCU-FDT Medical Foundation Department of Microbiology and Parasitology College of MedicineDocumento12 páginasA. Photoorganotrophs: MCU-FDT Medical Foundation Department of Microbiology and Parasitology College of MedicineJo Anne100% (2)
- Novel Drugs Targeting The Sars-Cov-2/Covid-19 Machinery: Ariane Sternberg, Dwight L. Mckee and Cord NaujokatDocumento11 páginasNovel Drugs Targeting The Sars-Cov-2/Covid-19 Machinery: Ariane Sternberg, Dwight L. Mckee and Cord Naujokatperi umardianaAinda não há avaliações
- 2021 - l4 Medical Bacteriology - Gram Negative Bacteria (I)Documento52 páginas2021 - l4 Medical Bacteriology - Gram Negative Bacteria (I)Tonny YuliantoAinda não há avaliações
- Babesia MicrotiDocumento9 páginasBabesia MicrotiFrancene Ac-DaAinda não há avaliações
- Pathology 4.05 Liver Pathology - Dr. YanezDocumento22 páginasPathology 4.05 Liver Pathology - Dr. YanezDranreb Berylle MasangkayAinda não há avaliações
- Intestinal NematodesDocumento72 páginasIntestinal Nematodessarguss14100% (6)
- Cholera PresentationDocumento10 páginasCholera PresentationjaniAinda não há avaliações
- 2013 Book EpigeneticsDevelopmentAndDisea PDFDocumento698 páginas2013 Book EpigeneticsDevelopmentAndDisea PDFSuelen Lima de Matos100% (1)