Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Dementia in Clinical Practice PDFDocumento404 páginasDementia in Clinical Practice PDFadriricalde100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Art:10.1007/s00455 016 9773 ZDocumento12 páginasArt:10.1007/s00455 016 9773 ZadriricaldeAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Fpsyg 07 01471Documento15 páginasFpsyg 07 01471adriricaldeAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- Sellers Et Al-2014-Developmental Medicine & Child NeurologyDocumento7 páginasSellers Et Al-2014-Developmental Medicine & Child NeurologyadriricaldeAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- English Et Al-2009-Developmental Disabilities Research ReviewsDocumento7 páginasEnglish Et Al-2009-Developmental Disabilities Research ReviewsadriricaldeAinda não há avaliações
- Tinnitus Current Understanding and Contemporary ManagementDocumento6 páginasTinnitus Current Understanding and Contemporary ManagementadriricaldeAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Art:10 1007/BF00706692Documento8 páginasArt:10 1007/BF00706692adriricaldeAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- AAA - 2010 - Diagnosis Treatment and Management of Children and Adults With Central Auditory Processing Disroder-AnnotatedDocumento51 páginasAAA - 2010 - Diagnosis Treatment and Management of Children and Adults With Central Auditory Processing Disroder-AnnotatedadriricaldeAinda não há avaliações
- 1 s2.0 S0093934X16300116 MainDocumento10 páginas1 s2.0 S0093934X16300116 MainadriricaldeAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- Myelomeningocele: How We Can Improve The Assessment of The Most Severe Form of Spina Bi FidaDocumento7 páginasMyelomeningocele: How We Can Improve The Assessment of The Most Severe Form of Spina Bi FidaadriricaldeAinda não há avaliações
- 1 s2.0 S0030666516300469 MainDocumento10 páginas1 s2.0 S0030666516300469 MainadriricaldeAinda não há avaliações
- Au Et Al-2010-Developmental Disabilities Research ReviewsDocumento10 páginasAu Et Al-2010-Developmental Disabilities Research ReviewsadriricaldeAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Using The Language CharacteristicsDocumento23 páginasUsing The Language CharacteristicsadriricaldeAinda não há avaliações
- Velopharyngeal Insufficiency Diagnosis and ManagementDocumento6 páginasVelopharyngeal Insufficiency Diagnosis and ManagementadriricaldeAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Delayed Developmental Language Milestones in Children With Duchenne's Muscular Dystrophy PDFDocumento5 páginasDelayed Developmental Language Milestones in Children With Duchenne's Muscular Dystrophy PDFadriricaldeAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Bilateral Vestibulopathy PDFDocumento6 páginasBilateral Vestibulopathy PDFadriricaldeAinda não há avaliações
- Structural Tympanic Membrane Changes in OMC and Cholesteatoma PDFDocumento6 páginasStructural Tympanic Membrane Changes in OMC and Cholesteatoma PDFadriricaldeAinda não há avaliações
- Abnormal Language Pathway in Children With Angelman SyndromeDocumento7 páginasAbnormal Language Pathway in Children With Angelman SyndromeadriricaldeAinda não há avaliações
- Cochlear OtosclerosisDocumento6 páginasCochlear OtosclerosisadriricaldeAinda não há avaliações
- Language and Eating Problems in Children PDFDocumento10 páginasLanguage and Eating Problems in Children PDFadriricaldeAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Cochlear Efferent Innervation and FunctionDocumento7 páginasCochlear Efferent Innervation and FunctionadriricaldeAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- Otolaryngology Head and Neck Surgery 2014 Wegner 201 7Documento7 páginasOtolaryngology Head and Neck Surgery 2014 Wegner 201 7adriricaldeAinda não há avaliações
- Auditory Development in Early Amplified ChildrenDocumento20 páginasAuditory Development in Early Amplified ChildrenadriricaldeAinda não há avaliações
- Feeding Disorders in ChildrenDocumento16 páginasFeeding Disorders in ChildrenadriricaldeAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- TalamoDocumento7 páginasTalamoDanya RoblesAinda não há avaliações
- Oromotor Variability in Children With Mild Pci PDFDocumento10 páginasOromotor Variability in Children With Mild Pci PDFadriricaldeAinda não há avaliações
- Otolaryngology Head and Neck Surgery 2014 Dorresteijn 919 24Documento6 páginasOtolaryngology Head and Neck Surgery 2014 Dorresteijn 919 24adriricaldeAinda não há avaliações
- Auris Nasus Larynx: Kimitaka KagaDocumento11 páginasAuris Nasus Larynx: Kimitaka KagaadriricaldeAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Seminars in Fetal & Neonatal Medicine: Cristen Olds, John S. OghalaiDocumento5 páginasSeminars in Fetal & Neonatal Medicine: Cristen Olds, John S. OghalaiadriricaldeAinda não há avaliações
- 0418 w08 QP 1Documento17 páginas0418 w08 QP 1pmvarshaAinda não há avaliações
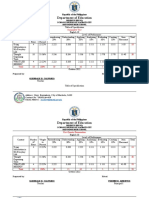
- Table of Specification ENGLISHDocumento2 páginasTable of Specification ENGLISHDonn Abel Aguilar IsturisAinda não há avaliações
- Carnot CycleDocumento3 páginasCarnot CyclealexontingAinda não há avaliações
- Lenovo IdeaPad U350 UserGuide V1.0Documento138 páginasLenovo IdeaPad U350 UserGuide V1.0Marc BengtssonAinda não há avaliações
- Math Curriculum Overview Grades 1 8Documento1 páginaMath Curriculum Overview Grades 1 8GuiselleAinda não há avaliações
- Conclusion For A Research Paper About BullyingDocumento7 páginasConclusion For A Research Paper About Bullyingafnkjuvgzjzrgl100% (3)
- Imports System - data.SqlClient Imports System - Data Imports System PartialDocumento2 páginasImports System - data.SqlClient Imports System - Data Imports System PartialStuart_Lonnon_1068Ainda não há avaliações
- ASTM C 136 Sieve Analysis of Fine and Coarse Aggregates (D)Documento5 páginasASTM C 136 Sieve Analysis of Fine and Coarse Aggregates (D)Yasir DharejoAinda não há avaliações
- Rolfsen Knot Table Guide Crossings 1-10Documento4 páginasRolfsen Knot Table Guide Crossings 1-10Pangloss LeibnizAinda não há avaliações
- Key Note Units 3-4Documento4 páginasKey Note Units 3-4Javier BahenaAinda não há avaliações
- C code snippets with answersDocumento14 páginasC code snippets with answersqwerty6327Ainda não há avaliações
- Identifying Research ProblemsDocumento29 páginasIdentifying Research ProblemsEdel Borden PaclianAinda não há avaliações
- A Personality Trait-Based Interactionist Model of Job PerformanceDocumento18 páginasA Personality Trait-Based Interactionist Model of Job PerformanceAlvina AhmedAinda não há avaliações
- Laser Plasma Accelerators PDFDocumento12 páginasLaser Plasma Accelerators PDFAjit UpadhyayAinda não há avaliações
- User Manual: Swift S3Documento97 páginasUser Manual: Swift S3smnguyenAinda não há avaliações
- Navier-Stokes EquationsDocumento395 páginasNavier-Stokes EquationsBouhadjar Meguenni100% (7)
- Sprite Graphics For The Commodore 64Documento200 páginasSprite Graphics For The Commodore 64scottmac67Ainda não há avaliações
- SYS600 - Visual SCIL Application DesignDocumento144 páginasSYS600 - Visual SCIL Application DesignDang JinlongAinda não há avaliações
- Páginas Desdeingles - Sep2008Documento1 páginaPáginas Desdeingles - Sep2008anayourteacher100% (1)
- Activity Emcee Mid-Year INSET 2021Documento3 páginasActivity Emcee Mid-Year INSET 2021Abegail A. Alangue-Calimag67% (6)
- 07CRMDocumento81 páginas07CRMsangramlifeAinda não há avaliações
- 4idealism Realism and Pragmatigsm in EducationDocumento41 páginas4idealism Realism and Pragmatigsm in EducationGaiLe Ann100% (1)
- What Is Science Cornell Notes ExampleDocumento3 páginasWhat Is Science Cornell Notes Exampleapi-240096234Ainda não há avaliações
- Literary Text Analysis WorksheetDocumento1 páginaLiterary Text Analysis Worksheetapi-403444340Ainda não há avaliações
- Mitchell 1986Documento34 páginasMitchell 1986Sara Veronica Florentin CuencaAinda não há avaliações
- New Microsoft Word DocumentDocumento5 páginasNew Microsoft Word DocumentxandercageAinda não há avaliações
- Assignment2-9509Documento5 páginasAssignment2-9509ritadhikarycseAinda não há avaliações
- Receiving Welcoming and Greeting of GuestDocumento18 páginasReceiving Welcoming and Greeting of GuestMarwa KorkabAinda não há avaliações
- Humanities Unit Plan Plus Lesson PlansDocumento12 páginasHumanities Unit Plan Plus Lesson Plansapi-298200210Ainda não há avaliações
- Discourse Community 2Documento7 páginasDiscourse Community 2api-272763663Ainda não há avaliações
- The Age of Magical Overthinking: Notes on Modern IrrationalityNo EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityNota: 4 de 5 estrelas4/5 (13)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNota: 5 de 5 estrelas5/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityNo EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityNota: 3.5 de 5 estrelas3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNo EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNota: 3.5 de 5 estrelas3.5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNo EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNota: 4 de 5 estrelas4/5 (402)