Você também pode gostar
- Cephalometric VTODocumento4 páginasCephalometric VTOedmoses4Ainda não há avaliações
- Orthodontics in the Vertical Dimension: A Case-Based ReviewNo EverandOrthodontics in the Vertical Dimension: A Case-Based ReviewAinda não há avaliações
- Interceptive Orthodontics: A Practical Guide to Occlusal ManagementNo EverandInterceptive Orthodontics: A Practical Guide to Occlusal ManagementAinda não há avaliações
- Maxillary Protraction / Orthodontic Courses by Indian Dental AcademyDocumento86 páginasMaxillary Protraction / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Various Intrusive ArchsDocumento10 páginasVarious Intrusive ArchsmutansAinda não há avaliações
- Biomechanics of Deep Bite TreatmentDocumento66 páginasBiomechanics of Deep Bite TreatmentMaitreye PriyadarshiniAinda não há avaliações
- Tweed - A Philosophy of Orthodontic TreatmentDocumento30 páginasTweed - A Philosophy of Orthodontic TreatmentriofrankfurtAinda não há avaliações
- Fixed Orthodontic Appliances: A Practical GuideNo EverandFixed Orthodontic Appliances: A Practical GuideNota: 1 de 5 estrelas1/5 (1)
- Twin BlockDocumento130 páginasTwin BlockRolando GamarraAinda não há avaliações
- Scissors Bite-Dragon Helix ApplianceDocumento6 páginasScissors Bite-Dragon Helix ApplianceGaurav PatelAinda não há avaliações
- American Journal QF Orthodontics: Facial Types Associated With Class II MalocclusionsDocumento18 páginasAmerican Journal QF Orthodontics: Facial Types Associated With Class II MalocclusionsKhyati Gupta100% (1)
- Extraction Vs Non Extraction Controversy: A Review: January 2018Documento9 páginasExtraction Vs Non Extraction Controversy: A Review: January 2018Jawad TariqAinda não há avaliações
- Skeletal Anchorage Systems in Orthodontics Absolute Anchorage Adream or RealityDocumento10 páginasSkeletal Anchorage Systems in Orthodontics Absolute Anchorage Adream or RealitySoe San KyawAinda não há avaliações
- Static Equilibrium and It's Importance - Mulligan-2 PDFDocumento14 páginasStatic Equilibrium and It's Importance - Mulligan-2 PDFdrzana78Ainda não há avaliações
- "Cephalometrics Is The Language in Which The Poetry of Orthodontic Diagnosis and Treatment Planning Is Written" - Cecil SteinerDocumento97 páginas"Cephalometrics Is The Language in Which The Poetry of Orthodontic Diagnosis and Treatment Planning Is Written" - Cecil Steinersanjay100% (1)
- Functional ApplianceHGHDFGDocumento40 páginasFunctional ApplianceHGHDFGmustafa_tambawalaAinda não há avaliações
- Bolton Analysis According To ABODocumento54 páginasBolton Analysis According To ABOkerminkAinda não há avaliações
- 1947 Howes CASE ANALYSIS AND TREATMENT PLANNING BASED UPON THE Relationship of Tooth Material To Its Supporting BoneDocumento35 páginas1947 Howes CASE ANALYSIS AND TREATMENT PLANNING BASED UPON THE Relationship of Tooth Material To Its Supporting BoneRockey ShrivastavaAinda não há avaliações
- Extractions in Orthodontics: An UpdateDocumento10 páginasExtractions in Orthodontics: An Updatedrzana78100% (1)
- Intrusion Arches ShinuDocumento66 páginasIntrusion Arches ShinuYuvashreeAinda não há avaliações
- Roth Vs MBT PDFDocumento8 páginasRoth Vs MBT PDFandiiperezAinda não há avaliações
- The Extraction Debate of 1911 by Case Dewey and Cryer 1964Documento13 páginasThe Extraction Debate of 1911 by Case Dewey and Cryer 1964SwathiLingannagariAinda não há avaliações
- Arch Forms 1-Ortho / Orthodontic Courses by Indian Dental AcademyDocumento48 páginasArch Forms 1-Ortho / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Cannon BracketsDocumento92 páginasCannon BracketsSzenyes Szabolcs0% (1)
- Tweed AJO 1946 - The Frankfort Mandibular Plane Angle in Orthodontic Diagnosis, Classification, Treatment Planning and PrognosisDocumento56 páginasTweed AJO 1946 - The Frankfort Mandibular Plane Angle in Orthodontic Diagnosis, Classification, Treatment Planning and PrognosisAnonymous 1uVifBp6100% (1)
- Biomechanics of Deep Overbite CorrectionDocumento8 páginasBiomechanics of Deep Overbite CorrectionLuis Paipay SantosAinda não há avaliações
- V-Bend and Anchorage in Orthodontics: Mehak Arya Iyrmds Dept of OrthodonticsDocumento37 páginasV-Bend and Anchorage in Orthodontics: Mehak Arya Iyrmds Dept of OrthodonticsMehak AryaAinda não há avaliações
- Understanding Masticatory Function in Unilateral CrossbitesNo EverandUnderstanding Masticatory Function in Unilateral CrossbitesAinda não há avaliações
- A Beginner's Guide To Surgical Treatment Objective: An Orthodontist's Point of ViewDocumento5 páginasA Beginner's Guide To Surgical Treatment Objective: An Orthodontist's Point of ViewNguyễn QuỳnhAinda não há avaliações
- 9-Miniscrews in Orthodontics Biomechanics-Case Report-Oussama Sandid - Mohamad Aboualnaser-Awatef Shaar-Miniscrews Mini-Implant en Orthodontie PDFDocumento19 páginas9-Miniscrews in Orthodontics Biomechanics-Case Report-Oussama Sandid - Mohamad Aboualnaser-Awatef Shaar-Miniscrews Mini-Implant en Orthodontie PDFAnonymous oD9H6T8p100% (1)
- BoltonDocumento26 páginasBoltonDryashpal SinghAinda não há avaliações
- Cephalometrics Manual KrothDocumento124 páginasCephalometrics Manual Krothimtiyazorthodontist100% (3)
- Orthodontics Treatment For TMD JournalDocumento19 páginasOrthodontics Treatment For TMD JournalEndang SetiowatiAinda não há avaliações
- Diagnosis and Treatment PlanningDocumento93 páginasDiagnosis and Treatment PlanningVikkii VeerakumarAinda não há avaliações
- Treatment Timing For Rapid Maxillary ExpansionDocumento8 páginasTreatment Timing For Rapid Maxillary Expansiongriffone1Ainda não há avaliações
- Evolution of Treatment Mechanics PDFDocumento9 páginasEvolution of Treatment Mechanics PDFJunaid Israr - OrthodonticsAinda não há avaliações
- MBT Product CatalogDocumento55 páginasMBT Product CatalogkirmaniAinda não há avaliações
- The Midline Diagnosis and Treatment ARTUROCAMACHODocumento10 páginasThe Midline Diagnosis and Treatment ARTUROCAMACHOMiguel AngelAinda não há avaliações
- Seminars in OrthodonticsDocumento3 páginasSeminars in Orthodonticsgriffone1Ainda não há avaliações
- Growth PredictionDocumento101 páginasGrowth PredictionVartika TripathiAinda não há avaliações
- Prevent Incisor Flaring in Fixed Functional ApplianceDocumento2 páginasPrevent Incisor Flaring in Fixed Functional ApplianceCyriac JohnAinda não há avaliações
- Open-Bite Malocclusion: Treatment and StabilityNo EverandOpen-Bite Malocclusion: Treatment and StabilityGuilherme JansonNota: 5 de 5 estrelas5/5 (1)
- Cone Beam Tomography in Orthodontics PDFDocumento8 páginasCone Beam Tomography in Orthodontics PDFdruzair007Ainda não há avaliações
- Mixed DentitionDocumento49 páginasMixed Dentitiongnna norAinda não há avaliações
- Jiang T 2019Documento9 páginasJiang T 2019CLAUDIA PATRICIA ROSALES BASANTEAinda não há avaliações
- Max Arch Distalization Tads'Documento9 páginasMax Arch Distalization Tads'Rohini TondaAinda não há avaliações
- Maxillary Protraction Dr.M.M.varadharaja / Orthodontic Courses by Indian Dental AcademyDocumento121 páginasMaxillary Protraction Dr.M.M.varadharaja / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Biostatistics in OrthodonticsDocumento117 páginasBiostatistics in OrthodonticsJoshua StalinAinda não há avaliações
- Timing in Orthodontics PDFDocumento5 páginasTiming in Orthodontics PDFdrzana78Ainda não há avaliações
- 12 Finishing and DetailingDocumento92 páginas12 Finishing and Detailingtanmayi minniAinda não há avaliações
- Functional Occlusion in Orthodontics: ClinicalDocumento11 páginasFunctional Occlusion in Orthodontics: ClinicalNaeem MoollaAinda não há avaliações
- Roth Versus MBTDocumento23 páginasRoth Versus MBTJose Antonio Figuroa AbadoAinda não há avaliações
- Fudamentals of Biomechanics and Biomechanics of Levelling and Aligning Includes Biomechanics of Molar Control PDFDocumento326 páginasFudamentals of Biomechanics and Biomechanics of Levelling and Aligning Includes Biomechanics of Molar Control PDFVioleta PajicAinda não há avaliações
- Rickett'S: Visual Treatment Objective (V.T.O)Documento4 páginasRickett'S: Visual Treatment Objective (V.T.O)MariyamAinda não há avaliações
- Bioprogressive Therapy As An AnswerDocumento39 páginasBioprogressive Therapy As An Answerelenaelena2011Ainda não há avaliações
- CORP Sample SassouniDocumento5 páginasCORP Sample SassouniFisaAinda não há avaliações
- A Cephalometric Study of The HawaiianDocumento16 páginasA Cephalometric Study of The HawaiianIvanna H. A.Ainda não há avaliações
- Analysus of The Soft Tissue Profile in Croatians With Normal Occlusions and Well-Balanced FacesDocumento6 páginasAnalysus of The Soft Tissue Profile in Croatians With Normal Occlusions and Well-Balanced FacesIvanna H. A.Ainda não há avaliações
- 2013 SB Course BrochureDocumento8 páginas2013 SB Course BrochureIvanna H. A.Ainda não há avaliações
- Cephalometric Features of Filipinos With Angle Class I Oclussion According To The Munich AnalysisDocumento6 páginasCephalometric Features of Filipinos With Angle Class I Oclussion According To The Munich AnalysisIvanna H. A.Ainda não há avaliações
- A Comparative Study of Southern Chinese and BritishDocumento8 páginasA Comparative Study of Southern Chinese and BritishIvanna H. A.Ainda não há avaliações
- 2013 SB Course BrochureDocumento8 páginas2013 SB Course BrochureIvanna H. A.Ainda não há avaliações
- Racial Variations in Cephalometric Analysis Between Whites and KuwaitsDocumento6 páginasRacial Variations in Cephalometric Analysis Between Whites and KuwaitsIvanna H. A.Ainda não há avaliações
- Ethinic Differences in Teh Soft Tissue Profile of Korean and European American Adults With Normal Oclusions and Well Balanced FacesDocumento9 páginasEthinic Differences in Teh Soft Tissue Profile of Korean and European American Adults With Normal Oclusions and Well Balanced FacesIvanna H. A.Ainda não há avaliações
- Analysus of The Soft Tissue Profile in Croatians With Normal Occlusions and Well-Balanced FacesDocumento6 páginasAnalysus of The Soft Tissue Profile in Croatians With Normal Occlusions and Well-Balanced FacesIvanna H. A.Ainda não há avaliações
- Linear and Angular Filipo Cephalometric Norms According To Age and SexDocumento6 páginasLinear and Angular Filipo Cephalometric Norms According To Age and SexIvanna H. A.Ainda não há avaliações
- Israeli Cephalometric Standards Compared To Downs and SteinerDocumento7 páginasIsraeli Cephalometric Standards Compared To Downs and SteinerIvanna H. A.Ainda não há avaliações
- Aoos 17 1 Noroozi6Documento3 páginasAoos 17 1 Noroozi6Ivanna H. A.Ainda não há avaliações
- Chinese Norms of Mcnamara Cephalometric AnalysisDocumento9 páginasChinese Norms of Mcnamara Cephalometric AnalysisIvanna H. A.Ainda não há avaliações
- Selected Cedphalometric Angular Norms in Kikuyo ChildrenDocumento6 páginasSelected Cedphalometric Angular Norms in Kikuyo ChildrenIvanna H. A.Ainda não há avaliações
- Anthony A GianellyDocumento2 páginasAnthony A GianellyIvanna H. A.Ainda não há avaliações
- Written Examination GuideDocumento17 páginasWritten Examination GuideIvanna H. A.Ainda não há avaliações
- Cephalometric Norms For Saudi Adults Living in The Western Region of Saudi ArabiaDocumento5 páginasCephalometric Norms For Saudi Adults Living in The Western Region of Saudi ArabiaIvanna H. A.Ainda não há avaliações
- Long Term Effectiveness of The Continuous and The Sectional Archwire Techniques in Leveling The Curve of SpeeDocumento6 páginasLong Term Effectiveness of The Continuous and The Sectional Archwire Techniques in Leveling The Curve of SpeeIvanna H. A.Ainda não há avaliações
- Long Term Effectiveness of The Continuous and The Sectional Archwire Techniques in Leveling The Curve of SpeeDocumento6 páginasLong Term Effectiveness of The Continuous and The Sectional Archwire Techniques in Leveling The Curve of SpeeIvanna H. A.Ainda não há avaliações
- Torque Expression in Stainless Steel Orthodontic BracketsDocumento10 páginasTorque Expression in Stainless Steel Orthodontic BracketspingapeluaAinda não há avaliações
- 6008 21106 1 PBDocumento8 páginas6008 21106 1 PBIvanna H. A.Ainda não há avaliações
- Orthodontics Pgi: Goals: This Series of Lectures Should Enable The Resident ToDocumento4 páginasOrthodontics Pgi: Goals: This Series of Lectures Should Enable The Resident ToIvanna H. A.Ainda não há avaliações
- 0022 enDocumento8 páginas0022 enIvanna H. A.Ainda não há avaliações
- Current Topics and Controversies Presented by DR Anthony GianellyDocumento2 páginasCurrent Topics and Controversies Presented by DR Anthony GianellyIvanna H. A.Ainda não há avaliações
- JCO Content Aug2005Documento1 páginaJCO Content Aug2005Ivanna H. A.Ainda não há avaliações
- Article 5Documento2 páginasArticle 5Ivanna H. A.Ainda não há avaliações
- Extraction Vs NonextractionDocumento5 páginasExtraction Vs NonextractionIvanna H. A.Ainda não há avaliações
- Orthodontic Anchorage A Systematic ReviewDocumento9 páginasOrthodontic Anchorage A Systematic ReviewIvanna H. A.Ainda não há avaliações
- Anchorage Control in Bioprogressive Vs Straight Wire TreatmentDocumento6 páginasAnchorage Control in Bioprogressive Vs Straight Wire TreatmentIvanna H. A.Ainda não há avaliações
- M&E Training ManualDocumento45 páginasM&E Training Manualsheittie100% (1)
- 2021 重症核心課程CRRT Dose and Prescription-NEW Ver1.0Documento63 páginas2021 重症核心課程CRRT Dose and Prescription-NEW Ver1.0Andy DazAinda não há avaliações
- The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5)Documento42 páginasThe Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5)Mihaela Onisia UngureanuAinda não há avaliações
- Adnexal Torsion: Clinical, Radiological and Pathological Characteristics in A Tertiary Care Centre in Southern IndiaDocumento6 páginasAdnexal Torsion: Clinical, Radiological and Pathological Characteristics in A Tertiary Care Centre in Southern IndiaKriti KumariAinda não há avaliações
- GroveX Reviews (#FDA APPROVED) - #2023 Unexpected Details Revealed - !Documento1 páginaGroveX Reviews (#FDA APPROVED) - #2023 Unexpected Details Revealed - !GroveX boostAinda não há avaliações
- Therapeutic Controversies: Antmi Yric Prophylaxis in Cesarean SectionDocumento6 páginasTherapeutic Controversies: Antmi Yric Prophylaxis in Cesarean Sectionnurul wahyuniAinda não há avaliações
- RF LatexDocumento1 páginaRF LatexDinesh SreedharanAinda não há avaliações
- Nursing Care Plan Surgical PDFDocumento2 páginasNursing Care Plan Surgical PDFDanielle Audrey100% (2)
- SirkulasiDocumento17 páginasSirkulasiJessica VanyaAinda não há avaliações
- Antimicrobials Q BanksDocumento65 páginasAntimicrobials Q Banksduy luuAinda não há avaliações
- Tuansi-Pa ManuscriptDocumento11 páginasTuansi-Pa Manuscriptallkhusairy6tuansiAinda não há avaliações
- 001 Diagnosis of Neurological DiseaseDocumento7 páginas001 Diagnosis of Neurological DiseasemgvbAinda não há avaliações
- An Ethnobotanical Survey of Medicinal Plants Used in Terai Forest of Western NepalDocumento15 páginasAn Ethnobotanical Survey of Medicinal Plants Used in Terai Forest of Western NepalLeandro DouglasAinda não há avaliações
- Stroke AHA GuidelinesDocumento104 páginasStroke AHA GuidelinesCristina ZeamaAinda não há avaliações
- Manchester Anaemia GuideDocumento13 páginasManchester Anaemia Guidemubzy14Ainda não há avaliações
- Tle 7 - 8 - FisheryDocumento17 páginasTle 7 - 8 - FisheryRey JavierAinda não há avaliações
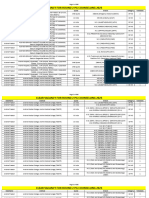
- Clear Vacancy R2Documento696 páginasClear Vacancy R2bhuviAinda não há avaliações
- Task 2 Engineering English (Redho Triwinoko, METO 5B)Documento3 páginasTask 2 Engineering English (Redho Triwinoko, METO 5B)Redho TriwinokoAinda não há avaliações
- Region: Arum TriphyllumDocumento3 páginasRegion: Arum TriphyllumKamalAinda não há avaliações
- Drug Facts: Aleve TabletsDocumento2 páginasDrug Facts: Aleve TabletsBima AstawaAinda não há avaliações
- Ocular Fundus DrawingDocumento33 páginasOcular Fundus DrawingguhanAinda não há avaliações
- Understanding and Using Sensitivity, Specificity and Predictive ValuesDocumento13 páginasUnderstanding and Using Sensitivity, Specificity and Predictive ValuesHaris PrayitnoAinda não há avaliações
- Ebook Cohens Pathways of The Pulp 12Th Edition PDF Full Chapter PDFDocumento67 páginasEbook Cohens Pathways of The Pulp 12Th Edition PDF Full Chapter PDFchristopher.jenkins207100% (27)
- 1 s2.0 S0895435615000141 MainDocumento10 páginas1 s2.0 S0895435615000141 MainBarron ManAinda não há avaliações
- COVID-19 Prevention & IEC Committee, PGIMER Chandigarh: Tentative Webinar Schedule For Healthcare ProfessionalsDocumento3 páginasCOVID-19 Prevention & IEC Committee, PGIMER Chandigarh: Tentative Webinar Schedule For Healthcare Professionalsvarshasharma05Ainda não há avaliações
- Cancer and Oncology Nursing NCLEX Practice Quiz ANSDocumento5 páginasCancer and Oncology Nursing NCLEX Practice Quiz ANSyanyan cadizAinda não há avaliações
- 1 - Chapter 1 of Your Textbook Describes The Purposes of Nursing ResearDocumento4 páginas1 - Chapter 1 of Your Textbook Describes The Purposes of Nursing ResearHelping TutorsAinda não há avaliações
- Musculoskeletal SystemDocumento46 páginasMusculoskeletal Systemapi-87967494100% (1)
- UnaniDocumento16 páginasUnaniRahul Banik888Ainda não há avaliações
- 2019E 14 - Supportive Care and Managment of Side EffectsDocumento82 páginas2019E 14 - Supportive Care and Managment of Side Effectsrusgal8992Ainda não há avaliações