Você também pode gostar
- Surgical Site MarkingDocumento12 páginasSurgical Site Markingh1m4w4nAinda não há avaliações
- Sop Number Title of SOP Author Consultation With StakeholdersDocumento23 páginasSop Number Title of SOP Author Consultation With StakeholdersMr. BamsAinda não há avaliações
- PPG GDCH Nur 44 Effective Communication Read Back OrderDocumento5 páginasPPG GDCH Nur 44 Effective Communication Read Back OrderKenny JosefAinda não há avaliações
- Operational Guidelines For Clients' Rights and Providers' Rights-DutiesDocumento34 páginasOperational Guidelines For Clients' Rights and Providers' Rights-DutiesVichhai100% (1)
- Day Case For WebDocumento34 páginasDay Case For WebDavid CruzAinda não há avaliações
- Chest Drains GuidanceDocumento14 páginasChest Drains Guidancenob2011nobAinda não há avaliações
- Be at Ease ChecklistDocumento2 páginasBe at Ease ChecklistDaniel Henderson100% (1)
- Ventilator, Weaning, SuctioningDocumento81 páginasVentilator, Weaning, SuctioningwaqarAinda não há avaliações
- Orthopaedic Nursing NSC 538: A.A Ogunlade Nursing Science Dept EUIDocumento10 páginasOrthopaedic Nursing NSC 538: A.A Ogunlade Nursing Science Dept EUIHABEEB FASASI100% (1)
- Vaishali Syal Moderator - Prof. J. R. ThakurDocumento34 páginasVaishali Syal Moderator - Prof. J. R. ThakurTasha NurfitrianiAinda não há avaliações
- 1 Infection Control and Universal PrecautionDocumento39 páginas1 Infection Control and Universal PrecautionHarshaWakodkarAinda não há avaliações
- IHOP - 9.13.25 - Time Out Universal Protocol For Invasive and Surgical ProceduresDocumento3 páginasIHOP - 9.13.25 - Time Out Universal Protocol For Invasive and Surgical Proceduresmaxxer1985Ainda não há avaliações
- Chapter 2 HandwashingDocumento18 páginasChapter 2 HandwashingMylene Valdez50% (2)
- Surgical Site Marking PolicyDocumento11 páginasSurgical Site Marking PolicymiraAinda não há avaliações
- Hospital Disclosure PolicyDocumento10 páginasHospital Disclosure Policyvks7876Ainda não há avaliações
- 16 Procedure On Destruction of Medical RecordsDocumento4 páginas16 Procedure On Destruction of Medical RecordsSanjay KadamAinda não há avaliações
- Operating Room Care of The Surgical Patient: Teaching PlanDocumento9 páginasOperating Room Care of The Surgical Patient: Teaching PlanscribdnijoizAinda não há avaliações
- The Intraoperative Patient: by Lisa M. Dunn RN, MSN/ED, CCRNDocumento52 páginasThe Intraoperative Patient: by Lisa M. Dunn RN, MSN/ED, CCRNrahmaya100% (1)
- Sputum CollectionDocumento4 páginasSputum CollectionBELIGANIO JOHANNAAinda não há avaliações
- Wee Bag, Nebulization, and Oxygen Therapy ChecklistDocumento2 páginasWee Bag, Nebulization, and Oxygen Therapy Checklistapril marquesesAinda não há avaliações
- SuctioningDocumento12 páginasSuctioningHannah Clarissa Faith AguilarAinda não há avaliações
- Complications of Urinary Bladder Catheters and Preventive Strategies - UpToDateDocumento8 páginasComplications of Urinary Bladder Catheters and Preventive Strategies - UpToDateJose Antonio Solis ChipaAinda não há avaliações
- Day Surgery Update 2019Documento15 páginasDay Surgery Update 2019O Mei NeilAinda não há avaliações
- Hand Hygiene Why How and When BrochureDocumento7 páginasHand Hygiene Why How and When BrochureWill JoshAinda não há avaliações
- ReportDocumento60 páginasReportNikky Rossel Flores100% (1)
- Wound Care Gopi SirDocumento110 páginasWound Care Gopi SirArvind ShenoyAinda não há avaliações
- Contrast and Special Radiographic Procedures: Topic - Aseptic TechniquesDocumento15 páginasContrast and Special Radiographic Procedures: Topic - Aseptic TechniquesPOOJA MAinda não há avaliações
- Blood Transfusions - TGH Policies & ProceduresDocumento4 páginasBlood Transfusions - TGH Policies & ProceduresMark Anthony FranciscoAinda não há avaliações
- NCM 103Documento48 páginasNCM 103Cheenapot BerberAinda não há avaliações
- (P1) BioethicsDocumento100 páginas(P1) BioethicsGeralyn KaeAinda não há avaliações
- Preparing The Sterile Field PPT June 2011Documento61 páginasPreparing The Sterile Field PPT June 2011gerard_xucnAinda não há avaliações
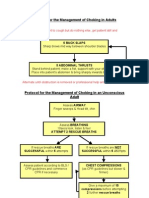
- Protocol For The Management of Choking in AdultsDocumento3 páginasProtocol For The Management of Choking in AdultsSarinah RynaAinda não há avaliações
- Aldrete Discharge Scoring - Appropriate For Post Anesthesia PhaseDocumento28 páginasAldrete Discharge Scoring - Appropriate For Post Anesthesia PhaseHeather PorterAinda não há avaliações
- Operating Theater ManagementDocumento5 páginasOperating Theater Managementtummalapalli venkateswara raoAinda não há avaliações
- 2007 International Patient Safety GoalsDocumento1 página2007 International Patient Safety GoalsElias Baraket FreijyAinda não há avaliações
- Patient Safety in The Operating RoomDocumento5 páginasPatient Safety in The Operating RoompabelloncatAinda não há avaliações
- CLCGP030 Theatre Operating List Session Scheduling PolicyDocumento19 páginasCLCGP030 Theatre Operating List Session Scheduling PolicyJeffy PuruggananAinda não há avaliações
- Sickness ProcedureDocumento27 páginasSickness ProcedureRay LeoAinda não há avaliações
- Operating Room Attire 2018Documento5 páginasOperating Room Attire 2018andrea rabangAinda não há avaliações
- Preoxygenation During Induction of Anesthesia in Noncritically Ill PatientsDocumento6 páginasPreoxygenation During Induction of Anesthesia in Noncritically Ill PatientsasfwegereAinda não há avaliações
- PBM Module1 MTP Template 0Documento2 páginasPBM Module1 MTP Template 0Daniela Marie RonquilloAinda não há avaliações
- Urinary CatheterDocumento4 páginasUrinary CatheterBindu SinghAinda não há avaliações
- Concept II-Vital StatisticsDocumento10 páginasConcept II-Vital Statisticsjpoti100% (1)
- ICTM111 PDF 02 - Healthcare System, Health System Framework & PH Health SystemDocumento4 páginasICTM111 PDF 02 - Healthcare System, Health System Framework & PH Health SystemJamAinda não há avaliações
- Major Basic Instrument SetDocumento4 páginasMajor Basic Instrument SetRaisah Bint AbdullahAinda não há avaliações
- Hemodialysis Central Venous Catheter STH ProtocolDocumento2 páginasHemodialysis Central Venous Catheter STH ProtocolNor HilaliahAinda não há avaliações
- Standards of PracticeDocumento9 páginasStandards of PracticeAlfitoHarfahGiffaryAinda não há avaliações
- Anesthesia For The Patient With Peripartum Hemorrhage - UpToDateDocumento25 páginasAnesthesia For The Patient With Peripartum Hemorrhage - UpToDateZurya UdayanaAinda não há avaliações
- 3rd Edition NABH Guidebook 2012 New PDFDocumento258 páginas3rd Edition NABH Guidebook 2012 New PDFraamki_99Ainda não há avaliações
- Emergency CodesDocumento23 páginasEmergency CodesJennifer B. GarciaAinda não há avaliações
- NCM 113 Examination Coverage and DateDocumento81 páginasNCM 113 Examination Coverage and DateDONNA MAE FUENTESAinda não há avaliações
- MR Ahm Medical RecordDocumento12 páginasMR Ahm Medical RecordTanti Farida RahmanAinda não há avaliações
- Health Care Waste Assessment ToolsDocumento28 páginasHealth Care Waste Assessment ToolsMohammed NabeelAinda não há avaliações
- AAU Senate Legislation of 2019Documento178 páginasAAU Senate Legislation of 2019carelessmanAinda não há avaliações
- Sedation Policy LPCH 6 11Documento24 páginasSedation Policy LPCH 6 11Tribowo WicaksonoAinda não há avaliações
- Position S: Pratiksha RaiDocumento49 páginasPosition S: Pratiksha RaiJoanne Cristie TolopiaAinda não há avaliações
- Primary HealthcareDocumento5 páginasPrimary HealthcareCHELSEA MOLINOS JUANAinda não há avaliações
- Aseptic Techniques PP TDocumento31 páginasAseptic Techniques PP TOjambo FlaviaAinda não há avaliações
- Aseptic Non Touch Technique Guidelines ANTTDocumento15 páginasAseptic Non Touch Technique Guidelines ANTTMa Anna Cris Lumongsud100% (1)
- Get ResourceDocumento28 páginasGet ResourceWalaa ElleithyAinda não há avaliações
- Patterns of Inheritance-Autosomal Recessive DiseaseDocumento7 páginasPatterns of Inheritance-Autosomal Recessive Diseasejoryjohary100% (1)
- X-Linked Recessive InheritanceDocumento1 páginaX-Linked Recessive InheritancejoryjoharyAinda não há avaliações
- Second Stage Labour CareDocumento2 páginasSecond Stage Labour Carejoryjohary100% (1)
- Struggling To Surrender - Some Impressions of An American Convert To Islam - Jeffery LangDocumento241 páginasStruggling To Surrender - Some Impressions of An American Convert To Islam - Jeffery Langapi-319543419Ainda não há avaliações
- IPPOL17 Aseptic Non Touch Tecnique (ANTT) PolicyDocumento27 páginasIPPOL17 Aseptic Non Touch Tecnique (ANTT) PolicyEvangelin MelvinAinda não há avaliações
- Aseptic Processing: A Review of Current Industry Practice: James Agalloco, James Akers, and Russell MadsenDocumento13 páginasAseptic Processing: A Review of Current Industry Practice: James Agalloco, James Akers, and Russell MadsenjbertralAinda não há avaliações
- Chart 10. Microbiology: Microbial Enumeration Endotoxin LimitsDocumento1 páginaChart 10. Microbiology: Microbial Enumeration Endotoxin LimitsThomas Niccolo Filamor ReyesAinda não há avaliações
- Asepsis & Infection Control: Handwashing and GlovingDocumento15 páginasAsepsis & Infection Control: Handwashing and GlovingGladys YaresAinda não há avaliações
- Surgical Services Design Guide PDFDocumento465 páginasSurgical Services Design Guide PDFCharles TestaAinda não há avaliações
- O R - Evaluation-ToolDocumento3 páginasO R - Evaluation-ToolLoungayvan BatuyogAinda não há avaliações
- Intravenous Admixture SystemDocumento61 páginasIntravenous Admixture SystemFitriah SalahuddinAinda não há avaliações
- Caring For A Hemovac DrainDocumento15 páginasCaring For A Hemovac DrainJaily Mariano0% (1)
- Subject: Nursing Education: Demonstration OnDocumento34 páginasSubject: Nursing Education: Demonstration OnBabita DhruwAinda não há avaliações
- J.G College of Nursing, AhmedabadDocumento15 páginasJ.G College of Nursing, AhmedabadKatie HolmesAinda não há avaliações
- Or Tour: Front DeskDocumento4 páginasOr Tour: Front DeskTomato MenudoAinda não há avaliações
- AsepsisDocumento20 páginasAsepsisErSandeepVermaAinda não há avaliações
- Theatre NursingDocumento4 páginasTheatre Nursinggeorgeloto1250% (2)
- Wound DressingDocumento18 páginasWound DressingKristi Elly YoehanaAinda não há avaliações
- Or ConceptsDocumento70 páginasOr ConceptsArnulfo ArmamentoAinda não há avaliações
- Ward Prep NotesDocumento7 páginasWard Prep NotesReese Alessandra GandulfoAinda não há avaliações
- Control of Microbial GrowthDocumento35 páginasControl of Microbial GrowthVincent ManganaanAinda não há avaliações
- 2010 KUHS B.SC (N) SyllabusDocumento254 páginas2010 KUHS B.SC (N) SyllabusJMCON LibraryAinda não há avaliações
- Thesis - Final (2) (Repaired)Documento61 páginasThesis - Final (2) (Repaired)Alexis MutuyimanaAinda não há avaliações
- Safe Effective Care RationalesDocumento9 páginasSafe Effective Care Rationalesrhymes2u100% (2)
- Small Animal Surgical Nursing: Skills and Concepts, 2006, 413 Pages, Sara J. Busch, 0323030637, 9780323030632, Elsevier Mosby, 2006Documento19 páginasSmall Animal Surgical Nursing: Skills and Concepts, 2006, 413 Pages, Sara J. Busch, 0323030637, 9780323030632, Elsevier Mosby, 2006mdmostafiz446Ainda não há avaliações
- Year 3 Courses - Semester I & 2 - MBCHBDocumento14 páginasYear 3 Courses - Semester I & 2 - MBCHBDeborah ChemutaiAinda não há avaliações
- Asepsis and Infection ControlDocumento6 páginasAsepsis and Infection ControlgilissaAinda não há avaliações
- PCM1 Midterm Exam Study GuideDocumento11 páginasPCM1 Midterm Exam Study GuidedjgAinda não há avaliações
- Dermatology Brochure - RegeneraActivaDocumento30 páginasDermatology Brochure - RegeneraActivaBiomed Medex OmanAinda não há avaliações
- 100 QuestionsDocumento11 páginas100 QuestionsSantosh KumarAinda não há avaliações
- Operation TheatreDocumento22 páginasOperation TheatreAbirami100% (1)
- Surgery-I Review (2019)Documento12 páginasSurgery-I Review (2019)Margaret ThatcherAinda não há avaliações
- Situation: Nursing Theory and Concepts Are The Basic Foundation of Nursing Practice Hence A Nurse Must Have A Good Knowledge With These ConceptsDocumento6 páginasSituation: Nursing Theory and Concepts Are The Basic Foundation of Nursing Practice Hence A Nurse Must Have A Good Knowledge With These ConceptsPaul EspinosaAinda não há avaliações
- Overview of Infection ControlDocumento43 páginasOverview of Infection ControlRhodora BenipayoAinda não há avaliações