Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- CC 12918Documento59 páginasCC 12918Romica MarcanAinda não há avaliações
- CC 12918Documento59 páginasCC 12918Romica MarcanAinda não há avaliações
- Gacp WhoDocumento80 páginasGacp WhoGarnasih Putri RastitiAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Asean Guidelines For: Final Draft: 21 July 2004Documento29 páginasAsean Guidelines For: Final Draft: 21 July 2004Jone YingAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- ASEAN Stability GuidelineDocumento37 páginasASEAN Stability GuidelinevarizzzAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Vancomycin: Group 5 R.M 2Documento31 páginasVancomycin: Group 5 R.M 2vi_wiviaAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- 263 - Dosing Information in Renal ImpairmentDocumento18 páginas263 - Dosing Information in Renal Impairmentvi_wiviaAinda não há avaliações
- 263 - Dosing Information in Renal ImpairmentDocumento18 páginas263 - Dosing Information in Renal Impairmentvi_wiviaAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Guide To Drug Dose Adjustment in Renal Impairment: (Based On Cockcroft-Gault Equation, Adapted From BNF)Documento2 páginasGuide To Drug Dose Adjustment in Renal Impairment: (Based On Cockcroft-Gault Equation, Adapted From BNF)vi_wiviaAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Guide To Drug Dose Adjustment in Renal Impairment: (Based On Cockcroft-Gault Equation, Adapted From BNF)Documento2 páginasGuide To Drug Dose Adjustment in Renal Impairment: (Based On Cockcroft-Gault Equation, Adapted From BNF)vi_wiviaAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Limitations of Learning by Discovery - Ausubel PDFDocumento14 páginasLimitations of Learning by Discovery - Ausubel PDFOpazo SebastianAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Experiment No. 2 Rockwell Hardness Test IntroductionDocumento3 páginasExperiment No. 2 Rockwell Hardness Test IntroductionAhmad Abd100% (1)
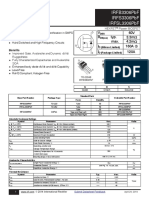
- Irfb3306Pbf Irfs3306Pbf Irfsl3306Pbf: V 60V R Typ. 3.3M: Max. 4.2M I 160A C I 120ADocumento12 páginasIrfb3306Pbf Irfs3306Pbf Irfsl3306Pbf: V 60V R Typ. 3.3M: Max. 4.2M I 160A C I 120ADirson Volmir WilligAinda não há avaliações
- Class - B Complementary Symmetry Power AmplifierDocumento3 páginasClass - B Complementary Symmetry Power AmplifierAnonymous SH0A20Ainda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Chapter 16 - Oral Radiography (Essentials of Dental Assisting)Documento96 páginasChapter 16 - Oral Radiography (Essentials of Dental Assisting)mussanteAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- New Features in IbaPDA v7.1.0Documento39 páginasNew Features in IbaPDA v7.1.0Miguel Ángel Álvarez VázquezAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Library of Babel - WikipediaDocumento35 páginasThe Library of Babel - WikipediaNeethu JosephAinda não há avaliações
- Polya Problem Solving StrategiesDocumento12 páginasPolya Problem Solving StrategiesGwandaleana VwearsosaAinda não há avaliações
- General Pathology Lecture Group 1 HandoutDocumento6 páginasGeneral Pathology Lecture Group 1 HandoutCecille AnnAinda não há avaliações
- Chapter 3Documento23 páginasChapter 3pganoelAinda não há avaliações
- EC 201 Network TheoryDocumento2 páginasEC 201 Network TheoryJoseph JohnAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Relay Maintenance and Testing: BenefitsDocumento2 páginasRelay Maintenance and Testing: BenefitsojoladapoAinda não há avaliações
- 3x Exemplar 2017 en PDFDocumento4 páginas3x Exemplar 2017 en PDFgudzalovAinda não há avaliações
- (Complete) Electrolysis of Copper SulphateDocumento4 páginas(Complete) Electrolysis of Copper SulphateNoooooAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Teleprotection Over IP MPLS Network White PaperDocumento23 páginasTeleprotection Over IP MPLS Network White PaperLakshmi Kiran100% (1)
- Business Process MappingDocumento14 páginasBusiness Process MappinghanxinAinda não há avaliações
- Biomechanic of Foot PDFDocumento8 páginasBiomechanic of Foot PDFMichealowen BabygoalAinda não há avaliações
- Chapter 1 IntroductionDocumento49 páginasChapter 1 IntroductionGemex4fshAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (120)
- College of Technology & Engineering: Practical Training at Hindustan Zinc Limited Zinc Smelter, Debari UdaipurDocumento24 páginasCollege of Technology & Engineering: Practical Training at Hindustan Zinc Limited Zinc Smelter, Debari UdaipurPooja SahuAinda não há avaliações
- 1400 CFM TDocumento3 páginas1400 CFM TmahmadwasiAinda não há avaliações
- Spare Parts List: Hydraulic BreakerDocumento28 páginasSpare Parts List: Hydraulic BreakerTeknik MakinaAinda não há avaliações
- Ergonomic DesignDocumento132 páginasErgonomic DesignErin WalkerAinda não há avaliações
- Sap SCM TrainingDocumento5 páginasSap SCM TrainingGLOBAL TEQAinda não há avaliações
- AlgebraDocumento66 páginasAlgebraOliseyenum Precious ChukuemekeAinda não há avaliações
- Index Terms LinksDocumento31 páginasIndex Terms Linksdeeptiwagle5649Ainda não há avaliações
- Checklist For Conreting WorkDocumento13 páginasChecklist For Conreting WorkMin Khant AungAinda não há avaliações
- PRD Doc Pro 3201-00001 Sen Ain V31Documento10 páginasPRD Doc Pro 3201-00001 Sen Ain V31rudybestyjAinda não há avaliações
- Magnetism NotesDocumento14 páginasMagnetism Notesapi-277818647Ainda não há avaliações
- 7FA Upgrade Combustion HardwareDocumento2 páginas7FA Upgrade Combustion Hardwaresauerbach1Ainda não há avaliações