Você também pode gostar
- Songs at The Forge: English SongsDocumento44 páginasSongs at The Forge: English SongsmandrakesMD93% (14)
- Integrated Management of Childhood Illness: Child Aged 2 Months Up To 5 YearsDocumento44 páginasIntegrated Management of Childhood Illness: Child Aged 2 Months Up To 5 YearsJulio Iñigo López100% (22)
- Hepatitis A-E VirusesDocumento7 páginasHepatitis A-E VirusesmandrakesMDAinda não há avaliações
- Viral Infections Comprehensive ReviewDocumento27 páginasViral Infections Comprehensive ReviewmandrakesMDAinda não há avaliações
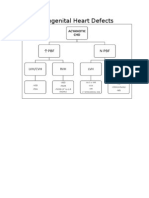
- Congenital Heart DefectsDocumento2 páginasCongenital Heart DefectsmandrakesMDAinda não há avaliações
- Gyne Rep Endo-Dr. Ona CruzDocumento12 páginasGyne Rep Endo-Dr. Ona CruzmandrakesMDAinda não há avaliações
- Bacte-Pedia Part 1Documento29 páginasBacte-Pedia Part 1mandrakesMDAinda não há avaliações
- Bacte Tb-PediaDocumento7 páginasBacte Tb-PediamandrakesMDAinda não há avaliações
- Evaluation of The Infant or Child With Congenital Heart DiseaseDocumento25 páginasEvaluation of The Infant or Child With Congenital Heart DiseasemandrakesMD100% (1)
- Lung CancerDocumento22 páginasLung CancermandrakesMD100% (1)
- Acquired Heart Disease - Pediatric Cardio ADocumento12 páginasAcquired Heart Disease - Pediatric Cardio AmandrakesMD100% (2)
- Obstructive Sleep Apnea - Pulmo LectureDocumento16 páginasObstructive Sleep Apnea - Pulmo LecturemandrakesMD0% (1)
- Bacterial Infections - Pediatrics Part 2Documento12 páginasBacterial Infections - Pediatrics Part 2mandrakesMDAinda não há avaliações
- Acquired Heart Disease - Pediatric Cardio ADocumento12 páginasAcquired Heart Disease - Pediatric Cardio AmandrakesMD100% (2)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5782)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Patho Common Stuff - RobbinsDocumento7 páginasPatho Common Stuff - RobbinsMaf BAinda não há avaliações
- Breast Cancer PresentationDocumento48 páginasBreast Cancer Presentationvanessa91% (11)
- Rasoushadhis in ArbudaDocumento67 páginasRasoushadhis in ArbudaSundara VeerrajuAinda não há avaliações
- Why Cells Divide: Understanding Cell Growth and HealingDocumento60 páginasWhy Cells Divide: Understanding Cell Growth and Healingmeher singhAinda não há avaliações
- Case Report: Multiple Skeletal Metastases From A Giant Cell Tumour of The Distal Fibula With Fatal OucomeDocumento28 páginasCase Report: Multiple Skeletal Metastases From A Giant Cell Tumour of The Distal Fibula With Fatal OucomeWaskitho NugrohoAinda não há avaliações
- Management of Cancer Notes For UndergraduatesDocumento27 páginasManagement of Cancer Notes For UndergraduatesLathaNarayanan BhattathiriAinda não há avaliações
- Homoeopathy for Breast CancerDocumento5 páginasHomoeopathy for Breast Cancerkathir_cAinda não há avaliações
- CPD Pulmo, USG SKIRING Hepar Bagi Pulmonologist Dr. Daniel 2022Documento43 páginasCPD Pulmo, USG SKIRING Hepar Bagi Pulmonologist Dr. Daniel 2022Dammar DjatiAinda não há avaliações
- Cancer - Nursing - ReviewerDocumento7 páginasCancer - Nursing - ReviewerDarius CrisostomoAinda não há avaliações
- Cancer Biology: Bio 117 Cell & Molecular BiologyDocumento35 páginasCancer Biology: Bio 117 Cell & Molecular BiologyQueen Grace C. Balbutin100% (1)
- NCCN Bone CancerDocumento93 páginasNCCN Bone Canceraurika sinambelaAinda não há avaliações
- Pathology of BreastDocumento87 páginasPathology of BreastPandu Harsarapama100% (2)
- Urologic Clinics of North AmericaDocumento160 páginasUrologic Clinics of North AmericaHaytham Ibrahim KamelAinda não há avaliações
- Staging of Colorectal CancerDocumento47 páginasStaging of Colorectal Cancerbo gum parkAinda não há avaliações
- EpendymomaDocumento5 páginasEpendymomaDenny's BerciaAinda não há avaliações
- Case PresentationDocumento21 páginasCase PresentationDrArish MahmoodAinda não há avaliações
- Hallmarks of Cancer: New Dimensions: ReviewDocumento17 páginasHallmarks of Cancer: New Dimensions: ReviewVignesh RavichandranAinda não há avaliações
- NEOPLASIADocumento70 páginasNEOPLASIARose de DiosAinda não há avaliações
- Imaging of Solitary and Multiple Pulmonary NodulesDocumento75 páginasImaging of Solitary and Multiple Pulmonary NodulesAnshulVarshneyAinda não há avaliações
- Intrahepatic Cholangiocarcinoma Surgery The ImpactDocumento10 páginasIntrahepatic Cholangiocarcinoma Surgery The Impactraplyhollow_68780740Ainda não há avaliações
- Medical Terminologies For Clinical ChemistryDocumento4 páginasMedical Terminologies For Clinical ChemistryScoobminiAinda não há avaliações
- Neoplasia: Key PointsDocumento16 páginasNeoplasia: Key PointsskAinda não há avaliações
- 12 Human Health & Diseases Ncert QuestionsDocumento7 páginas12 Human Health & Diseases Ncert Questionssamsung tabletAinda não há avaliações
- The Safe Use of Syringe Driver in Palliative CareDocumento3 páginasThe Safe Use of Syringe Driver in Palliative CarecohenserbanAinda não há avaliações
- Lesson Plan On Breast Cancer Pathology 2nd Year Bsc. Nursing.Documento17 páginasLesson Plan On Breast Cancer Pathology 2nd Year Bsc. Nursing.Suman Pandey100% (1)
- Notes: Non-Urothelial Bladder CancersDocumento5 páginasNotes: Non-Urothelial Bladder CancersTrivedi NisargAinda não há avaliações
- Sgop 2012Documento108 páginasSgop 2012PhoebeKatezPiedraCampasasAinda não há avaliações
- Role of Neoantigens in Cancer TherapyDocumento7 páginasRole of Neoantigens in Cancer TherapySazuAinda não há avaliações
- 2012 UpmcccanualreportDocumento70 páginas2012 Upmcccanualreportapi-290001443Ainda não há avaliações
- Medical Surgical NursingDocumento2 páginasMedical Surgical Nursingken_gondaAinda não há avaliações