Você também pode gostar
- Love Quotes From Books / MoviesDocumento1 páginaLove Quotes From Books / MoviesanasokourAinda não há avaliações
- And The Pursuit of Happiness. These Simple Assertions Started A Revolution ThatDocumento2 páginasAnd The Pursuit of Happiness. These Simple Assertions Started A Revolution ThatanasokourAinda não há avaliações
- ConversationDocumento2 páginasConversationanasokourAinda não há avaliações
- The Big List of Language For Talking About LessonsDocumento4 páginasThe Big List of Language For Talking About LessonsanasokourAinda não há avaliações
- Instructional Strategies: 1-Direct Instruction 2-Problem - Solving& Induction N3-GroupworkDocumento3 páginasInstructional Strategies: 1-Direct Instruction 2-Problem - Solving& Induction N3-GroupworkanasokourAinda não há avaliações
- Writing SkillDocumento1 páginaWriting SkillanasokourAinda não há avaliações
- Reading Skill Rubric For Reading Comprehension 9th GradeDocumento2 páginasReading Skill Rubric For Reading Comprehension 9th GradeanasokourAinda não há avaliações
- RespiratoryDocumento34 páginasRespiratoryanasokour100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Aap 2009Documento538 páginasAap 2009toniassaf100% (1)
- Bordetella Pertussis and Whooping CoughDocumento22 páginasBordetella Pertussis and Whooping CoughDian TikaAinda não há avaliações
- Doh Programs Related To Family Health - Expanded Programs On ImmunizationDocumento3 páginasDoh Programs Related To Family Health - Expanded Programs On ImmunizationPatrisha Bianca Paige BadillesAinda não há avaliações
- Mediplus: 2019 Benefit GuideDocumento24 páginasMediplus: 2019 Benefit GuideBruce FerreiraAinda não há avaliações
- CHN Final ExamDocumento12 páginasCHN Final ExamChristine UdhayAinda não há avaliações
- Community Health NursingDocumento396 páginasCommunity Health NursingAiza Oronce100% (2)
- Chapter 9 Health SupervisionDocumento9 páginasChapter 9 Health SupervisionKatrina UrbanoAinda não há avaliações
- RRB Paramedical Previous Paper 1 PDFDocumento7 páginasRRB Paramedical Previous Paper 1 PDFShiva RamAinda não há avaliações
- Statistical Profile of Scheduled Tribes in IndiaDocumento269 páginasStatistical Profile of Scheduled Tribes in Indiavky13218Ainda não há avaliações
- Article Review: Protecting Infants Against PertussisDocumento2 páginasArticle Review: Protecting Infants Against PertussisMadiAinda não há avaliações
- Parent Ver SCH 0 6yrsDocumento2 páginasParent Ver SCH 0 6yrsSrinivasamurthy KamarthiAinda não há avaliações
- TD (Tetanus, Diphtheria) Vaccine:: What You Need To KnowDocumento2 páginasTD (Tetanus, Diphtheria) Vaccine:: What You Need To KnowILyes GrAinda não há avaliações
- CH 11 IAP Parental Guide On VaccinationDocumento9 páginasCH 11 IAP Parental Guide On VaccinationAkankshaKirtiAinda não há avaliações
- Towards Water Sustainability: Ias Prelims Exam How To Command Polity Topics WDocumento40 páginasTowards Water Sustainability: Ias Prelims Exam How To Command Polity Topics WMohaideen SubaireAinda não há avaliações
- Lampiran Diagnosa Peer Review Puskesmas GondangDocumento14 páginasLampiran Diagnosa Peer Review Puskesmas Gondangyugo purwoAinda não há avaliações
- Obg Sem by Padmashree Institute of NursingDocumento26 páginasObg Sem by Padmashree Institute of NursingmOHAN.S100% (1)
- Gurmesa Bekele Yadeta 4Documento79 páginasGurmesa Bekele Yadeta 4Gurmessa BekeleAinda não há avaliações
- Vaccination For The Prevention of Shingles (Herpes Zoster) - UpToDateDocumento13 páginasVaccination For The Prevention of Shingles (Herpes Zoster) - UpToDateAlcemir JúniorAinda não há avaliações
- LAP DirectoryDocumento36 páginasLAP Directorydolly wattaAinda não há avaliações
- TTAV 7 Episodes TranscriptDocumento220 páginasTTAV 7 Episodes TranscriptRaul CortesAinda não há avaliações
- ECCD Vaccine Evaluation AdvancedDocumento47 páginasECCD Vaccine Evaluation Advancedko nayAinda não há avaliações
- ImmunizationDocumento2 páginasImmunizationannamcconkeyAinda não há avaliações
- School NursingDocumento407 páginasSchool NursingKa MiiAinda não há avaliações
- 413 Health Care SQPDocumento7 páginas413 Health Care SQPAnil SarohaAinda não há avaliações
- ABC's of Primary Health Care...Documento24 páginasABC's of Primary Health Care...rhenier_ilado100% (7)
- Protocol For Malaysian HospitalsDocumento434 páginasProtocol For Malaysian HospitalsSidney Lee100% (1)
- Proof The Covid-19 Jabs Should Be Stopped NowDocumento2 páginasProof The Covid-19 Jabs Should Be Stopped NowDiogo MiguelAinda não há avaliações
- All Mcqs of CHNDocumento115 páginasAll Mcqs of CHNumar khan93% (46)
- The Clinician's VaccineDocumento386 páginasThe Clinician's Vaccinekaren ceballosAinda não há avaliações
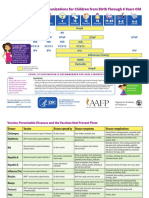
- 0 To 18yrs Combined Immunization ScheduleDocumento8 páginas0 To 18yrs Combined Immunization ScheduleNurses CommunityAinda não há avaliações