Você também pode gostar
- WalkthroughDocumento14 páginasWalkthroughGadge75% (4)
- PNLE: Maternal and Child Health Nursing Exam 3Documento41 páginasPNLE: Maternal and Child Health Nursing Exam 3Lot Rosit50% (2)
- Human Anatomy 7th Edition Marieb Test BankDocumento20 páginasHuman Anatomy 7th Edition Marieb Test BankKerriAdamsdwroi100% (14)
- Maternal and Child Nursing Post Test ReviewDocumento29 páginasMaternal and Child Nursing Post Test ReviewYaj CruzadaAinda não há avaliações
- Nle Pre Board June 2008 Npt1-Questions and RationaleDocumento25 páginasNle Pre Board June 2008 Npt1-Questions and RationaleAna Marie Besa Battung-ZalunAinda não há avaliações
- Nur - 100 Session 2 - SemillaDocumento6 páginasNur - 100 Session 2 - SemillaVon R Semilla100% (1)
- NCLEX Sample Questions For Maternal and Child Health Nursing 2Documento17 páginasNCLEX Sample Questions For Maternal and Child Health Nursing 2Rose Dacles100% (3)
- Pedia Exam 2Documento18 páginasPedia Exam 2quidditch07100% (2)
- Maternal and Child Health Nursing ReviewerDocumento17 páginasMaternal and Child Health Nursing ReviewerJeffrey Viernes100% (6)
- Obstetrical Nursing Practice ExamDocumento11 páginasObstetrical Nursing Practice Examstuffednurse83% (12)
- OCHONDRA CA - FinalExam - 2020Documento15 páginasOCHONDRA CA - FinalExam - 2020joyrena ochondraAinda não há avaliações
- TH ST TH TH ST TH STDocumento7 páginasTH ST TH TH ST TH STPaul Espinosa0% (3)
- MCN-OB Questions and RationalesDocumento23 páginasMCN-OB Questions and RationalesRI NA100% (3)
- Obstetric Sample Questions With RationaleDocumento31 páginasObstetric Sample Questions With RationaleTomzki Cornelio50% (2)
- CA2 Pediatric Nursing Review Post TestDocumento5 páginasCA2 Pediatric Nursing Review Post Testgabby100% (2)
- Fundamentals or Nursing ExamDocumento18 páginasFundamentals or Nursing Examapi-371817494% (16)
- NLE Practice Exam With AnswersDocumento43 páginasNLE Practice Exam With AnswersSuzette Rae TateAinda não há avaliações
- MCN Quizzes on Genetic Disorders & Pregnancy ComplicationsDocumento22 páginasMCN Quizzes on Genetic Disorders & Pregnancy ComplicationsRaquel Monsalve67% (3)
- Pediatric Nursing PrioritiesDocumento6 páginasPediatric Nursing PrioritiesJavier Shields83% (6)
- Essential Info on Conception and Fetal DevelopmentDocumento56 páginasEssential Info on Conception and Fetal DevelopmentJohanna Erazo Padilla80% (10)
- Maternal & Child Nursing Achievement TestDocumento13 páginasMaternal & Child Nursing Achievement TestMatelyn Oarga100% (1)
- MCN ExamDocumento10 páginasMCN ExamYaj CruzadaAinda não há avaliações
- PNLE NCLEX Practice Exam For Maternal and Child Health Nursing 2Documento5 páginasPNLE NCLEX Practice Exam For Maternal and Child Health Nursing 2bobtaguba100% (1)
- MCN Exam Questions 2Documento15 páginasMCN Exam Questions 2Emer Joy T. Vale67% (6)
- Practice Test Maternity-Nsg 100 ItemsDocumento21 páginasPractice Test Maternity-Nsg 100 ItemsPaul Christian P. Santos, RN100% (21)
- 50 Maternal and Child NCLEX QuestionsDocumento14 páginas50 Maternal and Child NCLEX QuestionsShengxy Ferrer100% (2)
- Answer and Rationale MaternityDocumento21 páginasAnswer and Rationale MaternityMark ElbenAinda não há avaliações
- Nle Pre Board June 2008 Npt2-Questions and RationaleDocumento22 páginasNle Pre Board June 2008 Npt2-Questions and RationaleJacey Racho100% (1)
- MCN Exam Gestational ConditionsDocumento9 páginasMCN Exam Gestational ConditionsEdith Cabrera Cabigas - SabalboroAinda não há avaliações
- FREE NLE REVIEW Np2Documento38 páginasFREE NLE REVIEW Np2Charm LigawadAinda não há avaliações
- Nursing Test 2 (NP Ii)Documento7 páginasNursing Test 2 (NP Ii)Yuxin LiuAinda não há avaliações
- Maternal ExamDocumento52 páginasMaternal ExamEdRobertArnad100% (14)
- Funda Prof - Ad LMR AnswersDocumento35 páginasFunda Prof - Ad LMR AnswersFreeNursingNotesAinda não há avaliações
- Birthing Center Nursing Care and ProceduresDocumento8 páginasBirthing Center Nursing Care and ProceduresJayselle ArvieAinda não há avaliações
- PNLE Maternal and Child Health Nursing Exam - Reviewer PDFDocumento29 páginasPNLE Maternal and Child Health Nursing Exam - Reviewer PDFSheng DekitAinda não há avaliações
- Midterm Exam Review for Maternal and Child NursingDocumento7 páginasMidterm Exam Review for Maternal and Child NursingCres Padua QuinzonAinda não há avaliações
- MCN QuizDocumento6 páginasMCN QuizMÖna Macaranas100% (5)
- Nursing Practice IIIDocumento17 páginasNursing Practice IIIstuffednurse100% (3)
- Maternal and Child Health Nursing TestDocumento21 páginasMaternal and Child Health Nursing TestAt Day's Ward50% (2)
- Prioritizing Nursing Actions for the Philippine Nursing Licensure Exam (PNLEDocumento73 páginasPrioritizing Nursing Actions for the Philippine Nursing Licensure Exam (PNLEabcalagoAinda não há avaliações
- NCLEX Maternal and Child Health Nursing Practice QuestionsDocumento7 páginasNCLEX Maternal and Child Health Nursing Practice Questionsraquel maniegoAinda não há avaliações
- Competency Appraisal Pregnancy SignsDocumento19 páginasCompetency Appraisal Pregnancy SignsJan Crizza Dale R. FrancoAinda não há avaliações
- NP2 RationaleDocumento19 páginasNP2 RationaleElizabella Henrietta TanaquilAinda não há avaliações
- Maternal Exam CIDocumento9 páginasMaternal Exam CIRyojie RetomaAinda não há avaliações
- PALMDocumento21 páginasPALMGiovanni Enrile100% (1)
- IMCI Post TESTDocumento7 páginasIMCI Post TESTeric100% (1)
- NP4 Nursing Board Exam NotesDocumento9 páginasNP4 Nursing Board Exam NotesNewb TobikkoAinda não há avaliações
- MCN ExamDocumento13 páginasMCN ExamtinaAinda não há avaliações
- Sec. 3C - 1 - OB Questions (Answer Key) - BrendaDocumento20 páginasSec. 3C - 1 - OB Questions (Answer Key) - Brendacididok84Ainda não há avaliações
- NP2 Nursing Board Exam June 2008 Answer KeyDocumento14 páginasNP2 Nursing Board Exam June 2008 Answer KeyBettina SanchezAinda não há avaliações
- Genetic counseling and self testicular examDocumento1 páginaGenetic counseling and self testicular examRosemarie R. ReyesAinda não há avaliações
- Pdfmergerfreecom Philippine Nursing Licensure Exam Pnle Rnpedia 2Documento1 páginaPdfmergerfreecom Philippine Nursing Licensure Exam Pnle Rnpedia 2Hazel100% (1)
- 15 Nursing Care of A Family During Labor and BirthDocumento14 páginas15 Nursing Care of A Family During Labor and BirthNurse UtopiaAinda não há avaliações
- Evaluation Exam For NCM 101Documento4 páginasEvaluation Exam For NCM 101myrna pedidoAinda não há avaliações
- Manila Adventist College Nursing Online AssignmentDocumento15 páginasManila Adventist College Nursing Online AssignmentAb Staholic Boii100% (1)
- Online Assignment 4Documento10 páginasOnline Assignment 4Ab Staholic BoiiAinda não há avaliações
- Quiz 1 Maternity NursingDocumento230 páginasQuiz 1 Maternity NursingAllaiza CristilleAinda não há avaliações
- Introduction To Maternity and Pediatric Nursing 6Th Edition Leifer Test Bank Full Chapter PDFDocumento33 páginasIntroduction To Maternity and Pediatric Nursing 6Th Edition Leifer Test Bank Full Chapter PDFotisfarrerfjh2100% (8)
- MCN Intra Partum Quiz QuestionsDocumento20 páginasMCN Intra Partum Quiz QuestionsKyla CapituloAinda não há avaliações
- NP 2 SET A - BOARD OF NURSINGDocumento30 páginasNP 2 SET A - BOARD OF NURSINGmarieekariee777Ainda não há avaliações
- CPC Report 2023 Final DraftDocumento35 páginasCPC Report 2023 Final DraftJo InglesAinda não há avaliações
- Menorrhagia (Heavy Menstrual Bleeding)Documento55 páginasMenorrhagia (Heavy Menstrual Bleeding)Aizi DwimeilaAinda não há avaliações
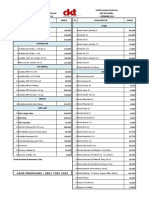
- DKT Indonesia Daftar Harga Produk Kontrasepsi 1 September 2018Documento4 páginasDKT Indonesia Daftar Harga Produk Kontrasepsi 1 September 2018YuliantiAinda não há avaliações
- Notes CBSE-Class-12-Biology-Human-Reproduction-Practice-QuestionsDocumento11 páginasNotes CBSE-Class-12-Biology-Human-Reproduction-Practice-QuestionsVikramAinda não há avaliações
- Fk-Umi: Dr. Kamajaya, MSC, SpandDocumento68 páginasFk-Umi: Dr. Kamajaya, MSC, SpanddebiAinda não há avaliações
- LESSON PLAN For COTDocumento5 páginasLESSON PLAN For COTMerrie Anne Pascual BagsicAinda não há avaliações
- Color Doppler ultrasound venous diameter predicts clinical varicocele gradeDocumento6 páginasColor Doppler ultrasound venous diameter predicts clinical varicocele gradeMuhammad FaisalAinda não há avaliações
- Philippines Supreme Court upholds most of Reproductive Health LawDocumento2 páginasPhilippines Supreme Court upholds most of Reproductive Health LawRon AceAinda não há avaliações
- MCQ 20Documento19 páginasMCQ 20Old driverAinda não há avaliações
- Handbook On Improving MCH Through RMNCH+A ApproachDocumento32 páginasHandbook On Improving MCH Through RMNCH+A ApproachJennifer Pearson-ParedesAinda não há avaliações
- How Do Organisms ReproduceDocumento8 páginasHow Do Organisms ReproducesushantAinda não há avaliações
- Teenage Pregnancy FinalDocumento3 páginasTeenage Pregnancy FinalCesar AmayaAinda não há avaliações
- Treating Recurrent Miscarriage with Traditional Chinese MedicineDocumento12 páginasTreating Recurrent Miscarriage with Traditional Chinese MedicineLecery Sophia WongAinda não há avaliações
- Bio T4 DLP KSSM Chapter15Documento99 páginasBio T4 DLP KSSM Chapter15Nurasyikin SaidinAinda não há avaliações
- Perineal CareDocumento3 páginasPerineal CareandreabreeAinda não há avaliações
- SF2 - 2019 - Grade 8 (Year II) - OLOHRDocumento3 páginasSF2 - 2019 - Grade 8 (Year II) - OLOHRjayson daladarAinda não há avaliações
- Lory Hui LomiDocumento20 páginasLory Hui Lomibill5Ainda não há avaliações
- Sexual and Reproductive Health Rights Among Married WomenDocumento10 páginasSexual and Reproductive Health Rights Among Married WomenArjun TamangAinda não há avaliações
- Menstrual CycleDocumento12 páginasMenstrual CycleJadessa VallarAinda não há avaliações
- Ncm107j Weekly NotesDocumento11 páginasNcm107j Weekly NotesSHEENA MAE DE LOS REYESAinda não há avaliações
- Penile Length-Somatometric Parameters Relationship in Healthy Egyptian MenDocumento5 páginasPenile Length-Somatometric Parameters Relationship in Healthy Egyptian Mengohary18047Ainda não há avaliações
- CPD: Cephalo-Pelvic Disproportion PathophysiologyDocumento3 páginasCPD: Cephalo-Pelvic Disproportion PathophysiologyTeanne Bathan100% (1)
- Placenta Previa, Abruptio Placenta, Anemia: Causes, Signs and Nursing CareDocumento3 páginasPlacenta Previa, Abruptio Placenta, Anemia: Causes, Signs and Nursing CareBench AvilaAinda não há avaliações
- FertilizationDocumento63 páginasFertilizationDheressaaAinda não há avaliações
- Jurnal Reading - Kulit - I Nyoman Fidry Octora Young Amukty PDFDocumento10 páginasJurnal Reading - Kulit - I Nyoman Fidry Octora Young Amukty PDFFidry YoungAinda não há avaliações
- KS3 Biology ReproductionDocumento22 páginasKS3 Biology ReproductionMEHDI MAICHOUFAinda não há avaliações
- Maternal & Child Health CareDocumento51 páginasMaternal & Child Health CareBhumi ChouhanAinda não há avaliações
- Maternal AssignmentDocumento3 páginasMaternal AssignmentJoule PeirreAinda não há avaliações