Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- Synthetic Approach ReportDocumento20 páginasSynthetic Approach ReportMarivic Diano100% (1)
- Return On InvestmentDocumento15 páginasReturn On InvestmentMarivic DianoAinda não há avaliações
- Wellness PowerpointDocumento28 páginasWellness PowerpointMarivic Diano0% (1)
- Light of HOPEDocumento33 páginasLight of HOPEMarivic DianoAinda não há avaliações
- BiologyDocumento42 páginasBiologyMarivic DianoAinda não há avaliações
- Why Did They Hide It FROM US: Remedy That Is 10,000 Times Stronger Than Chemotherapy!Documento2 páginasWhy Did They Hide It FROM US: Remedy That Is 10,000 Times Stronger Than Chemotherapy!Marivic DianoAinda não há avaliações
- Animal Tissues: Asia Technological School of Science and ArtsDocumento2 páginasAnimal Tissues: Asia Technological School of Science and ArtsMarivic DianoAinda não há avaliações
- Under The Guidance Of:: Dr. Sandeep Tandon Professor and Head of Dept. of PedodonticsDocumento79 páginasUnder The Guidance Of:: Dr. Sandeep Tandon Professor and Head of Dept. of PedodonticsMarivic DianoAinda não há avaliações
- Hospital Incident Command System (HICS) : Reported byDocumento42 páginasHospital Incident Command System (HICS) : Reported byMarivic DianoAinda não há avaliações
- Iv Regulation and Controlling DevicesDocumento21 páginasIv Regulation and Controlling DevicesMarivic DianoAinda não há avaliações
- Nurses' Perceived Job Related Stress and Job Satisfaction in Amman Private HospitalsDocumento31 páginasNurses' Perceived Job Related Stress and Job Satisfaction in Amman Private HospitalsMarivic Diano100% (1)
- Nurse To Colleagues: You Deserve A Break Today: by Tyler SmithDocumento2 páginasNurse To Colleagues: You Deserve A Break Today: by Tyler SmithMarivic DianoAinda não há avaliações
- Anatomy and Physiology of BVDocumento16 páginasAnatomy and Physiology of BVMarivic DianoAinda não há avaliações
- Suprising Truths About MotivationDocumento2 páginasSuprising Truths About MotivationMarivic DianoAinda não há avaliações
- Disaster Risk Management and MitigationDocumento5 páginasDisaster Risk Management and MitigationMarivic DianoAinda não há avaliações
- Fractures: (On Which We Will Likely Be Pimped)Documento66 páginasFractures: (On Which We Will Likely Be Pimped)Marivic DianoAinda não há avaliações
- Renal Cell Carcinoma - Nursing Considerations With The Use of Targeted TherapyDocumento50 páginasRenal Cell Carcinoma - Nursing Considerations With The Use of Targeted TherapyMarivic DianoAinda não há avaliações
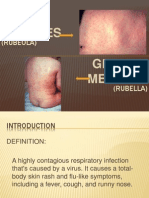
- MeaslesDocumento11 páginasMeaslesMarivic DianoAinda não há avaliações
- Palliative and Terminal CareDocumento78 páginasPalliative and Terminal CareMarivic DianoAinda não há avaliações
- Fluid and Electrolytes Report!!Documento20 páginasFluid and Electrolytes Report!!Marivic DianoAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Ce Mark - Application FormDocumento3 páginasCe Mark - Application Formrajivsinghal90Ainda não há avaliações
- Speaking Topics For Final ReviewDocumento3 páginasSpeaking Topics For Final ReviewNhư ÝAinda não há avaliações
- Fortune Falls - Lou VaneDocumento402 páginasFortune Falls - Lou VanetesteAinda não há avaliações
- 15 UrinalysisDocumento9 páginas15 UrinalysisJaney Ceniza تAinda não há avaliações
- Little Ann and Other Poems by Ann Taylor and Jane TaylorDocumento41 páginasLittle Ann and Other Poems by Ann Taylor and Jane Tayloralexa alexaAinda não há avaliações
- Pineapple PDFDocumento7 páginasPineapple PDFDestia AyuAinda não há avaliações
- Baxshin LABORATORY: Diagnostic Test and AnalysisDocumento1 páginaBaxshin LABORATORY: Diagnostic Test and AnalysisJabary HassanAinda não há avaliações
- EE2401 Power System Operation and ControlDocumento93 páginasEE2401 Power System Operation and ControlPrasanth GovindarajAinda não há avaliações
- POB Ch08Documento28 páginasPOB Ch08Anjum MalikAinda não há avaliações
- Chemrite SP 200Documento3 páginasChemrite SP 200ghazanfarAinda não há avaliações
- Unmasking Pleural Mesothelioma: A Silent ThreatDocumento11 páginasUnmasking Pleural Mesothelioma: A Silent ThreatCathenna DesuzaAinda não há avaliações
- 8953-Specifications For Doosan Man 9l21 31Documento7 páginas8953-Specifications For Doosan Man 9l21 31Bae Juyeon100% (1)
- Insulating Oil TestingDocumento6 páginasInsulating Oil TestingnasrunAinda não há avaliações
- 5070 s14 QP 11Documento16 páginas5070 s14 QP 11OsamaRahimAinda não há avaliações
- DTC P1602 Deterioration of Battery: DescriptionDocumento5 páginasDTC P1602 Deterioration of Battery: DescriptionEdy SudarsonoAinda não há avaliações
- Cisco - Level 45Documento1 páginaCisco - Level 45vithash shanAinda não há avaliações
- Guimbungan, Core Competency Module 1 - Part 3 PDFDocumento11 páginasGuimbungan, Core Competency Module 1 - Part 3 PDFSharlyne K. GuimbunganAinda não há avaliações
- NASA ISS Expedition 2 Press KitDocumento27 páginasNASA ISS Expedition 2 Press KitOrion2015Ainda não há avaliações
- The Brew Your Own Big Book of Clone Recipe - Brew Your OwnDocumento716 páginasThe Brew Your Own Big Book of Clone Recipe - Brew Your OwnFrederico Ribeiro67% (3)
- Hema Lec HematopoiesisDocumento8 páginasHema Lec HematopoiesisWayne ErumaAinda não há avaliações
- طبى 145Documento2 páginasطبى 145Yazan AbuFarhaAinda não há avaliações
- Contemporary ImageDocumento43 páginasContemporary ImageProf. L100% (1)
- AUDCISE Unit 1 WorksheetsDocumento2 páginasAUDCISE Unit 1 WorksheetsMarjet Cis QuintanaAinda não há avaliações
- Celitron ISS 25L - Product Spec Sheet V 2.1 enDocumento9 páginasCelitron ISS 25L - Product Spec Sheet V 2.1 enyogadwiprasetyo8_161Ainda não há avaliações
- Injection Analyzer Electronic Unit enDocumento67 páginasInjection Analyzer Electronic Unit enmayralizbethbustosAinda não há avaliações
- Rotary Vane PumpsDocumento7 páginasRotary Vane PumpshebsonbezerraAinda não há avaliações
- InotroposDocumento4 páginasInotroposjuan camiloAinda não há avaliações
- HOPE 3-Module 8-Week 5-6Documento9 páginasHOPE 3-Module 8-Week 5-6Freya SalorAinda não há avaliações
- Section IIDocumento8 páginasSection IIapi-471272376Ainda não há avaliações
- Region Iii - Central Luzon Padapada National High SchoolDocumento2 páginasRegion Iii - Central Luzon Padapada National High SchoolRotipAinda não há avaliações