Você também pode gostar
- Sample Letter of Medical NecessityDocumento4 páginasSample Letter of Medical NecessityGregory RussellAinda não há avaliações
- Miscellaneous For FinalsDocumento30 páginasMiscellaneous For Finalsjames.a.blairAinda não há avaliações
- Drug Adult Dose Child Dose Precautions and ContraindicationsDocumento9 páginasDrug Adult Dose Child Dose Precautions and ContraindicationsanshulAinda não há avaliações
- Road Map To Nclex - 2019 PCPDocumento422 páginasRoad Map To Nclex - 2019 PCPronDITCHvon Salindo100% (1)
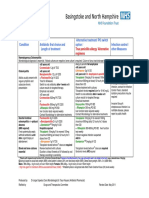
- Bacterial Meningitis HSV Encephalitis: Therapeutic Guidelines AntibioticDocumento2 páginasBacterial Meningitis HSV Encephalitis: Therapeutic Guidelines AntibioticBetari DhiraAinda não há avaliações
- Antibiotic Policy 2014Documento32 páginasAntibiotic Policy 2014shah007zaadAinda não há avaliações
- Guidelines For First-Line Empirical Antibiotic Therapy in AdultsDocumento1 páginaGuidelines For First-Line Empirical Antibiotic Therapy in AdultsAnonymous s4yarxAinda não há avaliações
- NAG Urinary Tract InfectionsDocumento14 páginasNAG Urinary Tract InfectionsJun JimenezAinda não há avaliações
- Max Fax Surgical GuidanceDocumento1 páginaMax Fax Surgical GuidanceMax FaxAinda não há avaliações
- E A G - SCH: Mpiric Ntibiotic UidelinesDocumento6 páginasE A G - SCH: Mpiric Ntibiotic UidelinesPulseWangminAinda não há avaliações
- Empiric Antibiotic Guidelines For Paediatric Intensive Care Unit (PICU)Documento7 páginasEmpiric Antibiotic Guidelines For Paediatric Intensive Care Unit (PICU)Benny Chris TantoAinda não há avaliações
- Internal Abdominal Infection Treatment ProtocolDocumento9 páginasInternal Abdominal Infection Treatment Protocolhatem newishyAinda não há avaliações
- Management of Healthcare-Associated Pneumonia (HCAP) in AdultsDocumento3 páginasManagement of Healthcare-Associated Pneumonia (HCAP) in Adultstheseus5Ainda não há avaliações
- 9 Drug StudyDocumento11 páginas9 Drug StudyJessa Mae Mauricio CastilloAinda não há avaliações
- Pocket Guide June2013 PDFDocumento2 páginasPocket Guide June2013 PDFSergeyGruntov100% (1)
- Febrile NeutropeniaDocumento3 páginasFebrile Neutropeniatheseus5Ainda não há avaliações
- SQC ABx Guidelines 2-21-2011 PDFDocumento2 páginasSQC ABx Guidelines 2-21-2011 PDFMinh SteveAinda não há avaliações
- Gui Iia Uk PDFDocumento2 páginasGui Iia Uk PDFluckevAinda não há avaliações
- Antibiotic Prophylaxis in Gustilo Grade I To III Open Fractures of The Lower LimbV5 - April18th2012Documento1 páginaAntibiotic Prophylaxis in Gustilo Grade I To III Open Fractures of The Lower LimbV5 - April18th2012Yopi ArdhiaswariAinda não há avaliações
- Central Nervous System InfectionsDocumento9 páginasCentral Nervous System InfectionsSaddamAinda não há avaliações
- Empiric Treatment Guidelines Common InfectionsDocumento9 páginasEmpiric Treatment Guidelines Common InfectionsShiza Batool100% (1)
- TASH Empirical Antibiotic Treatment Guidelines - 2018 Hospital and Ventilator Associated Pneumonia (HAP and VAP)Documento2 páginasTASH Empirical Antibiotic Treatment Guidelines - 2018 Hospital and Ventilator Associated Pneumonia (HAP and VAP)ጉራማይሌ TubeAinda não há avaliações
- Guide Paed Bone JNTDocumento11 páginasGuide Paed Bone JNTDorica GiurcaAinda não há avaliações
- Cilastati Imipenem Drug InfoDocumento19 páginasCilastati Imipenem Drug InfoCosmina GeorgianaAinda não há avaliações
- NAG Central Nervous System Infections As of Nov 2017Documento9 páginasNAG Central Nervous System Infections As of Nov 2017Rhod Bernaldez EstaAinda não há avaliações
- Antibiotic Hospital ManDocumento1 páginaAntibiotic Hospital Manarshiya.manasekiAinda não há avaliações
- Vancomycin & Vancomycin Resistant Enterococci: Abdullah M. Kharbosh, B.SC., PharmDocumento78 páginasVancomycin & Vancomycin Resistant Enterococci: Abdullah M. Kharbosh, B.SC., Pharmkharbosham100% (1)
- Perioperative Antimicrobial Prophylaxis Guidelines For Adult and Pediatric PatientsDocumento2 páginasPerioperative Antimicrobial Prophylaxis Guidelines For Adult and Pediatric Patientsihtisham1Ainda não há avaliações
- Bone and Joint Infections BNHFT 2010 PDFDocumento3 páginasBone and Joint Infections BNHFT 2010 PDFDanissa Fidia PuteriAinda não há avaliações
- 2012 Aug IMG Poster 165760a SepsisDocumento1 página2012 Aug IMG Poster 165760a SepsisTeng Huei LeeAinda não há avaliações
- Azithromycin Monograph - PaediatricDocumento7 páginasAzithromycin Monograph - PaediatrictynAinda não há avaliações
- Sepsis and Catheter Infections: Early Conversion From IV To Oral AntibioticsDocumento4 páginasSepsis and Catheter Infections: Early Conversion From IV To Oral AntibioticsChaim HerreraAinda não há avaliações
- CAP CURB-65 GuidelinesDocumento1 páginaCAP CURB-65 GuidelinesAndy LoakAinda não há avaliações
- NAG Sexually Transmitted InfectionsDocumento24 páginasNAG Sexually Transmitted InfectionsJun JimenezAinda não há avaliações
- Antibiotics in NeurosurgeryDocumento12 páginasAntibiotics in Neurosurgerylouglee9174100% (1)
- GentDocumento2 páginasGentOxford666Ainda não há avaliações
- GDL Fever OncologyDocumento16 páginasGDL Fever OncologyZaini GhazaliAinda não há avaliações
- Antibiotic PolicyDocumento4 páginasAntibiotic PolicyGAYATHIRIAinda não há avaliações
- Acute Pyelonephritis Treatment & Management: Approach ConsiderationsDocumento4 páginasAcute Pyelonephritis Treatment & Management: Approach ConsiderationsPeter InocandoAinda não há avaliações
- Habits Are Some of The Strategies RecommendedDocumento30 páginasHabits Are Some of The Strategies Recommendedmd.dascalescu2486Ainda não há avaliações
- AHS антибиотики рекомендацDocumento42 páginasAHS антибиотики рекомендацMaksym DemianchukAinda não há avaliações
- IIIiSTD Treatment ChartDocumento5 páginasIIIiSTD Treatment Chartjessieca liusenAinda não há avaliações
- Management of The Complications of Nephrotic SyndromeDocumento6 páginasManagement of The Complications of Nephrotic SyndromeRagabi RezaAinda não há avaliações
- Paediatric Cardiac Surgical Antibiotic Prophylaxis: PurposeDocumento9 páginasPaediatric Cardiac Surgical Antibiotic Prophylaxis: PurposeZamzam DomaAinda não há avaliações
- Medicine RotatationbookletDocumento20 páginasMedicine RotatationbookletJanelle JosephsAinda não há avaliações
- Id 397 TeicoplaninDocumento2 páginasId 397 TeicoplaninStacey WoodsAinda não há avaliações
- Guideline: Antibiotic Drug Monitoring: Aminoglycosides and GlycopeptidesDocumento8 páginasGuideline: Antibiotic Drug Monitoring: Aminoglycosides and GlycopeptidesKenRodulfReyesVillaruelAinda não há avaliações
- Ovarian Cancer Treatment Regimens - Print Article - Cancer Therapy AdvisorDocumento5 páginasOvarian Cancer Treatment Regimens - Print Article - Cancer Therapy AdvisorAnonymous g1hIPZAinda não há avaliações
- Champ Empiric Antimicrobial Guidelines: Consider Investigation and Treatment For Pertussis And/Or Chlamydia TrachomatisDocumento2 páginasChamp Empiric Antimicrobial Guidelines: Consider Investigation and Treatment For Pertussis And/Or Chlamydia TrachomatistynAinda não há avaliações
- AIIMS Issues New Guidelines For Treatment of CovidDocumento7 páginasAIIMS Issues New Guidelines For Treatment of Covidsenthil kumarAinda não há avaliações
- 1 s2.0 S0163445316300123 MainDocumento2 páginas1 s2.0 S0163445316300123 MainZara SaeedAinda não há avaliações
- Ob Gyn AdultDocumento3 páginasOb Gyn AdultHarshit RastogiAinda não há avaliações
- AIIMS Issues New Guidelines For Treatment of Covid-19 Cases: (Enter Post Title Here)Documento7 páginasAIIMS Issues New Guidelines For Treatment of Covid-19 Cases: (Enter Post Title Here)senthil kumarAinda não há avaliações
- Profil Ampicillin SulbactamDocumento12 páginasProfil Ampicillin SulbactamasriAinda não há avaliações
- NAG Upper Respiratory Tract InfectionsDocumento20 páginasNAG Upper Respiratory Tract InfectionsJun JimenezAinda não há avaliações
- Pneumonia Treatment Algorithm With Addendum For Aspiration 2015-2016.01.19Documento2 páginasPneumonia Treatment Algorithm With Addendum For Aspiration 2015-2016.01.19Irsalina TriastutikAinda não há avaliações
- Terapi AnakDocumento10 páginasTerapi AnakIka KrastanayaAinda não há avaliações
- Antimicrobial Treatment Guidelines For Common Infections enDocumento111 páginasAntimicrobial Treatment Guidelines For Common Infections enRoofia VahedianAinda não há avaliações
- Antibiotic Surgical Prophylaxis Protocol SMH October 2018 UpdateDocumento7 páginasAntibiotic Surgical Prophylaxis Protocol SMH October 2018 Updatessrnew2023Ainda não há avaliações
- CPG Typhoid Fever 2017Documento11 páginasCPG Typhoid Fever 2017Tam Adrian Aya-ayAinda não há avaliações
- Top Trials in Gastroenterology & HepatologyNo EverandTop Trials in Gastroenterology & HepatologyNota: 4.5 de 5 estrelas4.5/5 (7)
- NCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!No EverandNCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!Nota: 5 de 5 estrelas5/5 (4)
- Toacs Surgical Trainees 2009 ADocumento15 páginasToacs Surgical Trainees 2009 AAnonymous bzHRfZzv100% (1)
- PHE For AdolescentsDocumento26 páginasPHE For AdolescentsSanifa MedAinda não há avaliações
- Medication Guide Remicade (Rem-Eh-Kaid) (Infliximab) : Before Starting REMICADE, Tell Your Doctor If YouDocumento5 páginasMedication Guide Remicade (Rem-Eh-Kaid) (Infliximab) : Before Starting REMICADE, Tell Your Doctor If YouHakkaniAinda não há avaliações
- Madhavi Venigalla, MD Medical Oncology/Hematology Lakeland Regional Cancer CenterDocumento26 páginasMadhavi Venigalla, MD Medical Oncology/Hematology Lakeland Regional Cancer Centerdikyhardiyansyah2Ainda não há avaliações
- Antenatal Care (ANC) : For Year III Regular Midwifery StudentsDocumento76 páginasAntenatal Care (ANC) : For Year III Regular Midwifery StudentsAman KifleAinda não há avaliações
- New ListDocumento3 páginasNew ListKumar MakwanaAinda não há avaliações
- Europass CV 20141120 Gjoka enDocumento2 páginasEuropass CV 20141120 Gjoka enArdit ZotajAinda não há avaliações
- Shock ExamDocumento3 páginasShock ExamMilagros Fuertes Yosores100% (1)
- GR No. 168512 Garcia v. Salvador, 20 March 2007Documento2 páginasGR No. 168512 Garcia v. Salvador, 20 March 2007Niña VillegasAinda não há avaliações
- Methods of EpidemiologyDocumento28 páginasMethods of EpidemiologyAlice sylviya SamuelAinda não há avaliações
- Single Visit EndodonticsDocumento5 páginasSingle Visit EndodonticsSreena VenugopalanAinda não há avaliações
- Laboratory Test Report: Male 30 YearsDocumento3 páginasLaboratory Test Report: Male 30 YearsMohammed MoizuddinAinda não há avaliações
- Medical ATO Ukraine, April, 2015Documento27 páginasMedical ATO Ukraine, April, 2015Patrick Chellew100% (1)
- Tablanza-Finals Activity 1 (Lab)Documento3 páginasTablanza-Finals Activity 1 (Lab)trust nobodyAinda não há avaliações
- AOM CPG RevisedDocumento26 páginasAOM CPG Revisedmefav7778520Ainda não há avaliações
- SCHITOSOMIASISDocumento8 páginasSCHITOSOMIASISxteph04Ainda não há avaliações
- Ovr New MohDocumento2 páginasOvr New MohhyAinda não há avaliações
- Facet Joint Pain-Advances in Patient Selection and TreatmentDocumento16 páginasFacet Joint Pain-Advances in Patient Selection and TreatmentthiagoAinda não há avaliações
- 321Z3D2 0KD8D6L7P001F6G PDFDocumento13 páginas321Z3D2 0KD8D6L7P001F6G PDFNBC MontanaAinda não há avaliações
- ID Identifikasi Wilayah Dengan PermasalahanDocumento10 páginasID Identifikasi Wilayah Dengan PermasalahanDhery MursalAinda não há avaliações
- Etiology and Pathogenesis of The Congenital Pneumonia in Newborns Literature Review Part 1 PDFDocumento4 páginasEtiology and Pathogenesis of The Congenital Pneumonia in Newborns Literature Review Part 1 PDFGolden DawnAinda não há avaliações
- New Laser Diabetic RetinopatiDocumento10 páginasNew Laser Diabetic RetinopatiIndah KurniawatiAinda não há avaliações
- Factors Associated With The Use of Herbal Medicine Among Pregnant Women in The Nkwanta North and South Districts of Oti Region, Ghana.Documento68 páginasFactors Associated With The Use of Herbal Medicine Among Pregnant Women in The Nkwanta North and South Districts of Oti Region, Ghana.Samuel CrewzAinda não há avaliações
- ICD 10 Dalam ExcelDocumento103 páginasICD 10 Dalam ExcelJumpa Utama AmrannurAinda não há avaliações
- Lecture-11 Breech PresentationDocumento27 páginasLecture-11 Breech PresentationMadhu Sudhan PandeyaAinda não há avaliações
- Original PDF Complementary and Alternative Therapies For Nursing Practice 5th PDFDocumento41 páginasOriginal PDF Complementary and Alternative Therapies For Nursing Practice 5th PDFpaul.shropshire768100% (37)
- Colonization V InfectionDocumento1 páginaColonization V InfectionVerina Logito LoAinda não há avaliações
- Orthodontics-Gurkeerat Singh, 2nd EditionDocumento704 páginasOrthodontics-Gurkeerat Singh, 2nd Editionkeralaapple85% (34)