Você também pode gostar
- King Rush MoreDocumento1 páginaKing Rush MoreawuahbohAinda não há avaliações
- Oop Say You Know MeDocumento1 páginaOop Say You Know MeawuahbohAinda não há avaliações
- Pharm NclexDocumento9 páginasPharm NclexawuahbohAinda não há avaliações
- Article For CET CHFDocumento5 páginasArticle For CET CHFawuahbohAinda não há avaliações
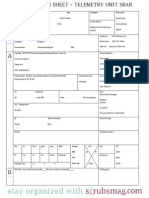
- Nurse Brain Sheet Telemetry Unit SBARDocumento1 páginaNurse Brain Sheet Telemetry Unit SBARvsosa624Ainda não há avaliações
- Massachusetts Department of Public HealthDocumento24 páginasMassachusetts Department of Public HealthawuahbohAinda não há avaliações
- HandOff SampleToolsDocumento9 páginasHandOff SampleToolsOllie EvansAinda não há avaliações
- The BSN Job Search: Interview Preparation: Telling Your StoryDocumento25 páginasThe BSN Job Search: Interview Preparation: Telling Your StoryawuahbohAinda não há avaliações
- Article For JournalDocumento6 páginasArticle For JournalawuahbohAinda não há avaliações
- NCLEX Random FactsDocumento34 páginasNCLEX Random FactsLegnaMary100% (8)
- Probability of A or B and A and B-1Documento2 páginasProbability of A or B and A and B-1awuahbohAinda não há avaliações
- Middle Age Adult Health History Assignment Guidelines N315 Fall 2013Documento23 páginasMiddle Age Adult Health History Assignment Guidelines N315 Fall 2013awuahbohAinda não há avaliações
- EBP Article 1Documento11 páginasEBP Article 1awuahbohAinda não há avaliações
- PolypharmacyDocumento24 páginasPolypharmacySurina Zaman HuriAinda não há avaliações
- Drugs NclexDocumento30 páginasDrugs Nclexawuahboh100% (1)
- EBP Article 3Documento6 páginasEBP Article 3awuahbohAinda não há avaliações
- Tips On Answering NclexDocumento4 páginasTips On Answering NclexawuahbohAinda não há avaliações
- Random FactsDocumento338 páginasRandom Factscyram81100% (1)
- Critical Thinking StrategiesDocumento3 páginasCritical Thinking StrategiesawuahbohAinda não há avaliações
- Therapeutic CommunicationDocumento1 páginaTherapeutic CommunicationawuahbohAinda não há avaliações
- Does Prospective Payment Increase Hospital (In) Efficiency? Evidence From The Swiss Hospital SectorDocumento24 páginasDoes Prospective Payment Increase Hospital (In) Efficiency? Evidence From The Swiss Hospital SectorawuahbohAinda não há avaliações
- ENT Throat and EsophagusDocumento41 páginasENT Throat and EsophagusMUHAMMAD HASAN NAGRAAinda não há avaliações
- Parkland formula and rule of 9Documento8 páginasParkland formula and rule of 9awuahbohAinda não há avaliações
- STDA VaricealDocumento8 páginasSTDA VaricealDeisy de JesusAinda não há avaliações
- Article For CET CHFDocumento5 páginasArticle For CET CHFawuahbohAinda não há avaliações
- Article For Jouranal 2 (498P)Documento5 páginasArticle For Jouranal 2 (498P)awuahbohAinda não há avaliações
- Patient Report FormDocumento1 páginaPatient Report FormawuahbohAinda não há avaliações
- Debate 3 Youth Incarceration in Adult PrisonsDocumento6 páginasDebate 3 Youth Incarceration in Adult PrisonsawuahbohAinda não há avaliações
- Article For Journal 4-18-14Documento8 páginasArticle For Journal 4-18-14awuahbohAinda não há avaliações
- Article For JournalDocumento6 páginasArticle For JournalawuahbohAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- CHN Assignment (Community Health Nursing)Documento21 páginasCHN Assignment (Community Health Nursing)binjuAinda não há avaliações
- Frankel 4Documento13 páginasFrankel 4Fabian BarretoAinda não há avaliações
- Generic PfPan Job AidDocumento1 páginaGeneric PfPan Job AidSilvia SatoAinda não há avaliações
- LearnEnglish Reading B2 A Plastic Ocean A Film ReviewDocumento5 páginasLearnEnglish Reading B2 A Plastic Ocean A Film ReviewSerly FimasariAinda não há avaliações
- Personal Trainer TextDocumento97 páginasPersonal Trainer Textwuddafren100% (1)
- Introduction To Environmental Health LectureDocumento41 páginasIntroduction To Environmental Health LectureJudy OuAinda não há avaliações
- Slide PPT PrismaDocumento31 páginasSlide PPT PrismaUlul Azmi AdnanAinda não há avaliações
- Direct-To-Implant Breast ReconstructionDocumento3 páginasDirect-To-Implant Breast ReconstructionCarlos Javier SolorzaAinda não há avaliações
- Pq-Unocal Csms '03Documento15 páginasPq-Unocal Csms '03Ismail Hamzah Azmatkhan Al-husainiAinda não há avaliações
- Nutrition Counseling And Dietary InstructionDocumento5 páginasNutrition Counseling And Dietary Instructionnicoleangela ubasroselloAinda não há avaliações
- 2016 3 23 9 12 47tapchi-Dhdn-So12 (97) .2015-Color-WebDocumento128 páginas2016 3 23 9 12 47tapchi-Dhdn-So12 (97) .2015-Color-WebThọ Nguyễn Văn100% (1)
- Penicillin: Weird RPG Zine Issue 1 F A L L 2 0 1 9Documento16 páginasPenicillin: Weird RPG Zine Issue 1 F A L L 2 0 1 9iAinda não há avaliações
- Human Resources Manager or Human Resources Director or Sr. HR BuDocumento2 páginasHuman Resources Manager or Human Resources Director or Sr. HR Buapi-77982767Ainda não há avaliações
- Commentary: Novel Application For G Protein - Biased Mu Opioid Receptor Agonists in Opioid Relapse PreventionDocumento2 páginasCommentary: Novel Application For G Protein - Biased Mu Opioid Receptor Agonists in Opioid Relapse PreventionIntan AyuAinda não há avaliações
- What is pancytopenia and its causesDocumento33 páginasWhat is pancytopenia and its causesDabogski FranceAinda não há avaliações
- AA PamphletDocumento52 páginasAA PamphletCarmen UleiaAinda não há avaliações
- Eclampsia Nursing Care Plan - Altered Tissue PerfusionDocumento2 páginasEclampsia Nursing Care Plan - Altered Tissue PerfusionCyrus De Asis84% (32)
- Housing ContractDocumento5 páginasHousing Contractapi-225453429100% (1)
- Fire Retardant Research PaperDocumento2 páginasFire Retardant Research Paperapi-318759920Ainda não há avaliações
- 4th Quarter CAPSTONEDocumento30 páginas4th Quarter CAPSTONEWallace RamosAinda não há avaliações
- USMLE High YieldDocumento8 páginasUSMLE High YieldNajia ChoudhuryAinda não há avaliações
- TRS 957 (2010) - Annex 3 - WHO GMP For Pharmaceutical Products Containing Hazardous SubstancesDocumento17 páginasTRS 957 (2010) - Annex 3 - WHO GMP For Pharmaceutical Products Containing Hazardous SubstancesQuang Hiếu NgôAinda não há avaliações
- Assisted SuicideDocumento30 páginasAssisted SuicideAlex Mini AndraAinda não há avaliações
- Ethical Decision Making in ResearchDocumento2 páginasEthical Decision Making in ResearchChandraKurniawanAinda não há avaliações
- Colegio de San Gabriel Arcangel, Inc.: READING REPORT in - Complementary and Alternative MedicineDocumento2 páginasColegio de San Gabriel Arcangel, Inc.: READING REPORT in - Complementary and Alternative MedicineJonille EchevarriaAinda não há avaliações
- 1 s2.0 S2772569323000026 MainDocumento8 páginas1 s2.0 S2772569323000026 MainAditya RizkyAinda não há avaliações
- Attachment Theory and FathersDocumento16 páginasAttachment Theory and FathersGraceAinda não há avaliações
- Surya Namaskar BenefitsDocumento16 páginasSurya Namaskar BenefitsMillion Dollar KnowledgeAinda não há avaliações
- Evidence Based Practices For Young Children With AutismDocumento11 páginasEvidence Based Practices For Young Children With Autismkonyicska_kingaAinda não há avaliações
- Paedo Don TicsDocumento103 páginasPaedo Don TicsIana RusuAinda não há avaliações