Você também pode gostar
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Deer Exercise For MenDocumento3 páginasThe Deer Exercise For Menkbarn389100% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Metabolic Encephalopathies and Delirium: Panayiotis N. Varelas, MD, PHDDocumento34 páginasMetabolic Encephalopathies and Delirium: Panayiotis N. Varelas, MD, PHDjorge_suoAinda não há avaliações
- Play TherapyDocumento4 páginasPlay TherapyAnita Hani ChristinaAinda não há avaliações
- Buku BacaanDocumento329 páginasBuku BacaanNurhasni FebrianiAinda não há avaliações
- ModifiersDocumento8 páginasModifiersKarna Palanivelu100% (6)
- Homoeopathic Treatment of Parkinson DieseDocumento23 páginasHomoeopathic Treatment of Parkinson DieseNidhi SrivastavaAinda não há avaliações
- Neuro DMS3 FDocumento142 páginasNeuro DMS3 FVicente CáceresAinda não há avaliações
- Cary Blair Transport MediumDocumento1 páginaCary Blair Transport MediumVijeyachandhar DorairajAinda não há avaliações
- Arginine Stimulation Test For GHRHDocumento2 páginasArginine Stimulation Test For GHRHVijeyachandhar DorairajAinda não há avaliações
- No 25 Bharathi Nagar Kamarajar Road Uppilipalayam Post Coimbatore Pincode: 641015 Contact No: 9092912220Documento1 páginaNo 25 Bharathi Nagar Kamarajar Road Uppilipalayam Post Coimbatore Pincode: 641015 Contact No: 9092912220Vijeyachandhar DorairajAinda não há avaliações
- FNH LiverDocumento10 páginasFNH LiverVijeyachandhar DorairajAinda não há avaliações
- Pgi Mdms ProspectusDocumento16 páginasPgi Mdms ProspectusVijeyachandhar DorairajAinda não há avaliações
- Nbme 1Documento39 páginasNbme 1rockAinda não há avaliações
- Skeletal Dysplasia3 PDFDocumento7 páginasSkeletal Dysplasia3 PDFVijeyachandhar DorairajAinda não há avaliações
- Faq Aiims PG July 2015Documento6 páginasFaq Aiims PG July 2015Vijeyachandhar DorairajAinda não há avaliações
- BehaviourismDocumento9 páginasBehaviourismVijeyachandhar DorairajAinda não há avaliações
- WHO Dengue Guidelines 2013Documento160 páginasWHO Dengue Guidelines 2013Jason MirasolAinda não há avaliações
- Transthoracic EcocardiographyDocumento5 páginasTransthoracic EcocardiographyVijeyachandhar DorairajAinda não há avaliações
- Histone Modifications12Documento70 páginasHistone Modifications12Vijeyachandhar DorairajAinda não há avaliações
- Q Rate of Removal of Substance: F GC BS GCDocumento2 páginasQ Rate of Removal of Substance: F GC BS GCVijeyachandhar DorairajAinda não há avaliações
- 2009 CMT Framework (Revised Aug 2012)Documento166 páginas2009 CMT Framework (Revised Aug 2012)Vijeyachandhar DorairajAinda não há avaliações
- Arc Ureteral StonesDocumento79 páginasArc Ureteral StonesVijeyachandhar DorairajAinda não há avaliações
- Nucleotide Excision Repair Defect and DiseasesDocumento8 páginasNucleotide Excision Repair Defect and DiseasesVijeyachandhar DorairajAinda não há avaliações
- Clinical Review: Systemic Lupus ErythematosusDocumento5 páginasClinical Review: Systemic Lupus ErythematosusVijeyachandhar DorairajAinda não há avaliações
- Hepatorenal SyndromeDocumento14 páginasHepatorenal SyndromeVijeyachandhar DorairajAinda não há avaliações
- All ChildrenDocumento5 páginasAll ChildrenVijeyachandhar DorairajAinda não há avaliações
- Measurement of Renal Function in PracticeDocumento5 páginasMeasurement of Renal Function in PracticeVijeyachandhar DorairajAinda não há avaliações
- Venous ThromboliskDocumento5 páginasVenous ThromboliskVijeyachandhar DorairajAinda não há avaliações
- Op PoisoningDocumento6 páginasOp PoisoningVijeyachandhar DorairajAinda não há avaliações
- Hereditary HemochromatosisDocumento6 páginasHereditary HemochromatosisVijeyachandhar DorairajAinda não há avaliações
- BMJ 335 7628 CR 01037 PDFDocumento5 páginasBMJ 335 7628 CR 01037 PDFDescargasExposicionesAinda não há avaliações
- Lower Gi Bleeding in AdultsDocumento7 páginasLower Gi Bleeding in AdultsVijeyachandhar DorairajAinda não há avaliações
- H Pylori Infection TreatmentDocumento5 páginasH Pylori Infection TreatmentVijeyachandhar DorairajAinda não há avaliações
- Acute Respiratory Distress Syndrome: Clinical ReviewDocumento6 páginasAcute Respiratory Distress Syndrome: Clinical ReviewVijeyachandhar DorairajAinda não há avaliações
- Benign Prostatic Hyperplasia. - Diagnosis: Clinical ReviewDocumento4 páginasBenign Prostatic Hyperplasia. - Diagnosis: Clinical ReviewVijeyachandhar DorairajAinda não há avaliações
- Cocci Dio I o MycosisDocumento7 páginasCocci Dio I o MycosisVijeyachandhar DorairajAinda não há avaliações
- Darwish Badran CVDocumento14 páginasDarwish Badran CVMedicsindex Telepin SlidecaseAinda não há avaliações
- Current Practice of Occupational Therapy For Children With AutismDocumento8 páginasCurrent Practice of Occupational Therapy For Children With AutismNovia RambakAinda não há avaliações
- Oncology Nursing: Detection and Prevention of CancerDocumento14 páginasOncology Nursing: Detection and Prevention of CancerEdwin Delos Reyes AbuAinda não há avaliações
- Abscess Incision and Drainage NEJMDocumento4 páginasAbscess Incision and Drainage NEJMMarcela CharryAinda não há avaliações
- Kellian-Hunte hw410 Unit 9 - Assignment-Stress - Critical Issues in Management and PreventionDocumento8 páginasKellian-Hunte hw410 Unit 9 - Assignment-Stress - Critical Issues in Management and Preventionapi-616884609Ainda não há avaliações
- Drug Study For HELLP SyndromeDocumento19 páginasDrug Study For HELLP SyndromeRosemarie CarpioAinda não há avaliações
- Contact Dermatitis: What Are Some Common Causes of Contact Dermatitis?Documento13 páginasContact Dermatitis: What Are Some Common Causes of Contact Dermatitis?Hanna AthirahAinda não há avaliações
- 3.02 Learning and Memory: ExamplesDocumento2 páginas3.02 Learning and Memory: ExamplesMarkayla HinesAinda não há avaliações
- Simplified ACLS AlgorithmDocumento1 páginaSimplified ACLS AlgorithmBrianAinda não há avaliações
- Speak Truth To Power in KI-Media Series - Gabor Gombos (Hungary) "Mental Disability Rights"Documento8 páginasSpeak Truth To Power in KI-Media Series - Gabor Gombos (Hungary) "Mental Disability Rights"kilettersAinda não há avaliações
- Amlodipine CPDocumento2 páginasAmlodipine CPRose EchevarriaAinda não há avaliações
- FS13 PolycythemiaVera FactSheetDocumento7 páginasFS13 PolycythemiaVera FactSheetMala 'emyu' UmarAinda não há avaliações
- Practice Guidelines For Telemental HealthDocumento51 páginasPractice Guidelines For Telemental HealthNataanatiAinda não há avaliações
- Satara ODF ReportDocumento27 páginasSatara ODF ReportPrashant JadhavAinda não há avaliações
- Interferential Stimulation For The Treatment of Musculoskeletal PainDocumento15 páginasInterferential Stimulation For The Treatment of Musculoskeletal PainCTAFDocumentsAinda não há avaliações
- Which of The Following Complications Is Thought To Be The Most Common Cause of AppendicitisDocumento15 páginasWhich of The Following Complications Is Thought To Be The Most Common Cause of AppendicitisKristine CastilloAinda não há avaliações
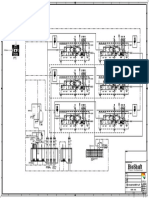
- P&ID - STP-Yanbu SWCC (6units)Documento1 páginaP&ID - STP-Yanbu SWCC (6units)Ashraf BayomiAinda não há avaliações
- Da Vinci: Robotic SurgeryDocumento2 páginasDa Vinci: Robotic SurgeryMani DhamodharanAinda não há avaliações
- Tuberculous Spondylitis After Vertebral Augmentation: A Case Report With A Literature ReviewDocumento9 páginasTuberculous Spondylitis After Vertebral Augmentation: A Case Report With A Literature ReviewHendra SalehAinda não há avaliações
- Pulmonary Medicine and Critical CareDocumento96 páginasPulmonary Medicine and Critical CaresarahamrdAinda não há avaliações
- The Use of Attar (Essential Oils) : Chamomile (Dry & Hot)Documento6 páginasThe Use of Attar (Essential Oils) : Chamomile (Dry & Hot)Ashraf DockratAinda não há avaliações
- Acute Pain Related To Inflammation and Distension of The Colon.Documento2 páginasAcute Pain Related To Inflammation and Distension of The Colon.JULIANNE BAYHONAinda não há avaliações
- Video Game TreatmentDocumento1 páginaVideo Game TreatmentYosi FestaAinda não há avaliações