Você também pode gostar
- I. Approach To Clinical Interviewing and DiagnosisDocumento6 páginasI. Approach To Clinical Interviewing and DiagnosisRoci ArceAinda não há avaliações
- Psychiatric Aspects of AIDSDocumento7 páginasPsychiatric Aspects of AIDSRoci ArceAinda não há avaliações
- The Assessment and Treatment of Sexual DysfunctionDocumento6 páginasThe Assessment and Treatment of Sexual DysfunctionRoci ArceAinda não há avaliações
- Psychiatric Disorders and PregnancyDocumento13 páginasPsychiatric Disorders and PregnancyRoci ArceAinda não há avaliações
- Adolescent Drug AbuseDocumento6 páginasAdolescent Drug AbuseRoci ArceAinda não há avaliações
- The Management of Chronic PainDocumento7 páginasThe Management of Chronic PainRoci ArceAinda não há avaliações
- Psychiatric Disorders in Primary Care SettingsDocumento4 páginasPsychiatric Disorders in Primary Care SettingsRoci ArceAinda não há avaliações
- Postpartum Psychiatryc DisordersDocumento6 páginasPostpartum Psychiatryc DisordersRoci ArceAinda não há avaliações
- Psychiatric Consultation in The General HospitalDocumento5 páginasPsychiatric Consultation in The General HospitalRoci ArceAinda não há avaliações
- Psychopharmacology For Elderly PatientsDocumento6 páginasPsychopharmacology For Elderly PatientsRoci ArceAinda não há avaliações
- Developmental Issues in Late LifeDocumento6 páginasDevelopmental Issues in Late LifeRoci ArceAinda não há avaliações
- Premenstrual Syndrome and Premenstrual Dysphoric DisorderDocumento9 páginasPremenstrual Syndrome and Premenstrual Dysphoric DisorderRoci ArceAinda não há avaliações
- Electroconvulsive TherapyDocumento6 páginasElectroconvulsive TherapyRoci ArceAinda não há avaliações
- Obsessive-Compulsive Disorder in Children and AdolescentsDocumento5 páginasObsessive-Compulsive Disorder in Children and AdolescentsRoci ArceAinda não há avaliações
- Principles of Child and Adolescent PsychopharmacologyDocumento10 páginasPrinciples of Child and Adolescent PsychopharmacologyRoci ArceAinda não há avaliações
- Medical Treatment of DepressionDocumento12 páginasMedical Treatment of DepressionRoci ArceAinda não há avaliações
- Encopresis and EnuresisDocumento10 páginasEncopresis and EnuresisRoci ArceAinda não há avaliações
- Conduct DisorderDocumento5 páginasConduct DisorderRoci ArceAinda não há avaliações
- Mood Stabilizers: Uses and Side EffectsDocumento9 páginasMood Stabilizers: Uses and Side EffectsRoci ArceAinda não há avaliações
- Autism Spectrum DisordersDocumento8 páginasAutism Spectrum DisordersRoci ArceAinda não há avaliações
- Understanding Medication InteractionDocumento6 páginasUnderstanding Medication InteractionRoci ArceAinda não há avaliações
- Attention Deficit-Hyperactivity DisorderDocumento8 páginasAttention Deficit-Hyperactivity DisorderRoci ArceAinda não há avaliações
- The Use of Stimulants in Psychiatric PracticeDocumento5 páginasThe Use of Stimulants in Psychiatric PracticeRoci Arce100% (1)
- Antipsychotic MedicationsDocumento8 páginasAntipsychotic MedicationsRoci ArceAinda não há avaliações
- Sedative-Hypnotic DrugsDocumento8 páginasSedative-Hypnotic DrugsRoci ArceAinda não há avaliações
- Group TherapyDocumento6 páginasGroup TherapyRoci ArceAinda não há avaliações
- Anxiety MedicationsDocumento4 páginasAnxiety MedicationsRoci ArceAinda não há avaliações
- Marital and Family TherapiesDocumento5 páginasMarital and Family TherapiesRoci ArceAinda não há avaliações
- Relaxation TrainingDocumento6 páginasRelaxation TrainingRoci ArceAinda não há avaliações
- Planned Brief PsychotherapyDocumento7 páginasPlanned Brief PsychotherapyRoci ArceAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Psychiatry and NeurologyDocumento114 páginasPsychiatry and Neurologyjames.a.blairAinda não há avaliações
- Personality Disorders ExplainedDocumento46 páginasPersonality Disorders ExplainedHafizi100% (1)
- Schizoobsessive Spectrum Disorders An UpdateDocumento15 páginasSchizoobsessive Spectrum Disorders An UpdateRubiAinda não há avaliações
- Mental Illness in FilmDocumento4 páginasMental Illness in FilmLosinginterestineverything HiAinda não há avaliações
- Activity Abnormal Personality Disorders Speed DatingDocumento2 páginasActivity Abnormal Personality Disorders Speed DatingJanie VandeBerg0% (1)
- MCMI IV Interpretation Webinar HandoutDocumento24 páginasMCMI IV Interpretation Webinar HandoutTejas ShahAinda não há avaliações
- HNS 107Documento95 páginasHNS 107claudette1882Ainda não há avaliações
- Abnormal Psych - Luna LovegoofDocumento6 páginasAbnormal Psych - Luna Lovegoofricha0% (1)
- Schizophrenia Spectrum and Other Psychotic DisorderDocumento14 páginasSchizophrenia Spectrum and Other Psychotic Disordereyesheild100% (1)
- DSM-IV and DSM-5 Criteria For The Personality Disorders 5-1-12Documento15 páginasDSM-IV and DSM-5 Criteria For The Personality Disorders 5-1-12ouestlechatdememeAinda não há avaliações
- Personality Disorder - WikipediaDocumento36 páginasPersonality Disorder - WikipediaAhmad Tohir Nasution100% (1)
- TUGASKUDocumento12 páginasTUGASKURetno Shofi WidianaAinda não há avaliações
- Psychological DisordersDocumento48 páginasPsychological Disordersapi-448144386100% (1)
- Mcmi IiiDocumento111 páginasMcmi Iiipemea200895% (19)
- PSY 408 - Unit Exam #4 With Answers (7-20-2023)Documento3 páginasPSY 408 - Unit Exam #4 With Answers (7-20-2023)Ashley TaylorAinda não há avaliações
- Disorder of Adult PersonalityDocumento71 páginasDisorder of Adult PersonalityodyAinda não há avaliações
- Adrian Raine Editor, Todd Lencz Editor, Sarnoff A. Mednick Editor Schizotypal Personality 2007Documento526 páginasAdrian Raine Editor, Todd Lencz Editor, Sarnoff A. Mednick Editor Schizotypal Personality 2007vero100% (2)
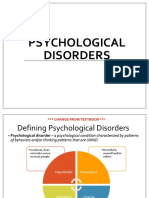
- Redefining Our Perceptions of What Constitutes Psychological DisordersDocumento21 páginasRedefining Our Perceptions of What Constitutes Psychological DisordersaKmaL100% (1)
- PD and ASDDocumento8 páginasPD and ASDKrol Amafo100% (1)
- Cluster A (Odd/eccentric) : Paranoid Schizoid SchizotypalDocumento4 páginasCluster A (Odd/eccentric) : Paranoid Schizoid SchizotypalnursekatieAinda não há avaliações
- Self, Solipsism, and Schizophrenic DelusionsDocumento21 páginasSelf, Solipsism, and Schizophrenic Delusionsjcrosby77Ainda não há avaliações
- Levy Johnson Personality Disorderschapterin APAHandbookof Clinical PsychologyfordistributionDocumento94 páginasLevy Johnson Personality Disorderschapterin APAHandbookof Clinical Psychologyfordistributionjavier ornelasAinda não há avaliações
- PERSONALITY DISORDERS: CLUSTERS A AND BDocumento58 páginasPERSONALITY DISORDERS: CLUSTERS A AND BJoanneMontalboAinda não há avaliações
- Prediction of Psychosis in Youth at High Clinical RiskDocumento20 páginasPrediction of Psychosis in Youth at High Clinical Risksaurav.das2030Ainda não há avaliações
- Argument Essay Rough DraftDocumento5 páginasArgument Essay Rough Draftapi-462047554Ainda não há avaliações
- Forensic Psychiatry PDFDocumento8 páginasForensic Psychiatry PDFleoqfb688gmail.com HernandezAinda não há avaliações
- Childhood Adversity and Personality Disorders Results From A Nationallyrepresentative Population-Based Study - Afifi 2016 PDFDocumento9 páginasChildhood Adversity and Personality Disorders Results From A Nationallyrepresentative Population-Based Study - Afifi 2016 PDFRodrigo Romo MuñozAinda não há avaliações
- MMPI 2 y MCMI IIDocumento10 páginasMMPI 2 y MCMI IIErika Arroyo100% (1)
- Personality Disorder TestDocumento2 páginasPersonality Disorder Testmagjrshomei100% (1)
- The Three Clusters of Personality DisordersDocumento3 páginasThe Three Clusters of Personality DisordersRaffAinda não há avaliações