Você também pode gostar
- Li 2011-smDocumento14 páginasLi 2011-smCLPHtheoryAinda não há avaliações
- RAS Role in Chronic Inflammation and AtherosclerosisDocumento11 páginasRAS Role in Chronic Inflammation and AtherosclerosisSukma EffendyAinda não há avaliações
- Mattias Carlström, Christopher S. Wilcox and William J. WelchDocumento7 páginasMattias Carlström, Christopher S. Wilcox and William J. WelchJulienne InostrozaAinda não há avaliações
- Endotelin and Renal IonDocumento15 páginasEndotelin and Renal IonSelly Cintya GusmanAinda não há avaliações
- Role of Thioredoxin-Interacting Protein in Mediating Endothelial Dysfunction in HypertensionDocumento13 páginasRole of Thioredoxin-Interacting Protein in Mediating Endothelial Dysfunction in HypertensionLeidy LambertinezAinda não há avaliações
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocumento25 páginasWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsManuel FierroAinda não há avaliações
- Ajprenal 00351 2005 PDFDocumento8 páginasAjprenal 00351 2005 PDFGauravAinda não há avaliações
- Ajprenal 00351 2005 PDFDocumento8 páginasAjprenal 00351 2005 PDFGauravAinda não há avaliações
- Interaction of Central Angiotensin II and Aldosterone On Sodium Intake and Blood PressureDocumento24 páginasInteraction of Central Angiotensin II and Aldosterone On Sodium Intake and Blood PressureJesus CastroAinda não há avaliações
- (2010) Tubular Reabsortion and Diabetes-Induced Glomerular FiltrationDocumento13 páginas(2010) Tubular Reabsortion and Diabetes-Induced Glomerular FiltrationEnrique MartinezAinda não há avaliações
- ANT 2 S20.fullDocumento13 páginasANT 2 S20.fulllguerreroAinda não há avaliações
- HipertensiuneDocumento9 páginasHipertensiuneCosmin CalanciaAinda não há avaliações
- Vaccine For Hypertension: Modulating The Renin - Angiotensin SystemDocumento9 páginasVaccine For Hypertension: Modulating The Renin - Angiotensin SystemRameshKrishnanAinda não há avaliações
- Ishikane 2018Documento51 páginasIshikane 2018yalocim666Ainda não há avaliações
- Larussa 2017Documento25 páginasLarussa 2017alan.rangel.puenteAinda não há avaliações
- tmpB355 TMPDocumento3 páginastmpB355 TMPFrontiersAinda não há avaliações
- Nitro-Oleic Acid Inhibits Angiotensin II-Induced HypertensionDocumento29 páginasNitro-Oleic Acid Inhibits Angiotensin II-Induced HypertensionKadek SuprajayaAinda não há avaliações
- Assessment and Treatment of Endothelial Dysfunction - 1999Documento10 páginasAssessment and Treatment of Endothelial Dysfunction - 1999Maria TraianAinda não há avaliações
- The Vasoactive Mas Receptor in Essential Hypertension: Clinical MedicineDocumento12 páginasThe Vasoactive Mas Receptor in Essential Hypertension: Clinical MedicineHesbon MomanyiAinda não há avaliações
- Review Article: Animal Models of Hypertension: An OverviewDocumento14 páginasReview Article: Animal Models of Hypertension: An OverviewrodrigodaliascienceAinda não há avaliações
- Effects of Alcohol On Intracellular PH Regulators and Electromechanical Parameters in Human MyocardiumDocumento9 páginasEffects of Alcohol On Intracellular PH Regulators and Electromechanical Parameters in Human MyocardiumAchmad LatiefAinda não há avaliações
- AT1 ReceptorDocumento6 páginasAT1 ReceptorTâm Nguyễn HữuAinda não há avaliações
- Circulation-2002-Cardiovascular Influences of A1b-Adrenergic Receptor Defect in MiceDocumento9 páginasCirculation-2002-Cardiovascular Influences of A1b-Adrenergic Receptor Defect in Miceyylf2016Ainda não há avaliações
- Calcio en La Secrecion de ReninaDocumento12 páginasCalcio en La Secrecion de ReninaJulisa Lipa CristobalAinda não há avaliações
- Angiotensin II Type 2 Receptor Deficiency Aggravates Renal Injury and Reduces Survival in Chronic Kidney Disease in MiceDocumento11 páginasAngiotensin II Type 2 Receptor Deficiency Aggravates Renal Injury and Reduces Survival in Chronic Kidney Disease in MicenovrodAinda não há avaliações
- AT R-At R Cross Talk: Cross Regulation of Angiotensin Ii Type 1 Receptor and The Angiotensin Ii Type 2 ReceptorDocumento5 páginasAT R-At R Cross Talk: Cross Regulation of Angiotensin Ii Type 1 Receptor and The Angiotensin Ii Type 2 ReceptorIrina Luciana DumitriuAinda não há avaliações
- Renal Blood Flow and OxygenationDocumento12 páginasRenal Blood Flow and OxygenationnanreAinda não há avaliações
- Pages 9 20Documento12 páginasPages 9 20Clyde R.OrtegaAinda não há avaliações
- Shishido 2006Documento8 páginasShishido 2006kevin gelaudeAinda não há avaliações
- Renin-Angiotensin System: I: (The Juxtaglomerular Apparatus)Documento1 páginaRenin-Angiotensin System: I: (The Juxtaglomerular Apparatus)reioctabianoAinda não há avaliações
- AT2 Receptor AgonistsDocumento5 páginasAT2 Receptor Agonistsfer123wizAinda não há avaliações
- CC 12031Documento200 páginasCC 12031Arti Tyagita KusumawardhaniAinda não há avaliações
- Angiotensin II, Via AT and AT Receptors and NF-Pathway, Regulates The Inflammatory Response in Unilateral Ureteral ObstructionDocumento16 páginasAngiotensin II, Via AT and AT Receptors and NF-Pathway, Regulates The Inflammatory Response in Unilateral Ureteral Obstructionarmash mominAinda não há avaliações
- Inhibition of Prostaglandin Synthesis During Polystyrenemicrosphere-Induced Pulmonary Embolism in The RatDocumento10 páginasInhibition of Prostaglandin Synthesis During Polystyrenemicrosphere-Induced Pulmonary Embolism in The RatshintaAinda não há avaliações
- Jurnal 33 PDFDocumento16 páginasJurnal 33 PDFshabrina ardeliaAinda não há avaliações
- Urea and Ammonia Metabolism and The Control of Renal Nitrogen ExcretionDocumento15 páginasUrea and Ammonia Metabolism and The Control of Renal Nitrogen ExcretionJames Cojab SacalAinda não há avaliações
- Interactions Between Thromboxane A2, Thromboxane/prostaglandin (TP) Receptors, and Endothelium-Derived HyperpolarizationDocumento9 páginasInteractions Between Thromboxane A2, Thromboxane/prostaglandin (TP) Receptors, and Endothelium-Derived HyperpolarizationMarco Antonio Garcia GonzalezAinda não há avaliações
- Salt Sensitivity of Blood Pressure in NKCC1-deficient MiceDocumento9 páginasSalt Sensitivity of Blood Pressure in NKCC1-deficient MiceHongyu LiAinda não há avaliações
- Protective Effect of 3-N-Butylphthalide Against Hypertensive Nephropathy in Spontaneously Hypertensive RatsDocumento19 páginasProtective Effect of 3-N-Butylphthalide Against Hypertensive Nephropathy in Spontaneously Hypertensive Ratsberliana syifaAinda não há avaliações
- Gastric distension causes peripheral vasoconstriction in anaesthetized pigsDocumento12 páginasGastric distension causes peripheral vasoconstriction in anaesthetized pigsHimanshu SharmaAinda não há avaliações
- 2012 Carnevale D. PI3K in Hypertension A Novel Therapeutic Target Controlling Vascular Myogenic Tone and Target Organ DamageDocumento6 páginas2012 Carnevale D. PI3K in Hypertension A Novel Therapeutic Target Controlling Vascular Myogenic Tone and Target Organ DamageAndi Suchy Qumala SarieAinda não há avaliações
- Renal Reflections: Exploring the Marvels of Nephrology: The Intricate Ballet of Kidney Functions UnveiledNo EverandRenal Reflections: Exploring the Marvels of Nephrology: The Intricate Ballet of Kidney Functions UnveiledAinda não há avaliações
- COX-2 Selectivity Alone Does Not de Ne The Cardiovascularrisks Associated With Non-Steroidal Anti-In Ammatory DrugsDocumento4 páginasCOX-2 Selectivity Alone Does Not de Ne The Cardiovascularrisks Associated With Non-Steroidal Anti-In Ammatory DrugsruleshellzAinda não há avaliações
- Interaction of TNF With Angiotensin II ContributesDocumento12 páginasInteraction of TNF With Angiotensin II ContributesMuôngAinda não há avaliações
- Inside Vitro Examination Along With Biodistribution Research Regarding HAdagrasib Copolymers Individuals Gastrin Issuing Peptide Receptor Inside Prostate Type of CancerqianiDocumento2 páginasInside Vitro Examination Along With Biodistribution Research Regarding HAdagrasib Copolymers Individuals Gastrin Issuing Peptide Receptor Inside Prostate Type of Cancerqianibottledoor0Ainda não há avaliações
- Jurnal DispanDocumento19 páginasJurnal Dispanrahmani kadarningsihAinda não há avaliações
- Devil and Angel in The Renin-Angiotensin System ACE-angiotensin II-AT1 Receptor Axis vs. ACE2-angiotensin - (1-7) - Mas Receptor AxisDocumento4 páginasDevil and Angel in The Renin-Angiotensin System ACE-angiotensin II-AT1 Receptor Axis vs. ACE2-angiotensin - (1-7) - Mas Receptor AxisLevente BalázsAinda não há avaliações
- ScienceDocumento8 páginasScienceDaniela Fantini ValeAinda não há avaliações
- Use of Inotropes and Vasopressor Agents in Critically Ill PatientsDocumento19 páginasUse of Inotropes and Vasopressor Agents in Critically Ill PatientsLong LeAinda não há avaliações
- Pharmaceuticals 03 01286Documento10 páginasPharmaceuticals 03 01286aAinda não há avaliações
- Joe 123Documento19 páginasJoe 123mohammed fayedAinda não há avaliações
- Junral 1999Documento4 páginasJunral 1999Aji Muhammad IqbalAinda não há avaliações
- Toxicology and Applied Pharmacology: Séin O'Connell, Craig Slattery, Michael P. Ryan, Tara McmorrowDocumento10 páginasToxicology and Applied Pharmacology: Séin O'Connell, Craig Slattery, Michael P. Ryan, Tara McmorrowDoyin AwodeleAinda não há avaliações
- Calcium Signaling in Health, Disease and TherapyDocumento9 páginasCalcium Signaling in Health, Disease and TherapyLeonel LedezmaAinda não há avaliações
- Endothelin, Kidney Disease, and HypertensionDocumento5 páginasEndothelin, Kidney Disease, and HypertensionRizki Cah KeratonAinda não há avaliações
- Intermittent Hypoxia-Activated Cyclooxygenase Pathway: Role in AtherosclerosisDocumento10 páginasIntermittent Hypoxia-Activated Cyclooxygenase Pathway: Role in AtherosclerosisaditAinda não há avaliações
- Review Article: The Mechanism of Acupuncture in Treating Essential Hypertension: A Narrative ReviewDocumento10 páginasReview Article: The Mechanism of Acupuncture in Treating Essential Hypertension: A Narrative ReviewpedroAinda não há avaliações
- HR 2008203Documento6 páginasHR 200820322125327Ainda não há avaliações
- Articolo 21Documento32 páginasArticolo 21Francesca BertaccaAinda não há avaliações
- Cross TalkDocumento12 páginasCross TalkWrasasena SuryatmajaAinda não há avaliações
- Queen LongevityDocumento9 páginasQueen Longevityfabiandionisio100% (1)
- Pathomorphology Final ExamDocumento262 páginasPathomorphology Final ExamMann SarwanAinda não há avaliações
- ABO Incompatibility in NewbornsDocumento4 páginasABO Incompatibility in NewbornsNollen LaquianAinda não há avaliações
- Circulatory System Peer Assessment: Examiner's NotesDocumento4 páginasCirculatory System Peer Assessment: Examiner's NotespkrajenpillaygmailcomAinda não há avaliações
- Charnley Ankle ArthrodesisDocumento12 páginasCharnley Ankle Arthrodesisdr_s_ganeshAinda não há avaliações
- IsopreneDocumento5 páginasIsopreneArdynaApriSapoetriAinda não há avaliações
- Psychology: Motivation and EmotionDocumento45 páginasPsychology: Motivation and EmotionAisyah AzmiAinda não há avaliações
- CBSE 2019 Biomolecules Project ReportDocumento15 páginasCBSE 2019 Biomolecules Project ReportRavindra JangidAinda não há avaliações
- Cormie2011 PDFDocumento22 páginasCormie2011 PDFGust AvoAinda não há avaliações
- Apgar ScoreDocumento11 páginasApgar Scorefaizura100% (1)
- Chapter 013Documento4 páginasChapter 013Nusa Koj100% (1)
- Animals Have Basic NeedsDocumento24 páginasAnimals Have Basic NeedsNarendran SubramaniamAinda não há avaliações
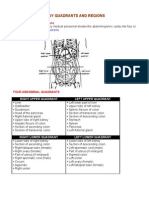
- Organs in The Body Quadrants and RegionsDocumento3 páginasOrgans in The Body Quadrants and RegionsDavid HosamAinda não há avaliações
- Biological Oxidation: Dr. Dalia ShaalanDocumento24 páginasBiological Oxidation: Dr. Dalia ShaalanALIYU AYUBA FUSAMIAinda não há avaliações
- Structures of Amino AcidsDocumento32 páginasStructures of Amino AcidsUsman GhaniAinda não há avaliações
- Broncho DilatorsDocumento53 páginasBroncho DilatorsDocRNAinda não há avaliações
- Aerobic Respiration: Chemiosmosis and Electron Transport ChainDocumento17 páginasAerobic Respiration: Chemiosmosis and Electron Transport ChainAihk kenneth BaronaAinda não há avaliações
- Lab ValuesDocumento3 páginasLab Valuessurviving nursing schoolAinda não há avaliações
- Jeffrey SatinoverDocumento7 páginasJeffrey SatinoverlooiiiiisAinda não há avaliações
- Cranial NervesDocumento118 páginasCranial NervesGan'sAinda não há avaliações
- DR - BD S Step 1 Guide - PDF Filename UTF-8 DR - BD S Step 1 GuideDocumento24 páginasDR - BD S Step 1 Guide - PDF Filename UTF-8 DR - BD S Step 1 GuideAdeelMunawarAinda não há avaliações
- Unit I Clothing Science Two Marks With Answer and Question BankDocumento3 páginasUnit I Clothing Science Two Marks With Answer and Question BankSivakumar KAinda não há avaliações
- Induced Lactation ANR SlidesDocumento11 páginasInduced Lactation ANR Slidesjohn cageAinda não há avaliações
- Infectiile de tract urinar: cazuri cliniceDocumento55 páginasInfectiile de tract urinar: cazuri cliniceMădălina Mihaela LuchianAinda não há avaliações
- LP Surgery ChestDocumento6 páginasLP Surgery Chestangelmd83Ainda não há avaliações
- Revision Sheet Grade 5 For Ut1Documento5 páginasRevision Sheet Grade 5 For Ut1Sudeep BhattacharyaAinda não há avaliações
- Patrick Ch19 p2Documento31 páginasPatrick Ch19 p2NizarAliAinda não há avaliações
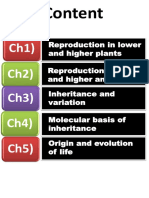
- Biology 12 HSC NotesDocumento195 páginasBiology 12 HSC NotesShitalPatilAinda não há avaliações
- Mash MethodDocumento28 páginasMash MethodShuvajoyyy100% (5)
- g12 Bone Grafts Subs JTG Rev 10 17 10Documento57 páginasg12 Bone Grafts Subs JTG Rev 10 17 10Tudor RalucaAinda não há avaliações