Você também pode gostar
- Braunwald Textbook of Cardiovascular Heart Disease 9th - CHM - 00Documento4 páginasBraunwald Textbook of Cardiovascular Heart Disease 9th - CHM - 00Teguh RahAinda não há avaliações
- 7-PDF 1 Nejmoa1214901Documento6 páginas7-PDF 1 Nejmoa1214901konstantin balabalaAinda não há avaliações
- Sulfamethoxazole Trimethoprim PDFDocumento10 páginasSulfamethoxazole Trimethoprim PDFAsi SyyffaAinda não há avaliações
- Pediatric Primary CareDocumento66 páginasPediatric Primary Carefairwoods100% (1)
- More DetailsDocumento6 páginasMore Detailsdavidmatt18Ainda não há avaliações
- Cript P ('t':'3', 'I':'668332442') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Documento17 páginasCript P ('t':'3', 'I':'668332442') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)rayndijrAinda não há avaliações
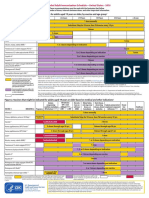
- Figure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupDocumento2 páginasFigure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupmsarasAinda não há avaliações
- Adult ScheduleDocumento3 páginasAdult ScheduledrmanojvimalAinda não há avaliações
- M M Rvaxpro ProspectDocumento57 páginasM M Rvaxpro ProspectNicoleta CiobotarAinda não há avaliações
- Multi Drug Resistant TuberculosisDocumento10 páginasMulti Drug Resistant TuberculosisThuvija DarshiniAinda não há avaliações
- Typhoid FeverDocumento6 páginasTyphoid FeverReeshabhdev GauttamAinda não há avaliações
- Influenza Tetanus, Diphtheria, Pertussis (Td/Tdap) Varicella Human Papillomavirus (HPV) FemaleDocumento5 páginasInfluenza Tetanus, Diphtheria, Pertussis (Td/Tdap) Varicella Human Papillomavirus (HPV) FemaleAneed KasparovAinda não há avaliações
- Tentang PCVDocumento12 páginasTentang PCVJanuwar LukitaAinda não há avaliações
- Istc & DotsDocumento67 páginasIstc & DotsNadilaAinda não há avaliações
- EMA - Pandemrix® (Vaccin A H1N1 - GSK)Documento37 páginasEMA - Pandemrix® (Vaccin A H1N1 - GSK)Tiffany TorresAinda não há avaliações
- Antibiotics 09 00436Documento16 páginasAntibiotics 09 00436Diego Andres Riquelme VeraAinda não há avaliações
- Advances in The Management of Low-Grade GliomasDocumento8 páginasAdvances in The Management of Low-Grade Gliomasgonococo29Ainda não há avaliações
- Journal Article Co TrimoxazoleDocumento2 páginasJournal Article Co TrimoxazoleMansyah HMAinda não há avaliações
- 7-PDF 1 9789241599801 EngDocumento19 páginas7-PDF 1 9789241599801 Engkonstantin balabalaAinda não há avaliações
- s12879 019 4536 8Documento11 páginass12879 019 4536 8mariamaAinda não há avaliações
- Conference Reports Guidelines Paediatric Care Treatment Access IAS 7 Kuala Lumpur 2013Documento8 páginasConference Reports Guidelines Paediatric Care Treatment Access IAS 7 Kuala Lumpur 2013Trie Arni DjunadiAinda não há avaliações
- DKW 076Documento7 páginasDKW 076Irfan AhmadAinda não há avaliações
- Patient Related FactorsDocumento7 páginasPatient Related FactorsandosaputraAinda não há avaliações
- Pharmacy: Cephalosporins: A Focus On Side Chains and - Lactam Cross-ReactivityDocumento16 páginasPharmacy: Cephalosporins: A Focus On Side Chains and - Lactam Cross-ReactivityKenneth DayritAinda não há avaliações
- Antibiotic Resistance Patterns of Urinary Tract Pathogens in Turkish ChildrenDocumento5 páginasAntibiotic Resistance Patterns of Urinary Tract Pathogens in Turkish ChildrenLavfy NjlaaAinda não há avaliações
- Critical Issues Concerning Splenectomy For Chronic Idiopathic Thrombocytopenic Purpura in ChildhoodDocumento3 páginasCritical Issues Concerning Splenectomy For Chronic Idiopathic Thrombocytopenic Purpura in ChildhoodVladimir Henry Triguero RosalesAinda não há avaliações
- H1N1 Clinician Guidance Final Version1Documento2 páginasH1N1 Clinician Guidance Final Version1cha_cruz_6Ainda não há avaliações
- Aspergillosis IDSA Pocketcard Guideline (2016)Documento24 páginasAspergillosis IDSA Pocketcard Guideline (2016)David GerickAinda não há avaliações
- Antibiotik StewardshipDocumento13 páginasAntibiotik StewardshipSeptiandry Ade PutraAinda não há avaliações
- Adult Immunization ScheduleDocumento3 páginasAdult Immunization ScheduleBryan Mae H. DegorioAinda não há avaliações
- 2.5 Implementation Considerations: Eligible Children Aged 6 YearsDocumento45 páginas2.5 Implementation Considerations: Eligible Children Aged 6 YearsSibaraniAinda não há avaliações
- Khvi 10 12 977719Documento6 páginasKhvi 10 12 977719Deby A. IrwantoAinda não há avaliações
- Pneumocistis de Patient UkDocumento6 páginasPneumocistis de Patient UkRaul Gutierrez VerdugoAinda não há avaliações
- Typhoid Fever MedicationDocumento17 páginasTyphoid Fever MedicationPlot BUnnies100% (1)
- 6h MCQDocumento22 páginas6h MCQFull MarksAinda não há avaliações
- Acute Otitis Media: EtiologyDocumento4 páginasAcute Otitis Media: EtiologyMahir FikaAinda não há avaliações
- A Randomised Dose-Ranging Study of Tiotropium Respimat® in Children With Symptomatic Asthma Despite Inhaled CorticosteroidsDocumento10 páginasA Randomised Dose-Ranging Study of Tiotropium Respimat® in Children With Symptomatic Asthma Despite Inhaled CorticosteroidsabdmaliknasAinda não há avaliações
- Di George Syndrome-6 - 1Documento6 páginasDi George Syndrome-6 - 1usamas85556Ainda não há avaliações
- Are Third Generation Cephalosporins Associated With A Bette - 2018 - Clinical MiDocumento6 páginasAre Third Generation Cephalosporins Associated With A Bette - 2018 - Clinical MiRadia LachehebAinda não há avaliações
- CF Guideline 2011 - Jan 4Documento200 páginasCF Guideline 2011 - Jan 4vtAinda não há avaliações
- 394 Full PDFDocumento20 páginas394 Full PDFHaltiAinda não há avaliações
- Funit Copii 6 Luni - 12 AniDocumento5 páginasFunit Copii 6 Luni - 12 AniLyova OrashanAinda não há avaliações
- Istc Report Short VersionDocumento4 páginasIstc Report Short Versiontri_wahyudianto_1Ainda não há avaliações
- Summary END TB Round Table 3 Experience Sharing On DRTB Diagnostics Policies and Whats in The PipelineDocumento10 páginasSummary END TB Round Table 3 Experience Sharing On DRTB Diagnostics Policies and Whats in The Pipelinedk11mapresAinda não há avaliações
- Clinical Reporting For Microbiology Laboratories. Cumulative Antibiotic Susceptibility Reporting.Documento57 páginasClinical Reporting For Microbiology Laboratories. Cumulative Antibiotic Susceptibility Reporting.tanty_ukAinda não há avaliações
- Cephalosporin 3rd Generation IssueDocumento5 páginasCephalosporin 3rd Generation IssuesemaraAinda não há avaliações
- De-Escalacion de ATM en UCI Revisión 2015 y en ShockDocumento15 páginasDe-Escalacion de ATM en UCI Revisión 2015 y en ShockLesly Peinado TorresAinda não há avaliações
- Initiating Antiretroviral Therapy in Treatment-Naive PatientsDocumento33 páginasInitiating Antiretroviral Therapy in Treatment-Naive Patients'Ema Surya PertiwiAinda não há avaliações
- Empirical Treatment of Sepsis in AdultsDocumento11 páginasEmpirical Treatment of Sepsis in AdultsMarnia SulfianaAinda não há avaliações
- Adult Combined ScheduleDocumento5 páginasAdult Combined SchedulelcmurilloAinda não há avaliações
- EBN MalariaDocumento2 páginasEBN Malariahp73092Ainda não há avaliações
- Tmi 12919Documento10 páginasTmi 12919Andi Nur AiynunAinda não há avaliações
- 'Initial Actions Following Exposure': Grade 2CDocumento2 páginas'Initial Actions Following Exposure': Grade 2Cabdulla990Ainda não há avaliações
- Rational Use of AntibioticsDocumento26 páginasRational Use of AntibioticsDr-Jagadeesh MangamooriAinda não há avaliações
- Updated Guideline For The Management of Upper Respiratory Tract Infections in South Africa: 2008Documento9 páginasUpdated Guideline For The Management of Upper Respiratory Tract Infections in South Africa: 2008Arum PelangiAinda não há avaliações
- Caselli 2014Documento5 páginasCaselli 2014AdrianaGallardoTapiaAinda não há avaliações
- Clinical Management Review 2023-2024: Volume 1: USMLE Step 3 and COMLEX-USA Level 3No EverandClinical Management Review 2023-2024: Volume 1: USMLE Step 3 and COMLEX-USA Level 3Nota: 5 de 5 estrelas5/5 (1)
- USMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsNo EverandUSMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsNota: 5 de 5 estrelas5/5 (9)
- Targeted Therapies for Lung CancerNo EverandTargeted Therapies for Lung CancerRavi SalgiaAinda não há avaliações
- Immunogenetics: A Molecular and Clinical Overview: A Molecular Approach to ImmunogeneticsNo EverandImmunogenetics: A Molecular and Clinical Overview: A Molecular Approach to ImmunogeneticsMuneeb U RehmanAinda não há avaliações
- The Efficacy of Intravenous Sodium Valproate and Phenytoin As The First-Line Treatment in Status Epilepticus: A Comparison StudyDocumento5 páginasThe Efficacy of Intravenous Sodium Valproate and Phenytoin As The First-Line Treatment in Status Epilepticus: A Comparison Studykonstantin balabalaAinda não há avaliações
- Delirium Presentation WebDocumento26 páginasDelirium Presentation Webkonstantin balabalaAinda não há avaliações
- Who NMH NPH 01.3Documento24 páginasWho NMH NPH 01.3konstantin balabalaAinda não há avaliações
- 6.7 Use of Pis in Initial Therapy: Table 10: Summary of Preferred First-Line Arv Regimens For Infants and ChildrenDocumento20 páginas6.7 Use of Pis in Initial Therapy: Table 10: Summary of Preferred First-Line Arv Regimens For Infants and Childrenkonstantin balabalaAinda não há avaliações
- 7-PDF 1 Nejmoa1214901Documento2 páginas7-PDF 1 Nejmoa1214901konstantin balabalaAinda não há avaliações
- When To Start Antiretroviral Therapy in Infants and ChildrenDocumento25 páginasWhen To Start Antiretroviral Therapy in Infants and Childrenkonstantin balabalaAinda não há avaliações
- 7-PDF 1 9789241599801 EngDocumento19 páginas7-PDF 1 9789241599801 Engkonstantin balabalaAinda não há avaliações
- Hyper Tiro IdDocumento5 páginasHyper Tiro Idkonstantin balabalaAinda não há avaliações
- 10 SirliDocumento11 páginas10 Sirlikonstantin balabalaAinda não há avaliações
- Variabel Kategorikal: Npar Tests - Tes BinomialDocumento4 páginasVariabel Kategorikal: Npar Tests - Tes Binomialkonstantin balabalaAinda não há avaliações
- Pathways VertigoDocumento1 páginaPathways Vertigokonstantin balabala0% (1)
- Formularium Farmasi Cendana 2020Documento42 páginasFormularium Farmasi Cendana 2020Vidyanti Permata DewiAinda não há avaliações
- Thyroid in PregnancyDocumento40 páginasThyroid in PregnancyGPFanAinda não há avaliações
- Health Declaration FormDocumento2 páginasHealth Declaration Formcreativeraj_181283100% (1)
- Analgetik Non Opioid NsaidDocumento3 páginasAnalgetik Non Opioid NsaidShintaAinda não há avaliações
- Flash Notes Billie-GeneticsDocumento29 páginasFlash Notes Billie-GeneticsschxzerrydawnAinda não há avaliações
- Daftar Antibiotik TerbaruDocumento4 páginasDaftar Antibiotik TerbaruAnonymous WmCaefjAinda não há avaliações
- LibroEnfermedadPeriodontalPag102201 PDFDocumento50 páginasLibroEnfermedadPeriodontalPag102201 PDFLorena RiveraAinda não há avaliações
- PANCE or PANRE PA Exam What Do Zebras Have To Do With My SuccessDocumento2 páginasPANCE or PANRE PA Exam What Do Zebras Have To Do With My SuccessHELP PANCE PANRE Online PA Exam Review CourseAinda não há avaliações
- BASIC DefectaDocumento7 páginasBASIC Defectaafifah klinikAinda não há avaliações
- Pure Antibiotic PowderDocumento2 páginasPure Antibiotic PowderTitan BiotechAinda não há avaliações
- KROK2 2008 Paper (200 QS)Documento61 páginasKROK2 2008 Paper (200 QS)Ali ZeeshanAinda não há avaliações
- Daftar Harga Obat Pt. Molex Ayus (Per Maret 2019) PDFDocumento4 páginasDaftar Harga Obat Pt. Molex Ayus (Per Maret 2019) PDFfirmianisaAinda não há avaliações
- Drug Study: Name of Drug Action Indication Adverse Effect Nursing ResponsibilityDocumento4 páginasDrug Study: Name of Drug Action Indication Adverse Effect Nursing ResponsibilityBel CortezAinda não há avaliações
- Peace Corps MTG 300 ImmunizationDocumento199 páginasPeace Corps MTG 300 ImmunizationAccessible Journal Media: Peace Corps DocumentsAinda não há avaliações
- DM Tipe II, Dsme Ginc 2017Documento10 páginasDM Tipe II, Dsme Ginc 2017Ahmad RifaiAinda não há avaliações
- SANOV18 DikonversiDocumento93 páginasSANOV18 DikonversiIc-tika Siee ChuabbieAinda não há avaliações
- High Yield Psychiatry: Shelf Exam Review Emma Holliday RamahiDocumento43 páginasHigh Yield Psychiatry: Shelf Exam Review Emma Holliday Ramahigreg100% (1)
- Med TemplateDocumento1 páginaMed TemplateAnbar100% (1)
- Reten HMIS OGOS 09 PkdjerantutDocumento11 páginasReten HMIS OGOS 09 Pkdjerantutzatie2009Ainda não há avaliações
- UtiDocumento34 páginasUtinimas putriAinda não há avaliações
- DHIS Secondary Health Facility Monthly Report FormDocumento4 páginasDHIS Secondary Health Facility Monthly Report FormBd Db0% (1)
- Difference Between GERD and PUDDocumento7 páginasDifference Between GERD and PUDOla Adel ShabeebAinda não há avaliações
- MumpsDocumento16 páginasMumpsRahul DhakerAinda não há avaliações
- INDICATIIDocumento17 páginasINDICATIITarek TarekAinda não há avaliações
- Label PatenDocumento15 páginasLabel PatenulfiaturohmahAinda não há avaliações
- KlinikDocumento165 páginasKlinikDwi Eka Suci WulandariAinda não há avaliações
- Drug Study: Patient: B.V Age: 58y/oDocumento2 páginasDrug Study: Patient: B.V Age: 58y/oAndrea Sibayan SorianoAinda não há avaliações
- Early Signs of AlzheimerDocumento4 páginasEarly Signs of Alzheimermoose73Ainda não há avaliações
- MEDICAMENTEDocumento13 páginasMEDICAMENTELily Ozunu100% (1)
- Pedia NotesDocumento3 páginasPedia NotesNikki DiocampoAinda não há avaliações