Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Antihipertension Drugs Revise 2010Documento71 páginasAntihipertension Drugs Revise 2010YeniAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Rational Drug Treatment2011Documento27 páginasRational Drug Treatment2011YeniAinda não há avaliações
- 2007 Guidelines For The Management of Arterial European Heart AssossDocumento75 páginas2007 Guidelines For The Management of Arterial European Heart AssossYeniAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- 2010 CHEP - RecommendationsDocumento5 páginas2010 CHEP - RecommendationsArdhito BudhijuwonoAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- History TakingDocumento28 páginasHistory TakingYeniAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Overview of Hypertension 2009Documento50 páginasThe Overview of Hypertension 2009YeniAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Physical Examination of Cardiovascular: DR - Ira Andaningsih SPJP Cardiovascular Block 2008Documento89 páginasPhysical Examination of Cardiovascular: DR - Ira Andaningsih SPJP Cardiovascular Block 2008YeniAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Film Session Grey's AnatomyDocumento4 páginasFilm Session Grey's AnatomyYeniAinda não há avaliações
- Erythropoiesis and Bilirubin Metabolism: V. Sutarmo SetiadjiDocumento16 páginasErythropoiesis and Bilirubin Metabolism: V. Sutarmo SetiadjiYeniAinda não há avaliações
- Metabolisme B-12 and FolateDocumento9 páginasMetabolisme B-12 and FolateYeniAinda não há avaliações
- Print-Slide DR DinaDocumento4 páginasPrint-Slide DR DinaYeniAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Print-Slide DR DinaDocumento4 páginasPrint-Slide DR DinaYeniAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Anemia UPHDocumento24 páginasAnemia UPHYeniAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Appropriate Use of Tests For Folate and Vitamin B12 DeficiencyDocumento4 páginasAppropriate Use of Tests For Folate and Vitamin B12 DeficiencyYeniAinda não há avaliações
- Anemia, Rhesus and Blood Group Incompatibility inDocumento42 páginasAnemia, Rhesus and Blood Group Incompatibility inYeniAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Dr. Haryanto - Kuliah Approach Anemia 2011Documento23 páginasDr. Haryanto - Kuliah Approach Anemia 2011YeniAinda não há avaliações
- Anemia ClinskillDocumento15 páginasAnemia ClinskillYeniAinda não há avaliações
- Anemia FarmakoDocumento28 páginasAnemia FarmakoYeniAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Erythrocyte Life Cycle: PathophysiologyDocumento15 páginasErythrocyte Life Cycle: PathophysiologyYeniAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Dr. Haryanto - Kuliah Anemi Deff Fe 2011Documento20 páginasDr. Haryanto - Kuliah Anemi Deff Fe 2011YeniAinda não há avaliações
- Syncope VonnyDocumento41 páginasSyncope VonnyYeniAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Syncope VonnyDocumento41 páginasSyncope VonnyYeniAinda não há avaliações
- Head InjuryDocumento40 páginasHead InjuryYeniAinda não há avaliações
- Tabel AntibiotikDocumento5 páginasTabel AntibiotikYeniAinda não há avaliações
- Anti VirusDocumento36 páginasAnti VirusYeniAinda não há avaliações
- Plenary Lecture Multiple Trauma by FredaDocumento19 páginasPlenary Lecture Multiple Trauma by FredaYeniAinda não há avaliações
- Nosocomial Infection UphDocumento77 páginasNosocomial Infection UphYeniAinda não há avaliações
- Nosocomial Infection UphDocumento77 páginasNosocomial Infection UphYeniAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Week 4 - Fungi Effector Mechanism of IRDocumento67 páginasWeek 4 - Fungi Effector Mechanism of IRYeniAinda não há avaliações
- TraceGains Inspection Day FDA Audit ChecklistDocumento2 páginasTraceGains Inspection Day FDA Audit Checklistdrs_mdu48Ainda não há avaliações
- "Next Friend" and "Guardian Ad Litem" - Difference BetweenDocumento1 página"Next Friend" and "Guardian Ad Litem" - Difference BetweenTeh Hong Xhe100% (2)
- Iomm VFD-3 030112Documento100 páginasIomm VFD-3 030112Alexander100% (1)
- Soil SSCDocumento11 páginasSoil SSCvkjha623477Ainda não há avaliações
- Anti Stain Nsl30 Super - Msds - SdsDocumento8 páginasAnti Stain Nsl30 Super - Msds - SdsS.A. MohsinAinda não há avaliações
- Yogananda Scientific HealingDocumento47 páginasYogananda Scientific HealingSagar Pandya100% (4)
- Art of Facing InterviewsDocumento15 páginasArt of Facing Interviewskrish_cvr2937100% (2)
- Business Plan Example - Little LearnerDocumento26 páginasBusiness Plan Example - Little LearnerCourtney mcintosh100% (1)
- OPSS1213 Mar98Documento3 páginasOPSS1213 Mar98Tony ParkAinda não há avaliações
- 2005 Harley Davidson Sportster 883 66418Documento136 páginas2005 Harley Davidson Sportster 883 66418Josef Bruno SchlittenbauerAinda não há avaliações
- EIL Document On Motor, PanelDocumento62 páginasEIL Document On Motor, PanelArindam Samanta100% (1)
- Funding HR2 Coalition LetterDocumento3 páginasFunding HR2 Coalition LetterFox NewsAinda não há avaliações
- ISO 45001:2018 & OHSAS 18001:2007 Clause-Wise Comparison MatrixDocumento3 páginasISO 45001:2018 & OHSAS 18001:2007 Clause-Wise Comparison MatrixvenkatesanAinda não há avaliações
- Dr. Sajjad Hussain Sumrra Isomerism (CHEM-305) Inorganic Chemistry-IIDocumento48 páginasDr. Sajjad Hussain Sumrra Isomerism (CHEM-305) Inorganic Chemistry-IITanya DilshadAinda não há avaliações
- Far Eastern University - Manila Income Taxation TAX1101 Fringe Benefit TaxDocumento10 páginasFar Eastern University - Manila Income Taxation TAX1101 Fringe Benefit TaxRyan Christian BalanquitAinda não há avaliações
- Acute Renal Failure in The Intensive Care Unit: Steven D. Weisbord, M.D., M.Sc. and Paul M. Palevsky, M.DDocumento12 páginasAcute Renal Failure in The Intensive Care Unit: Steven D. Weisbord, M.D., M.Sc. and Paul M. Palevsky, M.Dkerm6991Ainda não há avaliações
- Global Talent MonitorDocumento30 páginasGlobal Talent Monitornitinsoni807359Ainda não há avaliações
- NRF Nano EthicsDocumento18 páginasNRF Nano Ethicsfelipe de jesus juarez torresAinda não há avaliações
- CBEU Service ConditionsDocumento623 páginasCBEU Service ConditionsAtul ModiAinda não há avaliações
- NORSOK M-630 Edition 6 Draft For HearingDocumento146 páginasNORSOK M-630 Edition 6 Draft For Hearingcaod1712100% (1)
- Nitric AcidDocumento7 páginasNitric AcidKuldeep BhattAinda não há avaliações
- Cadorna, Chesca L. - NCPDocumento2 páginasCadorna, Chesca L. - NCPCadorna Chesca LoboAinda não há avaliações
- Itrogen: by Deborah A. KramerDocumento18 páginasItrogen: by Deborah A. KramernycAinda não há avaliações
- Food Processing NC II - SAGDocumento4 páginasFood Processing NC II - SAGNylmazdahr Sañeud DammahomAinda não há avaliações
- ArticleDocumento5 páginasArticleJordi Sumoy PifarréAinda não há avaliações
- Laboratory Cold ChainDocumento22 páginasLaboratory Cold ChainEmiAinda não há avaliações
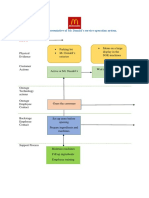
- Blueprint Huynh My Ky Duyen 2022 McDonald'sDocumento2 páginasBlueprint Huynh My Ky Duyen 2022 McDonald'sHuỳnh Mỹ Kỳ DuyênAinda não há avaliações
- DyslexiaDocumento19 páginasDyslexiaKeren HapkhAinda não há avaliações
- SanMilan Inigo Cycling Physiology and Physiological TestingDocumento67 páginasSanMilan Inigo Cycling Physiology and Physiological Testingjesus.clemente.90Ainda não há avaliações
- Join Our Telegram Channel: @AJITLULLA: To Get Daily Question Papers & SolutionsDocumento24 páginasJoin Our Telegram Channel: @AJITLULLA: To Get Daily Question Papers & SolutionsNaveen KumarAinda não há avaliações
- Glucose Revolution: The Life-Changing Power of Balancing Your Blood SugarNo EverandGlucose Revolution: The Life-Changing Power of Balancing Your Blood SugarNota: 5 de 5 estrelas5/5 (351)
- Forever Strong: A New, Science-Based Strategy for Aging WellNo EverandForever Strong: A New, Science-Based Strategy for Aging WellAinda não há avaliações
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyNo EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyNota: 4.5 de 5 estrelas4.5/5 (3)
- Eat & Run: My Unlikely Journey to Ultramarathon GreatnessNo EverandEat & Run: My Unlikely Journey to Ultramarathon GreatnessAinda não há avaliações
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonNo EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonNota: 3.5 de 5 estrelas3.5/5 (33)
- Summary of Mary Claire Haver's The Galveston DietNo EverandSummary of Mary Claire Haver's The Galveston DietNota: 5 de 5 estrelas5/5 (1)
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookNo EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookNota: 3.5 de 5 estrelas3.5/5 (2)
- Grit & Grace: Train the Mind, Train the Body, Own Your LifeNo EverandGrit & Grace: Train the Mind, Train the Body, Own Your LifeNota: 4 de 5 estrelas4/5 (3)