Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1091)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- G6PD Brochure 2017Documento3 páginasG6PD Brochure 2017Je Ann Catherine FeliasAinda não há avaliações
- Immunology of Transplant RejectionDocumento8 páginasImmunology of Transplant Rejectionxplaind100% (1)
- The Effectiveness of Cognitive Behavioral Therapy (CBT) On Generalized Anxiety Disorder (GAD)Documento8 páginasThe Effectiveness of Cognitive Behavioral Therapy (CBT) On Generalized Anxiety Disorder (GAD)nadia rukmanaAinda não há avaliações
- Metabical Case Solution Havard Business School ReviewDocumento3 páginasMetabical Case Solution Havard Business School ReviewparoengineerAinda não há avaliações
- Coding Poli Mata: Papillitis H46 Hypertension Ocular:h40.0 Macula H35.8 Ptosis H02.4 Chalazion H00.1 Asthenopia H53.1Documento1 páginaCoding Poli Mata: Papillitis H46 Hypertension Ocular:h40.0 Macula H35.8 Ptosis H02.4 Chalazion H00.1 Asthenopia H53.1nurcasanAinda não há avaliações
- cl-DUTIES AND RESPONSIBILITIES OF LAB PERSONNELSDocumento2 páginascl-DUTIES AND RESPONSIBILITIES OF LAB PERSONNELSRazel Ann Elagio100% (2)
- Chapter 14 - Fluid and Electrolytes - Balance and DisturbanceDocumento20 páginasChapter 14 - Fluid and Electrolytes - Balance and DisturbanceEmily Cormier100% (1)
- To Compare Rosuvastatin With Atorvastatin in Terms of Mean Change in LDL C in Patient With Diabetes PDFDocumento7 páginasTo Compare Rosuvastatin With Atorvastatin in Terms of Mean Change in LDL C in Patient With Diabetes PDFJez RarangAinda não há avaliações
- Upper Extremity Reconstruction: Surgical SolutionsDocumento16 páginasUpper Extremity Reconstruction: Surgical Solutionsapi-488115640Ainda não há avaliações
- Perawatan Pasien Dengan Gips Cast Skill LabDocumento36 páginasPerawatan Pasien Dengan Gips Cast Skill LabFadhilah putri fertyciaAinda não há avaliações
- Aldrich Cover Letter FinalDocumento1 páginaAldrich Cover Letter Finalapi-532847344Ainda não há avaliações
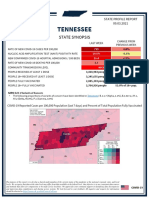
- Tennessee State Profile Report 20210903 PublicDocumento17 páginasTennessee State Profile Report 20210903 PublicAnonymous GF8PPILW5Ainda não há avaliações
- Cilacar CME Final 23-8-2010Documento91 páginasCilacar CME Final 23-8-2010Kanchan Pathak100% (1)
- Marijuana: Aron H. Lichtman Professor Department of Pharmacology and ToxicologyDocumento67 páginasMarijuana: Aron H. Lichtman Professor Department of Pharmacology and Toxicologyunknown racerx50Ainda não há avaliações
- AlexithymiaDocumento10 páginasAlexithymiaCassiopea AndromedaAinda não há avaliações
- Clinical Documentation Improvement For Physician E/M CodingDocumento5 páginasClinical Documentation Improvement For Physician E/M CodingAudioEducatorAinda não há avaliações
- PPH Simulation PowerpointDocumento1 páginaPPH Simulation Powerpointapi-353926961Ainda não há avaliações
- Journal Recent Advances in Management of Maxillofacial TraumaDocumento9 páginasJournal Recent Advances in Management of Maxillofacial TraumaPrazna ShafiraAinda não há avaliações
- 1 PBDocumento11 páginas1 PBNaswa Alifia PutriAinda não há avaliações
- Joanna 11Documento42 páginasJoanna 11Joanne GuzmanAinda não há avaliações
- SBLE English SimpleDocumento8 páginasSBLE English SimpleKian GonzagaAinda não há avaliações
- Presentasi Virus Corona Bahasa InggrisDocumento7 páginasPresentasi Virus Corona Bahasa Inggrisjasmin andraina100% (1)
- Data Change Template CardivaDocumento123 páginasData Change Template CardivaNorilyn FloresAinda não há avaliações
- Company Profile Indo Medika InternationalDocumento12 páginasCompany Profile Indo Medika InternationalshavinravizaAinda não há avaliações
- Patient Rights & Responsibilities 03 Aug 2011Documento1 páginaPatient Rights & Responsibilities 03 Aug 2011Jv SinghAinda não há avaliações
- Romano Et Al-2024-Cochrane Database of Systematic ReviewsDocumento111 páginasRomano Et Al-2024-Cochrane Database of Systematic Reviewsaraujoaoh07Ainda não há avaliações
- Hypersensitivity 2Documento3 páginasHypersensitivity 2kuldip.biotechAinda não há avaliações
- Retrospective Study - The Presence of Malassezia in Feline Skin Biopsies. A Clinicopathological Study (Pages 7-14)Documento8 páginasRetrospective Study - The Presence of Malassezia in Feline Skin Biopsies. A Clinicopathological Study (Pages 7-14)jenAinda não há avaliações
- Antihistamine in Pediatrics AllergyDocumento10 páginasAntihistamine in Pediatrics AllergyIndra AdjuddinAinda não há avaliações
- GCC Guidelines For Ectd SubmissionDocumento18 páginasGCC Guidelines For Ectd SubmissionSatadal Deb RoyAinda não há avaliações