Você também pode gostar
- Exercise For The Brain: 70 Neurobic Exercises To Increase Mental Fitness & Prevent Memory Loss (With Crossword Puzzles)No EverandExercise For The Brain: 70 Neurobic Exercises To Increase Mental Fitness & Prevent Memory Loss (With Crossword Puzzles)Ainda não há avaliações
- Exercise For The Brain: 70 Neurobic Exercises To Increase Mental Fitness & Prevent Memory Loss: How Non Routine Actions And Thoughts Improve Mental HealthNo EverandExercise For The Brain: 70 Neurobic Exercises To Increase Mental Fitness & Prevent Memory Loss: How Non Routine Actions And Thoughts Improve Mental HealthAinda não há avaliações
- Exercises for the Brain and Memory : 70 Neurobic Exercises & FUN Puzzles to Increase Mental Fitness & Boost Your Brain Juice Today (With Crossword Puzzles)No EverandExercises for the Brain and Memory : 70 Neurobic Exercises & FUN Puzzles to Increase Mental Fitness & Boost Your Brain Juice Today (With Crossword Puzzles)Nota: 4 de 5 estrelas4/5 (8)
- Anti Aging Secret of the Animals: Learn the Simple Somatic Movements That Can Cure Back Pain, Restore Your Flexibility and Rejuvenate Your Body to Its Natural, Youthful State Today!No EverandAnti Aging Secret of the Animals: Learn the Simple Somatic Movements That Can Cure Back Pain, Restore Your Flexibility and Rejuvenate Your Body to Its Natural, Youthful State Today!Nota: 5 de 5 estrelas5/5 (1)
- Exercises for the Brain and Memory : 70 Neurobic Exercises & FUN Puzzles to Increase Mental Fitness & Boost Your Brain Juice Today: (Special 2 In 1 Exclusive Edition)No EverandExercises for the Brain and Memory : 70 Neurobic Exercises & FUN Puzzles to Increase Mental Fitness & Boost Your Brain Juice Today: (Special 2 In 1 Exclusive Edition)Nota: 4 de 5 estrelas4/5 (1)
- Neurohacking For Online Learning: Study and Life Habits Optimized for Your Personal Mind-Body Energy StateNo EverandNeurohacking For Online Learning: Study and Life Habits Optimized for Your Personal Mind-Body Energy StateAinda não há avaliações
- Move Right. Live Right.: What the mind believes capable, becomes capable: Strategies to move towards a better youNo EverandMove Right. Live Right.: What the mind believes capable, becomes capable: Strategies to move towards a better youAinda não há avaliações
- Brain Health: How to Nurture and Nourish Your Brain for Top Performance!No EverandBrain Health: How to Nurture and Nourish Your Brain for Top Performance!Ainda não há avaliações
- Stretching: The Top 100 Best Stretches Of All Time: Increase Flexibility, Gain Strength, Relieve Pain & Prevent InjuryNo EverandStretching: The Top 100 Best Stretches Of All Time: Increase Flexibility, Gain Strength, Relieve Pain & Prevent InjuryAinda não há avaliações
- Neuro-Habits: Rewire Your Brain to Stop Self-Defeating Behaviors and Make the Right Choice Every TimeNo EverandNeuro-Habits: Rewire Your Brain to Stop Self-Defeating Behaviors and Make the Right Choice Every TimeNota: 4.5 de 5 estrelas4.5/5 (3)
- REWIRE YOUR BRAIN: Harnessing Neuroplasticity for Personal Transformation (2023 Beginner Guide)No EverandREWIRE YOUR BRAIN: Harnessing Neuroplasticity for Personal Transformation (2023 Beginner Guide)Ainda não há avaliações
- Super Body, Super Brain: The Workout That Does It AllNo EverandSuper Body, Super Brain: The Workout That Does It AllNota: 3.5 de 5 estrelas3.5/5 (5)
- Better Stretching: 9 Minutes a Day to Greater Flexibility, Less Pain, and Enhanced Performance, the JoeTherapy WayNo EverandBetter Stretching: 9 Minutes a Day to Greater Flexibility, Less Pain, and Enhanced Performance, the JoeTherapy WayNota: 4 de 5 estrelas4/5 (5)
- How To Learn (Qualitatively and Quantitatively) : The BrainDocumento5 páginasHow To Learn (Qualitatively and Quantitatively) : The Brainashutosh choudharyAinda não há avaliações
- Brain Training: 23 Ultimate Brain Training Tips for Mental Focus and Concentration TrainingNo EverandBrain Training: 23 Ultimate Brain Training Tips for Mental Focus and Concentration TrainingNota: 4.5 de 5 estrelas4.5/5 (3)
- Jack Heggie - The Use of The Eyes in Movement (Feldenkrais) (1985)Documento62 páginasJack Heggie - The Use of The Eyes in Movement (Feldenkrais) (1985)Joaquín González100% (1)
- Boost Your Brain Health - A Practical Guide To Keep Your Brain Sharp And Improve Memory Power As You AgeNo EverandBoost Your Brain Health - A Practical Guide To Keep Your Brain Sharp And Improve Memory Power As You AgeNota: 3.5 de 5 estrelas3.5/5 (9)
- The Anti-Anxiety Toolkit: Rapid Techniques to Rewire the BrainNo EverandThe Anti-Anxiety Toolkit: Rapid Techniques to Rewire the BrainNota: 4.5 de 5 estrelas4.5/5 (6)
- Personal Transformation Mastery: In Personal Transformation Mastery, you’ll discover that you really do have untapped potential just waiting to be unleashed.No EverandPersonal Transformation Mastery: In Personal Transformation Mastery, you’ll discover that you really do have untapped potential just waiting to be unleashed.Ainda não há avaliações
- The FIT Chronicles: A Collection of fitness articles covering all aspects of exercise and its componentsNo EverandThe FIT Chronicles: A Collection of fitness articles covering all aspects of exercise and its componentsNota: 5 de 5 estrelas5/5 (1)
- Английский эссе 6Documento2 páginasАнглийский эссе 6Екатерина БалакайAinda não há avaliações
- MELT Performance: A Step by-Step Program to Accelerate Your Fitness Goals, Improve Balance and Control, and Prevent Chronic Pain and Injuries for LifeNo EverandMELT Performance: A Step by-Step Program to Accelerate Your Fitness Goals, Improve Balance and Control, and Prevent Chronic Pain and Injuries for LifeAinda não há avaliações
- (English) After Watching This, Your Brain Will Not Be The Same - Lara Boyd - TEDxVancouver (DownSub - Com)Documento12 páginas(English) After Watching This, Your Brain Will Not Be The Same - Lara Boyd - TEDxVancouver (DownSub - Com)Maulana Yazid Al AnnuriAinda não há avaliações
- Brain Training: The Ultimate Guide to Increase Your Brain Power and Improving Your Memory (Brain Exercise, Concentration, Neuroplasticity, Mental Clarity, Brain Plasticity)No EverandBrain Training: The Ultimate Guide to Increase Your Brain Power and Improving Your Memory (Brain Exercise, Concentration, Neuroplasticity, Mental Clarity, Brain Plasticity)Ainda não há avaliações
- Bonus 1 Exercise SleepDocumento7 páginasBonus 1 Exercise SleeprafaschettiniAinda não há avaliações
- Memory Improvement, Accelerated Learning and Brain Training: Learn How to Optimize and Improve Your Memory and Learning Capabilities for Top Results in University and at WorkNo EverandMemory Improvement, Accelerated Learning and Brain Training: Learn How to Optimize and Improve Your Memory and Learning Capabilities for Top Results in University and at WorkAinda não há avaliações
- The Muscular System Part 1Documento30 páginasThe Muscular System Part 1ISTORYAAinda não há avaliações
- Mindful Manifestation Meditation: How to Use the Power of Your Mind to Manifest the Life You ImagineNo EverandMindful Manifestation Meditation: How to Use the Power of Your Mind to Manifest the Life You ImagineAinda não há avaliações
- Fitness and Exercise Fun for Baby Boomers and SeniorsNo EverandFitness and Exercise Fun for Baby Boomers and SeniorsAinda não há avaliações
- Rena - Yuliana-UNIT 7 CONCENTRATION (3) - ILDocumento4 páginasRena - Yuliana-UNIT 7 CONCENTRATION (3) - ILEkhaAinda não há avaliações
- K.A.T.T - Day 8 - MOVEMENT & PHYSIOLOGYDocumento1 páginaK.A.T.T - Day 8 - MOVEMENT & PHYSIOLOGYAnurag WareAinda não há avaliações
- Freeweight Training Anatomy: An Illustrated Guide to the Muscles Used while Exercising with Dumbbells, Barbells, and Kettlebells and moreNo EverandFreeweight Training Anatomy: An Illustrated Guide to the Muscles Used while Exercising with Dumbbells, Barbells, and Kettlebells and moreAinda não há avaliações
- Maximising Your Intellectual Abilities: Learn how to make the most of your intelligenceNo EverandMaximising Your Intellectual Abilities: Learn how to make the most of your intelligenceAinda não há avaliações
- Anat Baniel Mal Di schiena-GBDocumento9 páginasAnat Baniel Mal Di schiena-GBVittorioAinda não há avaliações
- Defying the Pains of Gravity: Using Proper Posture TechniqueNo EverandDefying the Pains of Gravity: Using Proper Posture TechniqueAinda não há avaliações
- JACK HEGGIE OJOS - The Use of The Eyes in Movement (1985)Documento58 páginasJACK HEGGIE OJOS - The Use of The Eyes in Movement (1985)Adriana M. VillalónAinda não há avaliações
- Concentration: Maintain Laser Sharp Focus & Attention for 5 Hours or More: Mind Hack, #3No EverandConcentration: Maintain Laser Sharp Focus & Attention for 5 Hours or More: Mind Hack, #3Ainda não há avaliações
- The Power Of Habit - Transforming Your Life One Step At A TimeNo EverandThe Power Of Habit - Transforming Your Life One Step At A TimeAinda não há avaliações
- Brain Training: Exercise Your Mind and Improve Your Memory (Mental Clarity Neuroplasticity and to Boost Overall Mind Power)No EverandBrain Training: Exercise Your Mind and Improve Your Memory (Mental Clarity Neuroplasticity and to Boost Overall Mind Power)Ainda não há avaliações
- Jack Heggie - Use of The Eyes in Movement (1985) PDFDocumento62 páginasJack Heggie - Use of The Eyes in Movement (1985) PDFNeoFu26100% (1)
- Reflection in SystemsDocumento1 páginaReflection in SystemsGeraldine PadillaAinda não há avaliações
- Trigger Point System 2Documento6 páginasTrigger Point System 2Jaime GutzmanAinda não há avaliações
- Nano Workouts: Get in Shape and Lose Weight During Everyday ActivitiesNo EverandNano Workouts: Get in Shape and Lose Weight During Everyday ActivitiesAinda não há avaliações
- Premature Ejaculation: The Complete Guide to Better Sex, and Controlling PE - Learn How to Last Longer in Bed and Get Complete Control Over Your EjaculationNo EverandPremature Ejaculation: The Complete Guide to Better Sex, and Controlling PE - Learn How to Last Longer in Bed and Get Complete Control Over Your EjaculationNota: 5 de 5 estrelas5/5 (1)
- Student Wellbeing Handbook: How to Thrive and Be Your Best SelfNo EverandStudent Wellbeing Handbook: How to Thrive and Be Your Best SelfAinda não há avaliações
- Stewart J - ResumeDocumento2 páginasStewart J - Resumeapi-232971337Ainda não há avaliações
- Stewart James - Leadership PlanDocumento8 páginasStewart James - Leadership Planapi-232971337Ainda não há avaliações
- Crone Stewart Systematic Review-FinalDocumento20 páginasCrone Stewart Systematic Review-Finalapi-232971337Ainda não há avaliações
- Stewart J - Occupational Profile AnalysisDocumento12 páginasStewart J - Occupational Profile Analysisapi-232971337100% (2)
- Immigration PresentationDocumento34 páginasImmigration Presentationapi-232971337Ainda não há avaliações
- Eval 36833338Documento5 páginasEval 36833338api-232971337Ainda não há avaliações
- Eval 40795427Documento5 páginasEval 40795427api-232971337Ainda não há avaliações
- Eval 38446785Documento4 páginasEval 38446785api-232971337Ainda não há avaliações
- l2 Rancho High SchoolDocumento1 páginal2 Rancho High Schoolapi-232971337Ainda não há avaliações
- Stewart J - Assistive Technology PaperDocumento12 páginasStewart J - Assistive Technology Paperapi-232971337Ainda não há avaliações
- Assignment Professional Development PlanDocumento3 páginasAssignment Professional Development Planapi-232971337Ainda não há avaliações
- Occupational Profile-AdultsDocumento11 páginasOccupational Profile-Adultsapi-232971337Ainda não há avaliações
- Child-Based Group Case StudyDocumento19 páginasChild-Based Group Case Studyapi-232971337Ainda não há avaliações
- Child-Based Research ReviewDocumento9 páginasChild-Based Research Reviewapi-232971337Ainda não há avaliações
- Occupational Analysis PaperDocumento18 páginasOccupational Analysis Paperapi-232971337Ainda não há avaliações
- Crone Loja Mourselas Pierson Stewart QualresrptDocumento34 páginasCrone Loja Mourselas Pierson Stewart Qualresrptapi-233645719Ainda não há avaliações
- Quantitative PaperDocumento9 páginasQuantitative Paperapi-232971337Ainda não há avaliações
- CBR Estimate ComparisonDocumento1 páginaCBR Estimate ComparisonNinan Koshy VaidyanAinda não há avaliações
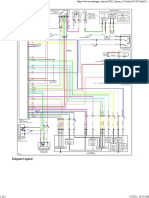
- 2012 Mitsubishi LANCER CVT WiringDocumento1 página2012 Mitsubishi LANCER CVT WiringMohamed MoustafaAinda não há avaliações
- Directory: 2010 Annual Guide OutfittersDocumento10 páginasDirectory: 2010 Annual Guide OutfittersKelly WrightAinda não há avaliações
- dl24m ManualDocumento47 páginasdl24m Manualperalta78Ainda não há avaliações
- Noble Graham - Mas Oyama in AmericaDocumento23 páginasNoble Graham - Mas Oyama in AmericaClin Eastwood100% (5)
- Blood DopingDocumento7 páginasBlood DopingRizza Mae Salvania100% (1)
- Contoh Article Issue ReportDocumento12 páginasContoh Article Issue ReportMohd AlzairuddinAinda não há avaliações
- The Complete Book of Reading, Grades 5-6 (PDFDrive) - Pages-1-2,4-7,56-147Documento98 páginasThe Complete Book of Reading, Grades 5-6 (PDFDrive) - Pages-1-2,4-7,56-147アイジーAijiAinda não há avaliações
- Daftar Harga KueDocumento2 páginasDaftar Harga KueElsa RosalinaAinda não há avaliações
- Sat Kriya Kundalini YogaDocumento2 páginasSat Kriya Kundalini YogacharanAinda não há avaliações
- Swami Sivananda Health and Hatha YogaDocumento409 páginasSwami Sivananda Health and Hatha YogaPaulo CondesAinda não há avaliações
- Vag 401 VW Audi Seat Skoda Function ListDocumento6 páginasVag 401 VW Audi Seat Skoda Function ListMichael KleinAinda não há avaliações
- Guidlines For PL and SS FKLDocumento118 páginasGuidlines For PL and SS FKLKenax1teAinda não há avaliações
- Phase ShiftDocumento1 páginaPhase ShiftdaniAinda não há avaliações
- Imc - VODAFONEDocumento28 páginasImc - VODAFONEPayal Homagni MondalAinda não há avaliações
- Weber Adf PDFDocumento7 páginasWeber Adf PDFCarlos HerreraAinda não há avaliações
- Fire End Croker 2016Documento124 páginasFire End Croker 2016PillaChantasAinda não há avaliações
- Kkcasinonightauction 18Documento4 páginasKkcasinonightauction 18api-185935584Ainda não há avaliações
- Julia A. Ott: 30 Shenandoah Ave Manchester, New Jersey 08759 (732) 691-5524Documento1 páginaJulia A. Ott: 30 Shenandoah Ave Manchester, New Jersey 08759 (732) 691-5524api-263348833Ainda não há avaliações
- (AC-S08) Week 08 - Pre-Task - Quiz - Weekly Quiz - INGLES III (31920)Documento2 páginas(AC-S08) Week 08 - Pre-Task - Quiz - Weekly Quiz - INGLES III (31920)edson antonio heredia tantaricoAinda não há avaliações
- BB BB BB BB BB BBDocumento8 páginasBB BB BB BB BB BBYuri CiabattiAinda não há avaliações
- Rough DraftDocumento5 páginasRough Draftapi-408200501Ainda não há avaliações
- AHA Syllabus For Colour Belts V6Documento26 páginasAHA Syllabus For Colour Belts V6laukuneAinda não há avaliações
- Program Kina Urania 6.4.-12.4.2023Documento2 páginasProgram Kina Urania 6.4.-12.4.2023OsijekNewsAinda não há avaliações
- MK11 - Fatality ListDocumento1 páginaMK11 - Fatality ListJobasces MarinAinda não há avaliações
- The Legend of Zelda Title ThemeDocumento2 páginasThe Legend of Zelda Title ThemeAnonymous NVYl2XdAinda não há avaliações
- Sheiko Cms MsDocumento10 páginasSheiko Cms Mssuboh7231Ainda não há avaliações
- PF2 S02-00 King in Thorns (Tiers 7-8)Documento45 páginasPF2 S02-00 King in Thorns (Tiers 7-8)Túlio Fernandes MoreiraAinda não há avaliações
- 451 849Documento4 páginas451 849Roksana VoloshenyukAinda não há avaliações
- GF v2.50 Point Calc (Beta) v12Documento6 páginasGF v2.50 Point Calc (Beta) v12Hernan GarciaAinda não há avaliações