Você também pode gostar
- Anatomy of The LungsDocumento8 páginasAnatomy of The LungschinecheremnfAinda não há avaliações
- Clinical Anatomy of Respiratory System: Dr. Ridwan Harrianto MHSC (Om), SP - OkDocumento31 páginasClinical Anatomy of Respiratory System: Dr. Ridwan Harrianto MHSC (Om), SP - OkMahasiswa StrugleAinda não há avaliações
- Pleura: LungsDocumento7 páginasPleura: LungsbarbacumlaudeAinda não há avaliações
- Overview of Visceral Thorax - PleuraDocumento33 páginasOverview of Visceral Thorax - PleuraHrishikesh BirjeAinda não há avaliações
- Anatomy of Pluera, Lungs and The Tracheobroncial TreeDocumento108 páginasAnatomy of Pluera, Lungs and The Tracheobroncial TreeTahleel AltafAinda não há avaliações
- Anatomy Notes 3Documento3 páginasAnatomy Notes 3Nia IarajuliAinda não há avaliações
- (Pulmones) : 1e. The LungsDocumento4 páginas(Pulmones) : 1e. The LungszhysanestebanAinda não há avaliações
- Lungs and PleuraDocumento7 páginasLungs and PleuraArvin ArliandoAinda não há avaliações
- Lungs: Objectives of LearningDocumento15 páginasLungs: Objectives of LearningSyeda SapnaAinda não há avaliações
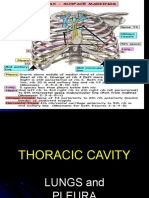
- Surface MarkingsDocumento123 páginasSurface Markingsdrmsupriya091159Ainda não há avaliações
- BronchiectasisDocumento71 páginasBronchiectasisvijay1234568883Ainda não há avaliações
- Lungs-WPS OfficeDocumento23 páginasLungs-WPS Officezenith parmarAinda não há avaliações
- Structure of The Pleurae: Parietal PleuraDocumento7 páginasStructure of The Pleurae: Parietal PleuraGeorge WinchesterAinda não há avaliações
- Unit 6 Part 2 Thoracic CavityDocumento56 páginasUnit 6 Part 2 Thoracic CavitySiraj ShiferawAinda não há avaliações
- Chest X Ray and CollapseDocumento88 páginasChest X Ray and Collapseraseefa hamzaAinda não há avaliações
- Anat Case 2Documento8 páginasAnat Case 2AnanaaAinda não há avaliações
- Trachea, Bronchial Tree and Bronchopulmonary Segments: by Nitisha GuptaDocumento15 páginasTrachea, Bronchial Tree and Bronchopulmonary Segments: by Nitisha GuptaNITISHA GUPTAAinda não há avaliações
- Anat - Respi Gross CompiledDocumento8 páginasAnat - Respi Gross CompiledLeslie Kimberly Lisay100% (1)
- Azygous VeinDocumento12 páginasAzygous VeinLorenz SmallAinda não há avaliações
- Embryology, Gross Anatomy and Histology of Lungs and Pleura: For PC-II Medicine Students By: Zelalem ADocumento58 páginasEmbryology, Gross Anatomy and Histology of Lungs and Pleura: For PC-II Medicine Students By: Zelalem AAmanuel MaruAinda não há avaliações
- Lungs 2014Documento64 páginasLungs 2014atidAinda não há avaliações
- General Anatomy 4 Thoracic Cavity: Dr. Wesam BaderDocumento46 páginasGeneral Anatomy 4 Thoracic Cavity: Dr. Wesam BaderAhmadAinda não há avaliações
- Null 4Documento47 páginasNull 4Kenyan MillanAinda não há avaliações
- Lungs and Pleura Student PC1 2017Documento31 páginasLungs and Pleura Student PC1 2017Obongsamuel IdiongAinda não há avaliações
- THORAX Part 2Documento59 páginasTHORAX Part 2idrimuha333Ainda não há avaliações
- Anatomy of ThoraxDocumento43 páginasAnatomy of ThoraxNunmoy HnialumAinda não há avaliações
- Thoracic cavity & contents: Thorax Unit Lecture 3 & 4 مسعلأا ليلج رديح .دDocumento18 páginasThoracic cavity & contents: Thorax Unit Lecture 3 & 4 مسعلأا ليلج رديح .دMuhammad UsmanAinda não há avaliações
- Trachea, Bronchi, Lungs Bronchopulmonary Segments: Roel Cobarde M.DDocumento25 páginasTrachea, Bronchi, Lungs Bronchopulmonary Segments: Roel Cobarde M.DMiriam JonesAinda não há avaliações
- Bolu Seminar in Lungs 2Documento34 páginasBolu Seminar in Lungs 2Bamgbose OpeyemiAinda não há avaliações
- 20-Trachea, Bronchi & BPSDocumento37 páginas20-Trachea, Bronchi & BPSpm7197362Ainda não há avaliações
- Anatomy RespiratoryDocumento68 páginasAnatomy RespiratorydofezdsAinda não há avaliações
- Anatomy 2Documento43 páginasAnatomy 2bikedet268Ainda não há avaliações
- Thorax LungsDocumento128 páginasThorax LungsVernon MasakayanAinda não há avaliações
- Pleura & LungsDocumento26 páginasPleura & Lungswashma SoomroAinda não há avaliações
- The Thoracic CavityDocumento43 páginasThe Thoracic Cavitybayenn100% (2)
- Gross Anatomy of LungsDocumento8 páginasGross Anatomy of LungsAriguna WijayaAinda não há avaliações
- Dams NotesDocumento28 páginasDams NotesmuskanAinda não há avaliações
- Anatomy Personal NoteDocumento7 páginasAnatomy Personal NoteShereen Al-ObinayAinda não há avaliações
- 1Documento39 páginas1Nadine WangAinda não há avaliações
- Pemeriksaan Fisik ParuDocumento17 páginasPemeriksaan Fisik ParuMuhammad Luthfi AziziAinda não há avaliações
- ScriptDocumento3 páginasScriptAubrey GadorAinda não há avaliações
- Full Text of "Thorax - Notes"Documento10 páginasFull Text of "Thorax - Notes"ᙢᑌᕼᗩᙢᙢᕮᗪ ᗷᗩᖇᔓᘉᒎᓰAinda não há avaliações
- Trachea and LungsDocumento25 páginasTrachea and LungsDr.pallavi kumariAinda não há avaliações
- Trachea, Lungs, Pleura.Documento24 páginasTrachea, Lungs, Pleura.Shimmering MoonAinda não há avaliações
- Anatomy Lec 13 (Lungs)Documento28 páginasAnatomy Lec 13 (Lungs)afzal sulemaniAinda não há avaliações
- Lower Resp TractDocumento32 páginasLower Resp TractTakshikaAinda não há avaliações
- Anatomy, Lecture 5, Pleurae & Lungs (Slides)Documento21 páginasAnatomy, Lecture 5, Pleurae & Lungs (Slides)Ali Al-Qudsi100% (1)
- Lung AnatomyDocumento19 páginasLung AnatomyScott Yee100% (2)
- Unit 5.2 Pleura and LungsDocumento27 páginasUnit 5.2 Pleura and LungsBidhan RegmiAinda não há avaliações
- Checklist 3Documento9 páginasChecklist 3FranklinSappAinda não há avaliações
- The Pleurae and Pleural CavitiesDocumento3 páginasThe Pleurae and Pleural Cavitiesoseko anthonyAinda não há avaliações
- Dissertation On Copd - by - Shivbalak (2013)Documento108 páginasDissertation On Copd - by - Shivbalak (2013)ShivBalakChauhanAinda não há avaliações
- Broncho-Pulmonary SegmentsDocumento29 páginasBroncho-Pulmonary SegmentsArbin PanjaAinda não há avaliações
- The Thorax Part Ii - The Thoracic Cavity: Juan Guido G. Joyo, PTRP Juvi G. Alicabo, PTRP, CCP, CTMBP, CTTTPDocumento98 páginasThe Thorax Part Ii - The Thoracic Cavity: Juan Guido G. Joyo, PTRP Juvi G. Alicabo, PTRP, CCP, CTMBP, CTTTPFerjie Angelica DalandaoAinda não há avaliações
- SURFACE ANATOMY OF LUNGS PPT AssignmentDocumento11 páginasSURFACE ANATOMY OF LUNGS PPT Assignmentshivani100% (2)
- Respiratory Notes (Chris Andersen, ICUPrimaryPrep - Com)Documento14 páginasRespiratory Notes (Chris Andersen, ICUPrimaryPrep - Com)PkernAinda não há avaliações
- A Writer's Guide to Medicine: Volume 2: Illness & InjuryNo EverandA Writer's Guide to Medicine: Volume 2: Illness & InjuryAinda não há avaliações
- Juris Change of Surname 2Documento5 páginasJuris Change of Surname 2mbdelenaAinda não há avaliações
- Rejoin DerDocumento3 páginasRejoin DermbdelenaAinda não há avaliações
- Female Reproductive System - Jan. 22, 24, 2013 - Dr. C. AyochokDocumento10 páginasFemale Reproductive System - Jan. 22, 24, 2013 - Dr. C. AyochokmbdelenaAinda não há avaliações
- 14 Ana Anatomy of Respiration October 1 MontenegroDocumento3 páginas14 Ana Anatomy of Respiration October 1 MontenegrombdelenaAinda não há avaliações
- 12 Ana Kinesiology of Glenohumeral Joint August 16 AbiogDocumento2 páginas12 Ana Kinesiology of Glenohumeral Joint August 16 AbiogmbdelenaAinda não há avaliações
- 1 Ana Intro Finals September 16 LaygoDocumento3 páginas1 Ana Intro Finals September 16 LaygombdelenaAinda não há avaliações
- Coconut Regeneration Guidelines ENGDocumento10 páginasCoconut Regeneration Guidelines ENGmbdelenaAinda não há avaliações
- Organic AcidsDocumento25 páginasOrganic Acidssatti_indianAinda não há avaliações
- 15-Lead ECG PowerpointDocumento20 páginas15-Lead ECG Powerpointgillian102290Ainda não há avaliações
- N, M, M: A M M - B H: Research LetterDocumento9 páginasN, M, M: A M M - B H: Research LetterOlivier BenarrocheAinda não há avaliações
- Feliciano, Troy Ivan Silva, Queenie Rose V. BSN 3-C: Rationale: To Track The Changes of Client's ConditionDocumento4 páginasFeliciano, Troy Ivan Silva, Queenie Rose V. BSN 3-C: Rationale: To Track The Changes of Client's ConditionQueenie SilvaAinda não há avaliações
- SYOK HipovolemikDocumento31 páginasSYOK HipovolemikAmaliahHarumiKarimAinda não há avaliações
- Materi HE GinjalDocumento61 páginasMateri HE GinjalYafi Dyah C.IAinda não há avaliações
- Nursing Review BulletsDocumento125 páginasNursing Review BulletsROBERT C. REÑA, BSN, RN, MAN (ue)96% (46)
- An Are Rob I C DegradationDocumento18 páginasAn Are Rob I C DegradationMartuchis EstradaAinda não há avaliações
- 10 Interesting Facts About CatsDocumento8 páginas10 Interesting Facts About CatsAndreea DanaAinda não há avaliações
- Pediatrics Protocols - Pediatric Handbook 3rd EditionDocumento25 páginasPediatrics Protocols - Pediatric Handbook 3rd Editionklteng85Ainda não há avaliações
- Detection of Leukemia in Human Blood Sample Based On Microscopic Images: A StudyDocumento8 páginasDetection of Leukemia in Human Blood Sample Based On Microscopic Images: A StudySaku RaAinda não há avaliações
- Systems and Disease II ComprehensiveDocumento54 páginasSystems and Disease II Comprehensivenasr234Ainda não há avaliações
- Omm Exam 3 LGTDocumento59 páginasOmm Exam 3 LGTSolomon Seth SallforsAinda não há avaliações
- 5090 w10 Ms 61Documento3 páginas5090 w10 Ms 61mstudy123456Ainda não há avaliações
- Quiz - Bones and MusclesDocumento1 páginaQuiz - Bones and MusclesSimranAinda não há avaliações
- Craniofacial Osteotomies For Hidden Head & Neck LesionsDocumento4 páginasCraniofacial Osteotomies For Hidden Head & Neck LesionsMohammad AkheelAinda não há avaliações
- Human Biology ATAR Y11 Sample Course Outline WACE 201516 - PDFDocumento4 páginasHuman Biology ATAR Y11 Sample Course Outline WACE 201516 - PDFpartyAinda não há avaliações
- Breathing Secrets v1-2Documento34 páginasBreathing Secrets v1-2Eduardo100% (4)
- DXN Is The Perfect BusinessDocumento45 páginasDXN Is The Perfect Businesssomasekharvasudevan83% (6)
- Dental MCQDocumento22 páginasDental MCQPinpointq0% (1)
- Pharmacology HandoutDocumento84 páginasPharmacology Handoutnanashimii100% (4)
- Ibo (The International Biology Olympiad)Documento6 páginasIbo (The International Biology Olympiad)RadpandjiAinda não há avaliações
- Physioex Lab Report: Pre-Lab Quiz ResultsDocumento3 páginasPhysioex Lab Report: Pre-Lab Quiz ResultsNicole de LeonAinda não há avaliações
- Different Approaches in Pharmacological ResearchDocumento3 páginasDifferent Approaches in Pharmacological ResearcharcherselevatorsAinda não há avaliações
- Pharmacology of Antipyretic DrugsDocumento19 páginasPharmacology of Antipyretic DrugsPretty HiaAinda não há avaliações
- Herniated Nucleus PulposusDocumento3 páginasHerniated Nucleus PulposusroselleanneAinda não há avaliações
- VerapamilDocumento2 páginasVerapamilMyla Reyes San MiguelAinda não há avaliações
- CHPT 70 Respiratory Part 2Documento56 páginasCHPT 70 Respiratory Part 2helen brockAinda não há avaliações
- ABSITEDocumento6 páginasABSITEhp0% (1)
- Syllabus NCM 103Documento11 páginasSyllabus NCM 103ivanguzman86Ainda não há avaliações