Você também pode gostar
- Charts For Kidney and Lower Urinary Tract Pathology. NephrologyDocumento34 páginasCharts For Kidney and Lower Urinary Tract Pathology. NephrologyM PatelAinda não há avaliações
- Renal Vascular Disease GuideDocumento46 páginasRenal Vascular Disease GuideCoy NuñezAinda não há avaliações
- Renal Path Q'sDocumento20 páginasRenal Path Q'skank_sAinda não há avaliações
- Robbins Ch. 26 Bones Joints and Soft-Tissue Tumors Review QuestionsDocumento7 páginasRobbins Ch. 26 Bones Joints and Soft-Tissue Tumors Review QuestionsPA2014100% (1)
- 1 Patho5 - Kidney I 2015bDocumento10 páginas1 Patho5 - Kidney I 2015bmiguel cuevasAinda não há avaliações
- Glomerular Diseases, Cysts, Renal Stones 2Documento7 páginasGlomerular Diseases, Cysts, Renal Stones 2Idris AdeoyeAinda não há avaliações
- Nephrology ReviewerDocumento3 páginasNephrology ReviewerNix14Ainda não há avaliações
- Gastrointestinal PathologyDocumento14 páginasGastrointestinal PathologyRahul ShuklaAinda não há avaliações
- Pathology PDFDocumento28 páginasPathology PDFRoman PanditAinda não há avaliações
- Robbin's SummariesDocumento98 páginasRobbin's SummariesnopedontsuemepleaseAinda não há avaliações
- Robbins Ch. 20 The Kidney Review QuestionsDocumento10 páginasRobbins Ch. 20 The Kidney Review QuestionsPA2014100% (4)
- GASTROINSTINAL TRACT Robbins 8th EditionDocumento4 páginasGASTROINSTINAL TRACT Robbins 8th EditionLim EricAinda não há avaliações
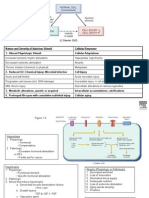
- Endocrine Gland Hormone(s) Secreted Stimulus Effect of Hormone Inhibition PathologyDocumento3 páginasEndocrine Gland Hormone(s) Secreted Stimulus Effect of Hormone Inhibition PathologySamuelAinda não há avaliações
- The Most CommonsDocumento80 páginasThe Most CommonsJmee8Ainda não há avaliações
- Lecture 29 - Pathology of HypertensionDocumento24 páginasLecture 29 - Pathology of Hypertensionapi-3703352100% (6)
- Ch.1 Baby Robbins OutlineDocumento11 páginasCh.1 Baby Robbins OutlinePA2014100% (3)
- Basic Examination of Urine - Dr. PinedaDocumento20 páginasBasic Examination of Urine - Dr. PinedaElei GarciaAinda não há avaliações
- Chapter 7 Neoplasia 1 2 Robbins and Cotran Pathologic Basis of Disease PDFDocumento9 páginasChapter 7 Neoplasia 1 2 Robbins and Cotran Pathologic Basis of Disease PDFChethranAinda não há avaliações
- Renal Disease McqsDocumento20 páginasRenal Disease McqsShankar Deshmukh100% (1)
- Hematologic Pathology p65-87Documento23 páginasHematologic Pathology p65-87zeroun24100% (1)
- Clinical case study on pathological findings and diagnosesDocumento28 páginasClinical case study on pathological findings and diagnosesshubham royalAinda não há avaliações
- Test Bank On GI PathologyDocumento14 páginasTest Bank On GI PathologySeff CausapinAinda não há avaliações
- SURGPATH - 2.1 The Gastrointestinal Tract (Robbins) - TableDocumento8 páginasSURGPATH - 2.1 The Gastrointestinal Tract (Robbins) - TableAngela Caguitla100% (1)
- Chapter 11 Blood Vessels 8th Ed NotesDocumento7 páginasChapter 11 Blood Vessels 8th Ed NotesKyle Christopher SiaAinda não há avaliações
- Causes, Types and Morphology of Cell Injury and DeathDocumento18 páginasCauses, Types and Morphology of Cell Injury and DeathYoja GarzonAinda não há avaliações
- Robbins Ch. 18 Liver and Biliary Tract Review QuestionsDocumento12 páginasRobbins Ch. 18 Liver and Biliary Tract Review QuestionsPA2014Ainda não há avaliações
- Gastroenterology: Diseases of The EsophagusDocumento18 páginasGastroenterology: Diseases of The EsophagusKayeshiana30Ainda não há avaliações
- Inflammatory Response and Vascular Permeability ChangesDocumento20 páginasInflammatory Response and Vascular Permeability Changesjeffaguilar100% (2)
- 5 6057345046456304562Documento490 páginas5 6057345046456304562DK DeepakAinda não há avaliações
- Pathology Week 6 p18-35Documento18 páginasPathology Week 6 p18-35zeroun24Ainda não há avaliações
- 2021 Systemic Pathology S4T1 - RBC and Bleeding Disorders PDFDocumento27 páginas2021 Systemic Pathology S4T1 - RBC and Bleeding Disorders PDFAlexis Bondad100% (1)
- Chapter 13 Neoplastic Proliferations of White CellsDocumento16 páginasChapter 13 Neoplastic Proliferations of White CellsOmar100% (1)
- Toronto Notes Nephrology 2015 22Documento1 páginaToronto Notes Nephrology 2015 22JUSASB0% (1)
- DISC, Drugs, Infection, Thick Basal MembraneDocumento5 páginasDISC, Drugs, Infection, Thick Basal MembraneHOPEAinda não há avaliações
- Cellular InjuryDocumento26 páginasCellular InjuryRitz CelsoAinda não há avaliações
- Cellular Injury, Adaptation and Cell DeathDocumento8 páginasCellular Injury, Adaptation and Cell DeathJessica Febrina Wuisan100% (1)
- Cell Adaptation and Necrosis: Hypertrophy, Atrophy, MetaplasiaDocumento8 páginasCell Adaptation and Necrosis: Hypertrophy, Atrophy, MetaplasiaivankcurryAinda não há avaliações
- Imm Pathology 2016Documento43 páginasImm Pathology 2016Aamir Hamaad100% (3)
- Pathology Finals Reviewer on WBCs, Lymph Nodes, Spleen & ThymusDocumento5 páginasPathology Finals Reviewer on WBCs, Lymph Nodes, Spleen & Thymusangel_sagun_1Ainda não há avaliações
- ENDOCRINE PATHOLOGY WebpathDocumento35 páginasENDOCRINE PATHOLOGY Webpathapi-3766657Ainda não há avaliações
- Endocrine Pathology p17-32Documento16 páginasEndocrine Pathology p17-32zeroun24Ainda não há avaliações
- Patho Robbins Sumary Pereira MDDocumento22 páginasPatho Robbins Sumary Pereira MDNicole SarcosAinda não há avaliações
- Table of Genetic Disorders: Download A Copy of This Study GuideDocumento11 páginasTable of Genetic Disorders: Download A Copy of This Study Guideerica perezAinda não há avaliações
- Robbins Pathology Chapter 24 - EndocrineDocumento2 páginasRobbins Pathology Chapter 24 - Endocrinescorpiosphinx79100% (2)
- Pediatrics SamplexDocumento6 páginasPediatrics SamplexThea SansonAinda não há avaliações
- Blood Vessels QuizDocumento28 páginasBlood Vessels Quiztatti999Ainda não há avaliações
- WBC Pathology: Lecturer: Associate Professor T. A. GrekovaDocumento49 páginasWBC Pathology: Lecturer: Associate Professor T. A. GrekovaFaheem MusthafaAinda não há avaliações
- Chapter 5 (Questions 2008-2009 Compiled)Documento28 páginasChapter 5 (Questions 2008-2009 Compiled)vetpathforumAinda não há avaliações
- MCQs Glomerular Injury Pathogenesis, Nephritic SyndromeDocumento5 páginasMCQs Glomerular Injury Pathogenesis, Nephritic SyndromeIshita SinghAinda não há avaliações
- Pathology 1Documento38 páginasPathology 1ARNOLD BORROMEOAinda não há avaliações
- Physiologic Monitoring of The Surgical PatientDocumento56 páginasPhysiologic Monitoring of The Surgical PatientSeid Adem100% (2)
- Pancreatic Hormones and Antidiabetic AgentsDocumento3 páginasPancreatic Hormones and Antidiabetic AgentsChristian DeeAinda não há avaliações
- Pathology of Liver, Biliary, and PancreasDocumento52 páginasPathology of Liver, Biliary, and PancreasHassan.shehri100% (11)
- Hemodynamic Disorders, Thromboembolic Disease, and ShockDocumento87 páginasHemodynamic Disorders, Thromboembolic Disease, and Shockgifty100% (1)
- Renal Questions by Dr. OkashaDocumento78 páginasRenal Questions by Dr. Okashamohammed okashaAinda não há avaliações
- Kidney Stones and Blood Vessel Diseases ExplainedDocumento19 páginasKidney Stones and Blood Vessel Diseases ExplainedmadhuAinda não há avaliações
- Renal DiseaseDocumento191 páginasRenal Diseasetokkeetak13Ainda não há avaliações
- Kidney, Bladder and Prostate Pathology For Allied Health SciencesDocumento38 páginasKidney, Bladder and Prostate Pathology For Allied Health SciencesMichael BrownAinda não há avaliações
- Renal PathologyDocumento34 páginasRenal PathologyShanaz ShaxawanAinda não há avaliações
- The Kidney Bereket FinalDocumento81 páginasThe Kidney Bereket FinalMai Kutin KoakAinda não há avaliações
- The EyeDocumento16 páginasThe Eyenbaumgartner0Ainda não há avaliações
- Histology Powerpoint ReviewDocumento29 páginasHistology Powerpoint Reviewnbaumgartner0Ainda não há avaliações
- Histology Final Exam Practice Test KeyDocumento13 páginasHistology Final Exam Practice Test Keynbaumgartner0100% (7)
- Cranial NervesDocumento4 páginasCranial Nervesnbaumgartner0Ainda não há avaliações
- One Lines Spring Exam 2Documento16 páginasOne Lines Spring Exam 2nbaumgartner0Ainda não há avaliações
- Anterior Triangle of The Neck Dr. BanezDocumento6 páginasAnterior Triangle of The Neck Dr. BanezMelissa SalayogAinda não há avaliações
- Anatomy Physiology Pre Final ExamDocumento4 páginasAnatomy Physiology Pre Final ExamFatima AsisAinda não há avaliações
- Big Picture Big Picture Practice July 2017Documento2 páginasBig Picture Big Picture Practice July 2017Edison halim100% (1)
- Human Anatomy and PhysiologyDocumento68 páginasHuman Anatomy and PhysiologyAbby Umali-Hernandez100% (3)
- Content in Demo TeachingDocumento6 páginasContent in Demo TeachingAgustines, Marie Char C.Ainda não há avaliações
- ANATOMY OF HATHA YOGA by H.david Coulter PDFDocumento493 páginasANATOMY OF HATHA YOGA by H.david Coulter PDFAnnick LîlâAinda não há avaliações
- Group 6 Blood Analysis 2Documento6 páginasGroup 6 Blood Analysis 2Kim TangoAinda não há avaliações
- MSU Case Study #1Documento2 páginasMSU Case Study #1Tracy MeadowsAinda não há avaliações
- Hormone RegulationDocumento21 páginasHormone RegulationJhansi Reddy TamatamAinda não há avaliações
- Blood Transfusion Guideline PDFDocumento26 páginasBlood Transfusion Guideline PDFEmhemed Amer TabibAinda não há avaliações
- The Digestive System Notes - Grade 9Documento3 páginasThe Digestive System Notes - Grade 9bd6cpynwmpAinda não há avaliações
- Internal Organs of Human BodyDocumento6 páginasInternal Organs of Human BodyVimalaChristinalAinda não há avaliações
- Prof 1, Sem 1 L 45 - CLASSIFICATION OF AKHLAT (HUMOURSDocumento14 páginasProf 1, Sem 1 L 45 - CLASSIFICATION OF AKHLAT (HUMOURSMI Manuha100% (1)
- Neoplasia: Study of New Cell Growths and TumorsDocumento9 páginasNeoplasia: Study of New Cell Growths and TumorsDocAxi Maximo Jr Axibal67% (6)
- Myringoplasty and TympanoplastyDocumento20 páginasMyringoplasty and TympanoplastyAsiya Zaidi100% (1)
- 6 Life ProcessesDocumento39 páginas6 Life ProcessesPrashant Sirohi50% (2)
- Painting Pictures of Success Initiates Inner Process of ElevationDocumento57 páginasPainting Pictures of Success Initiates Inner Process of ElevationrerenAinda não há avaliações
- 81: Mammalian Heart and Its RegulationDocumento75 páginas81: Mammalian Heart and Its RegulationIt's Ika100% (1)
- Study Questions Special SensesDocumento37 páginasStudy Questions Special SensesSurajit Bhattacharjee93% (14)
- Hering's Law of Direction of CureDocumento6 páginasHering's Law of Direction of Curekaravi schiniasAinda não há avaliações
- Complete Blood Count-2023-08-29t00 - 00 - 00Documento2 páginasComplete Blood Count-2023-08-29t00 - 00 - 00Michamiel SerratoAinda não há avaliações
- Transport Across CapillariesDocumento21 páginasTransport Across CapillariesDoc HamsAinda não há avaliações
- Primordial Germ CellsDocumento6 páginasPrimordial Germ CellsAll in one learners With WajihaAinda não há avaliações
- IGCSE Biology Workbook Chapter on Coordination and ResponseDocumento10 páginasIGCSE Biology Workbook Chapter on Coordination and ResponseЙордан БайчевAinda não há avaliações
- Muscle Tissue OutlineDocumento4 páginasMuscle Tissue OutlinePeachy PieAinda não há avaliações
- Worksheet 1.2 Organelle QuizDocumento3 páginasWorksheet 1.2 Organelle QuizCyndel TindoyAinda não há avaliações
- Leeward Microbiology 130 DR - Kae Final ExamDocumento164 páginasLeeward Microbiology 130 DR - Kae Final Examraymond theardAinda não há avaliações
- 2018, 840 Pages, Colour Plates, Gures, Tables 25cm: ISBN 938654648-5Documento822 páginas2018, 840 Pages, Colour Plates, Gures, Tables 25cm: ISBN 938654648-5Iryna ZapekaAinda não há avaliações
- Histology Laboratory Manual: Olgga A. Hara MSDocumento77 páginasHistology Laboratory Manual: Olgga A. Hara MSMark LopezAinda não há avaliações
- EET312 BMI Module 1Documento110 páginasEET312 BMI Module 1Thasneem FathimaAinda não há avaliações