Você também pode gostar
- Maximizing Auditory SlidesDocumento18 páginasMaximizing Auditory SlidesARUNGREESMAAinda não há avaliações
- Aphasia: Hana Nabila Ulfia 1102014118Documento14 páginasAphasia: Hana Nabila Ulfia 1102014118hana nabilaAinda não há avaliações
- Comprehensive Handbook of Pediatric Audiology - (23 Behavioral Audiometry in Infants and Children)Documento18 páginasComprehensive Handbook of Pediatric Audiology - (23 Behavioral Audiometry in Infants and Children)Juliane NascimentoAinda não há avaliações
- Dysarthria ChartDocumento12 páginasDysarthria ChartTalia Garcia100% (1)
- Diseases of Esophagus.Documento3 páginasDiseases of Esophagus.Isabel Castillo100% (2)
- Treatment of Wernicke'S Aphasia With Jargon: A Case StudyDocumento11 páginasTreatment of Wernicke'S Aphasia With Jargon: A Case StudyIvanaAinda não há avaliações
- DysarthriaDocumento2 páginasDysarthriaBanjo VergaraAinda não há avaliações
- Normal Non - Fluency, Primary Stuttering and Secondary StutteringDocumento21 páginasNormal Non - Fluency, Primary Stuttering and Secondary StutteringK PAinda não há avaliações
- Dysphagia After Total LaryngectomyDocumento6 páginasDysphagia After Total LaryngectomyEduardo Lima de Melo Jr.Ainda não há avaliações
- AphasiaDocumento8 páginasAphasiaapi-308647214Ainda não há avaliações
- Language - NeuroDocumento15 páginasLanguage - NeuroAifa Afeeqa Jamilan100% (1)
- Auditory Brainstem Response - ABR - in Clinical Practice PDFDocumento9 páginasAuditory Brainstem Response - ABR - in Clinical Practice PDFary wisma dewiAinda não há avaliações
- Approaches To Management of Stuttering (Piyush Malviya)Documento11 páginasApproaches To Management of Stuttering (Piyush Malviya)Piyush MalviyaAinda não há avaliações
- Mbs De-IdentifiedDocumento2 páginasMbs De-Identifiedapi-645942287Ainda não há avaliações
- APPROACHES TO MANAGEMENT OF FLUENCY DISORDERS - PDF / KUNNAMPALLIL GEJODocumento150 páginasAPPROACHES TO MANAGEMENT OF FLUENCY DISORDERS - PDF / KUNNAMPALLIL GEJOKUNNAMPALLIL GEJO JOHN100% (2)
- Aca - 1Documento28 páginasAca - 1Aparna LVAinda não há avaliações
- Theoretical Constructs in Fluency Development - PDF / KUNNAMPALLIL GEJODocumento74 páginasTheoretical Constructs in Fluency Development - PDF / KUNNAMPALLIL GEJOKUNNAMPALLIL GEJO JOHN100% (1)
- Classification of Velopharyngeal DysfunctionDocumento1 páginaClassification of Velopharyngeal DysfunctionVictoria Rojas AlvearAinda não há avaliações
- Aphasia, Apraxia, and Agnosia AphasiaDocumento7 páginasAphasia, Apraxia, and Agnosia Aphasiasomebody_maAinda não há avaliações
- Cognitive Linguistic Assessment Protocol For Adults - Kannada Clap-KDocumento47 páginasCognitive Linguistic Assessment Protocol For Adults - Kannada Clap-KSureaka PonnusamyAinda não há avaliações
- Van RiperDocumento1 páginaVan RiperSadaf RizwanhumayoonAinda não há avaliações
- FEES6Documento36 páginasFEES6Justy GuavaAinda não há avaliações
- 12724688Documento98 páginas12724688Melandes Tamiris100% (1)
- Pediatric Voice Handicap Index (pVHI) : A New Tool For Evaluating Pediatric DysphoniaDocumento6 páginasPediatric Voice Handicap Index (pVHI) : A New Tool For Evaluating Pediatric DysphoniaDiego Vargas LópezAinda não há avaliações
- Habla ClaraDocumento14 páginasHabla ClaraCristóbal Landeros TorresAinda não há avaliações
- Effectiveness of Deep Pharyngeal Neuromuscular Stimulation Versus Thermal Gustatory Stimulation in Decreasing Length of Swallow Initiation and Improving Lingual Movements - Maria H WillisDocumento54 páginasEffectiveness of Deep Pharyngeal Neuromuscular Stimulation Versus Thermal Gustatory Stimulation in Decreasing Length of Swallow Initiation and Improving Lingual Movements - Maria H WillisconstantineeliaAinda não há avaliações
- Voice Anatomy2Documento49 páginasVoice Anatomy2Jerônimo Feitosa100% (1)
- 2013 What Works - Speech Sound Disorders UpdateDocumento26 páginas2013 What Works - Speech Sound Disorders UpdatemariaAinda não há avaliações
- Rehabilitation Esophageal Speech & Artificial LarynxDocumento50 páginasRehabilitation Esophageal Speech & Artificial LarynxKUNNAMPALLIL GEJO JOHN100% (2)
- ORLADocumento10 páginasORLACarol CoelhoAinda não há avaliações
- Feeding Evaluation Report Client Name: Date Evaluated: D.O.B. TherapistDocumento41 páginasFeeding Evaluation Report Client Name: Date Evaluated: D.O.B. Therapistlisa de los santos100% (1)
- An Investigation Into Infant Cry and Apgar Score Using Principle Component AnalysisDocumento6 páginasAn Investigation Into Infant Cry and Apgar Score Using Principle Component AnalysisSaranya N MuthuAinda não há avaliações
- ApraxiaDocumento7 páginasApraxiagemapesfAinda não há avaliações
- Joseph C. Stemple - Edie R Hapner - Voice Therapy - Clinical Case Studies-Plural Publishing (2019)Documento531 páginasJoseph C. Stemple - Edie R Hapner - Voice Therapy - Clinical Case Studies-Plural Publishing (2019)szeho chanAinda não há avaliações
- CAPD Check ListDocumento12 páginasCAPD Check ListCaio LeônidasAinda não há avaliações
- Proforma For Fluency Disorders / KUNNAMPALLIL GEJODocumento2 páginasProforma For Fluency Disorders / KUNNAMPALLIL GEJOKUNNAMPALLIL GEJO JOHNAinda não há avaliações
- Cad TestDocumento8 páginasCad TestSajjadAhmad_QMCAinda não há avaliações
- Flaccid DysarthriaDocumento40 páginasFlaccid Dysarthriaaleeza nomanAinda não há avaliações
- Post Stroke WritingDocumento9 páginasPost Stroke WritingAdi ParamarthaAinda não há avaliações
- Efficacy of Stuttering Therapies - PDF /KUNNAMPALLIL GEJODocumento24 páginasEfficacy of Stuttering Therapies - PDF /KUNNAMPALLIL GEJOKUNNAMPALLIL GEJO JOHNAinda não há avaliações
- Management For Multiple HandicapDocumento57 páginasManagement For Multiple HandicapMSc Audio BAinda não há avaliações
- AphasiaDocumento29 páginasAphasiaHannan FarooqAinda não há avaliações
- TRANSFER, MAINTANENCE, RECOVERY & RELAPSE OF STUTTERING - PDF / KUNNAMPALLIL GEJO JOHNDocumento50 páginasTRANSFER, MAINTANENCE, RECOVERY & RELAPSE OF STUTTERING - PDF / KUNNAMPALLIL GEJO JOHNKUNNAMPALLIL GEJO JOHN100% (5)
- Admission:Discharge Criteria in Speech-Language Pathology - ASHADocumento16 páginasAdmission:Discharge Criteria in Speech-Language Pathology - ASHANádia MarquesAinda não há avaliações
- Aphasia: Western Aphasia Battery (WAB)Documento13 páginasAphasia: Western Aphasia Battery (WAB)amandaAinda não há avaliações
- Western Aphasia Battery Revised Pearson Clinical NaDocumento4 páginasWestern Aphasia Battery Revised Pearson Clinical NaBryan Kagz0% (1)
- 2014mshahandouts StoeckelDocumento37 páginas2014mshahandouts StoeckelAna Vogeley100% (1)
- Assessment and Treatment of Linguistic Deficits PDFDocumento96 páginasAssessment and Treatment of Linguistic Deficits PDFJumraini TammasseAinda não há avaliações
- Voice and Speech DisordersDocumento2 páginasVoice and Speech DisordersVishal Gaurav100% (1)
- A Bright SPPARC.Documento3 páginasA Bright SPPARC.Speech & Language Therapy in PracticeAinda não há avaliações
- Development of StutteringDocumento8 páginasDevelopment of StutteringSiha SalamAinda não há avaliações
- Language Aphasia: Lecture By: M.K. SastryDocumento15 páginasLanguage Aphasia: Lecture By: M.K. SastryAnonymous 5IUoLwGSdAinda não há avaliações
- Objetivos ICF-Speech-Sound-Disorder (ASHA)Documento2 páginasObjetivos ICF-Speech-Sound-Disorder (ASHA)labavillaAinda não há avaliações
- A Teacher's Voice - A Voical Hygiene Workshop-BL20Documento23 páginasA Teacher's Voice - A Voical Hygiene Workshop-BL20AngelaAinda não há avaliações
- 017 Speech Motor Dynamics in Stuttering (Peters) - FuturoFonoDocumento409 páginas017 Speech Motor Dynamics in Stuttering (Peters) - FuturoFonoJuli MirandaAinda não há avaliações
- TBL 3: Dysphagia: By: Anis, Aishah, Nubla, Hanafi, HidayahDocumento84 páginasTBL 3: Dysphagia: By: Anis, Aishah, Nubla, Hanafi, HidayahNadia RahimAinda não há avaliações
- Dysphagia Handicap Index, Development and ValidationDocumento7 páginasDysphagia Handicap Index, Development and ValidationWlf OoAinda não há avaliações
- Motor Speech Disorders in Pediatric Practice Childhood Motor Speech DisordersDocumento21 páginasMotor Speech Disorders in Pediatric Practice Childhood Motor Speech DisordersSwathi GeethaAinda não há avaliações
- A Comparison of Two Treatments For Childhood Apraxia of Speech - Methods and Treatment Protocol For A Parallel Group Randomised Control TrialDocumento9 páginasA Comparison of Two Treatments For Childhood Apraxia of Speech - Methods and Treatment Protocol For A Parallel Group Randomised Control TrialCamila CruzAinda não há avaliações
- Essential Communication SkillsDocumento85 páginasEssential Communication SkillsdarsunaddictedAinda não há avaliações
- Vocal Fold HistologyDocumento1 páginaVocal Fold HistologydarsunaddictedAinda não há avaliações
- OAE Pediatrician BookletDocumento22 páginasOAE Pediatrician BookletKalpana ParajuliAinda não há avaliações
- Uk Plummer VinsonSyndrome2005Documento5 páginasUk Plummer VinsonSyndrome2005darsunaddictedAinda não há avaliações
- Esophageal Foreign Bodies PDFDocumento7 páginasEsophageal Foreign Bodies PDFdarsunaddictedAinda não há avaliações
- PresbycusisDocumento5 páginasPresbycusisdarsunaddictedAinda não há avaliações
- Chapter 23 Maxillofacial TraumaDocumento29 páginasChapter 23 Maxillofacial TraumadarsunaddictedAinda não há avaliações
- Verrucous Carcinoma Ackerman'sDocumento3 páginasVerrucous Carcinoma Ackerman'sdarsunaddictedAinda não há avaliações
- Otolaryngology-Head and Neck Surgery: Author GuidelinesDocumento5 páginasOtolaryngology-Head and Neck Surgery: Author GuidelinesdarsunaddictedAinda não há avaliações
- 9-Rubella in Pregnancy, SOGC O8Documento7 páginas9-Rubella in Pregnancy, SOGC O8Taufan LutfiAinda não há avaliações
- Indication For BronchosDocumento2 páginasIndication For BronchosdarsunaddictedAinda não há avaliações
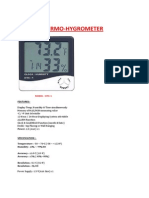
- Digital Thermo Hygrometer (HTC-1)Documento1 páginaDigital Thermo Hygrometer (HTC-1)darsunaddictedAinda não há avaliações
- Hand Hygiene Observation ToolDocumento1 páginaHand Hygiene Observation TooldarsunaddictedAinda não há avaliações
- Concept Paper Deaf Languages UploadDocumento9 páginasConcept Paper Deaf Languages UploadCecile Savercool CarpenterAinda não há avaliações
- THT Gambaran MTDocumento109 páginasTHT Gambaran MTCindy RiannieAinda não há avaliações
- Service Manual: Stereo Preamp MixerDocumento11 páginasService Manual: Stereo Preamp MixerAndrewWerdnaAinda não há avaliações
- RM Important Questions at VenkyDocumento15 páginasRM Important Questions at VenkyVenkateshYadavCivarlaAinda não há avaliações
- Lab 1 Compile SBFDocumento15 páginasLab 1 Compile SBFAin SufizaAinda não há avaliações
- Oticon More New Evidence - Reducing Sustained Listening EffortDocumento8 páginasOticon More New Evidence - Reducing Sustained Listening EffortAlAinda não há avaliações
- Science Chapter - (Sound) Class 8Documento8 páginasScience Chapter - (Sound) Class 8Khushi Kumari class 9 adm 664Ainda não há avaliações
- Menieres Disease A Review On Epidemiology Aetiology Diagnosis and TreatmentDocumento12 páginasMenieres Disease A Review On Epidemiology Aetiology Diagnosis and TreatmentGung ArdhiaAinda não há avaliações
- ECEPE3 - Lesson 1 AcousticsDocumento42 páginasECEPE3 - Lesson 1 AcousticsGenesis AlquizarAinda não há avaliações
- Stravinsky - The Rite of Spring (Full Score) PDFDocumento161 páginasStravinsky - The Rite of Spring (Full Score) PDFgotchimusicAinda não há avaliações
- SNA-Davis-Chapter 15 NoiseDocumento23 páginasSNA-Davis-Chapter 15 NoiseShanthini KaurAinda não há avaliações
- 13 SoundDocumento16 páginas13 SoundBhaskar T IsacAinda não há avaliações
- Hearing Aids System For Impaired Peoples: January 2004Documento5 páginasHearing Aids System For Impaired Peoples: January 2004Anvitha LokepalliAinda não há avaliações
- Aspects of Hearing Aids Fitting ProceduresDocumento150 páginasAspects of Hearing Aids Fitting ProceduresakAinda não há avaliações
- Criteria For Low Frequency Noise: 19 International Congress On Acoustics Madrid, 2-7 September 2007Documento0 páginaCriteria For Low Frequency Noise: 19 International Congress On Acoustics Madrid, 2-7 September 2007jsrgirAinda não há avaliações
- Daftar PustakaDocumento2 páginasDaftar PustakaRia Rizki JayantiAinda não há avaliações
- Mic/Line Mixer Owners ManualDocumento11 páginasMic/Line Mixer Owners Manualnaphon_hkAinda não há avaliações
- ACOUSTICSDocumento17 páginasACOUSTICSJeremiash ForondaAinda não há avaliações
- Difficulty in Hearing: Prepared By: Francis Quarre Lyka Jane Roguel John Lester Romero Alana Marees DolosoDocumento31 páginasDifficulty in Hearing: Prepared By: Francis Quarre Lyka Jane Roguel John Lester Romero Alana Marees DolosoJessa Mae SusonAinda não há avaliações
- Menier's Disease Ayurvedic TreatmentDocumento5 páginasMenier's Disease Ayurvedic TreatmentAmmiraju Gorti ChoudharyAinda não há avaliações
- Dynacord PDFDocumento204 páginasDynacord PDFRafRouf SehiliAinda não há avaliações
- 8EM PHYSoundDocumento18 páginas8EM PHYSoundsreekanthkataAinda não há avaliações
- Overview of Special EducationDocumento51 páginasOverview of Special EducationKhaira Racel Jay PucotAinda não há avaliações
- 15 Inch Two-Way Speaker: Professional SeriesDocumento2 páginas15 Inch Two-Way Speaker: Professional Seriesambet TayloAinda não há avaliações
- The Sonic Wonders of The WorldDocumento313 páginasThe Sonic Wonders of The WorldDamian Payo100% (1)
- Physical Assessment EarsDocumento65 páginasPhysical Assessment EarsDeeeeeAinda não há avaliações
- Unit 24 Task 2Documento4 páginasUnit 24 Task 2api-487574488Ainda não há avaliações
- Price List PDFDocumento9 páginasPrice List PDFrakkaraulAinda não há avaliações
- CT Imaging of The Temporal Bone: An Anatomical Review With Illustrative Cases of CholesteatomasDocumento116 páginasCT Imaging of The Temporal Bone: An Anatomical Review With Illustrative Cases of CholesteatomasDr-Firas Nayf Al-Thawabia100% (1)