Você também pode gostar
- Some Elements of Proportion and Optical Image Support in A TypefaceDocumento6 páginasSome Elements of Proportion and Optical Image Support in A TypefacesudhirnairAinda não há avaliações
- Sports Abhishek Sharma IMT GhaziabadDocumento10 páginasSports Abhishek Sharma IMT GhaziabadsudhirnairAinda não há avaliações
- Impact of Generic SubstitutionDocumento11 páginasImpact of Generic SubstitutionsudhirnairAinda não há avaliações
- Sports RVRKAbhishekSharma MDIDocumento11 páginasSports RVRKAbhishekSharma MDIsudhirnairAinda não há avaliações
- Healthcare Siddhartha Sarkar SP JainDocumento10 páginasHealthcare Siddhartha Sarkar SP JainsudhirnairAinda não há avaliações
- Sports SameerSinghal MDIDocumento9 páginasSports SameerSinghal MDIsudhirnairAinda não há avaliações
- Irrigation C Anand IIM IndoreDocumento10 páginasIrrigation C Anand IIM IndoresudhirnairAinda não há avaliações
- Waste Management - Jasleen Arora - IIFT DelhiDocumento10 páginasWaste Management - Jasleen Arora - IIFT DelhisudhirnairAinda não há avaliações
- River Pollution - Saikat Mondal - IIM LucknowDocumento11 páginasRiver Pollution - Saikat Mondal - IIM Lucknowsudhirnair0% (1)
- Waste Management - Bhavin Shah - IIM IndoreDocumento10 páginasWaste Management - Bhavin Shah - IIM IndoresudhirnairAinda não há avaliações
- River Pollution - Akshat Trivedi - IIM IndoreDocumento12 páginasRiver Pollution - Akshat Trivedi - IIM IndoresudhirnairAinda não há avaliações
- River Pollution Saloni Gupta XLRIDocumento10 páginasRiver Pollution Saloni Gupta XLRIsudhirnair100% (1)
- Waste Management - Asit Kumar Jain - IIM ShillongDocumento9 páginasWaste Management - Asit Kumar Jain - IIM ShillongsudhirnairAinda não há avaliações
- Waste Management Gaurav Tomar IMTDocumento10 páginasWaste Management Gaurav Tomar IMTsudhirnairAinda não há avaliações
- Sports Vaibhav Maheshwari XLRIDocumento12 páginasSports Vaibhav Maheshwari XLRIsudhirnairAinda não há avaliações
- Irrigation Ashutosh Dikshit IIM ShillongDocumento12 páginasIrrigation Ashutosh Dikshit IIM ShillongsudhirnairAinda não há avaliações
- Sports Sudharsan Narayanan IIM IndoreDocumento9 páginasSports Sudharsan Narayanan IIM IndoresudhirnairAinda não há avaliações
- River Pollution Ramaa Ramesh XLRIDocumento10 páginasRiver Pollution Ramaa Ramesh XLRIsudhirnairAinda não há avaliações
- Healthcare Karthik R IIM IndoreDocumento10 páginasHealthcare Karthik R IIM Indoresudhirnair100% (2)
- River Pollution Gyanesh Sinha FMSDocumento10 páginasRiver Pollution Gyanesh Sinha FMSsudhirnairAinda não há avaliações
- Irrigation Priyank Tiwari IIM IndoreDocumento10 páginasIrrigation Priyank Tiwari IIM IndoresudhirnairAinda não há avaliações
- Education Pradipta Banerjee XLRIDocumento10 páginasEducation Pradipta Banerjee XLRIsudhirnairAinda não há avaliações
- Higher Education - Pankaj Mishra - IIM LucknowDocumento10 páginasHigher Education - Pankaj Mishra - IIM LucknowsudhirnairAinda não há avaliações
- Irrigation Muthu An K TAPMIDocumento10 páginasIrrigation Muthu An K TAPMIsudhirnairAinda não há avaliações
- Irrigation Anjan Ash IIM ShillongDocumento10 páginasIrrigation Anjan Ash IIM ShillongsudhirnairAinda não há avaliações
- Higher Education Shruti Tewari XLRIDocumento10 páginasHigher Education Shruti Tewari XLRIsudhirnairAinda não há avaliações
- Healthcare - Pratyush Sinha Ahwan - IIM LucknowDocumento10 páginasHealthcare - Pratyush Sinha Ahwan - IIM LucknowsudhirnairAinda não há avaliações
- Education Kumar Gaurav IIM IndoreDocumento11 páginasEducation Kumar Gaurav IIM IndoresudhirnairAinda não há avaliações
- Healthcare Ankita XLRIDocumento10 páginasHealthcare Ankita XLRIsudhirnairAinda não há avaliações
- Higher Education Shruti Tewari XLRIDocumento10 páginasHigher Education Shruti Tewari XLRIsudhirnairAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Vacancy Annoucement NPWIC IIDocumento8 páginasVacancy Annoucement NPWIC IIGuull RukhAinda não há avaliações
- Permutations OnlyDocumento26 páginasPermutations OnlyazuraanasAinda não há avaliações
- Tkinter GUI Programming by ExampleDocumento374 páginasTkinter GUI Programming by ExampleArphan Desoja100% (5)
- Jamb English 1984Documento6 páginasJamb English 1984ademoladaniella865Ainda não há avaliações
- Micros 3700Documento498 páginasMicros 3700Nikie5100% (2)
- 01 Intro ERP Using GBI SAP Slides v2.01Documento14 páginas01 Intro ERP Using GBI SAP Slides v2.01Nikola SvilarAinda não há avaliações
- Implementing Ipv6 in The Enterprise Network: CCNP Route: Implementing Ip RoutingDocumento109 páginasImplementing Ipv6 in The Enterprise Network: CCNP Route: Implementing Ip RoutingMed ArefAinda não há avaliações
- DIGISOL Wireless Router SettingsDocumento2 páginasDIGISOL Wireless Router SettingsAvinash DubeyAinda não há avaliações
- Progression of Noel GallagherDocumento7 páginasProgression of Noel Gallagherfady_philip1201Ainda não há avaliações
- Chapter Real Project MiDocumento72 páginasChapter Real Project Mimayowa alexAinda não há avaliações
- Download: Eating For BeautyDocumento2 páginasDownload: Eating For BeautyJevimer Lobitana100% (1)
- Philosophy and Ecosystem: Towards A Transcendental EcologyDocumento20 páginasPhilosophy and Ecosystem: Towards A Transcendental EcologyAnthonyPaulSmithAinda não há avaliações
- Theory of Knowledge NotesDocumento9 páginasTheory of Knowledge NotesBIMO5 SawarthiaAinda não há avaliações
- Distocia de Dinamica enDocumento28 páginasDistocia de Dinamica enRaluca HabaAinda não há avaliações
- The Xia DynastyDocumento7 páginasThe Xia Dynastyapi-328198337Ainda não há avaliações
- Air Flow CalculationDocumento27 páginasAir Flow CalculationvisanuAinda não há avaliações
- KL1002 - 2-Channel Digital Input Terminal 24 V DC: Product InformationDocumento2 páginasKL1002 - 2-Channel Digital Input Terminal 24 V DC: Product InformationLenin ArzapaloAinda não há avaliações
- Rek Koran Bca Bulan Feb 2020Documento4 páginasRek Koran Bca Bulan Feb 2020Omar HasyadiAinda não há avaliações
- Earth Science Quiz on Seasons, Movements and StructureDocumento4 páginasEarth Science Quiz on Seasons, Movements and StructureRBS RISSAinda não há avaliações
- Aaa & Radius Configuration Issue1Documento26 páginasAaa & Radius Configuration Issue1api-3758431Ainda não há avaliações
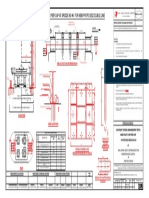
- Ohe Mast Fixing Arrangement On Pier Cap at Bridge No:46 For New Proposed Double LineDocumento1 páginaOhe Mast Fixing Arrangement On Pier Cap at Bridge No:46 For New Proposed Double LineRVNLPKG6B VBL-GTLMAinda não há avaliações
- 20 Multiple Choice BiodieselDocumento4 páginas20 Multiple Choice BiodieselNguyen KhoaAinda não há avaliações
- Journey of World Music Instruments ComDocumento3 páginasJourney of World Music Instruments ComSomesh PainuliAinda não há avaliações
- CK25/27/30/35 Tractor Workshop ManualDocumento402 páginasCK25/27/30/35 Tractor Workshop ManualFrançois Charrière100% (2)
- Chemical Food Safety PDFDocumento296 páginasChemical Food Safety PDFgoudhamAinda não há avaliações
- Manufacturing Engineering and Material Processing - 73 Handbook of Lapping and PolishingDocumento16 páginasManufacturing Engineering and Material Processing - 73 Handbook of Lapping and Polishingrsmith456100% (2)
- Gcu Clinical Eval 3Documento12 páginasGcu Clinical Eval 3api-296214965Ainda não há avaliações
- 4.BS3171 - Physics and Chemistry PDFDocumento2 páginas4.BS3171 - Physics and Chemistry PDFVijayarasu TAinda não há avaliações
- Gujarat Technological University: Subject Code: Date:01/01/2019 Subject Name: Time: 10:30 AM To 01:30 PM Total Marks: 70Documento3 páginasGujarat Technological University: Subject Code: Date:01/01/2019 Subject Name: Time: 10:30 AM To 01:30 PM Total Marks: 70harold_gravity9885Ainda não há avaliações