Você também pode gostar
- Study Model / Orthodontic Courses by Indian Dental AcademyDocumento134 páginasStudy Model / Orthodontic Courses by Indian Dental Academyindian dental academy100% (5)
- Sterilization of Ortho Instruments / Orthodontic Courses by Indian Dental AcademyDocumento57 páginasSterilization of Ortho Instruments / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Vit and Hormone in Relation To Growth and Development / Orthodontic Courses by Indian Dental AcademyDocumento38 páginasVit and Hormone in Relation To Growth and Development / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Saliva / Orthodontic Courses by Indian Dental AcademyDocumento191 páginasSaliva / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Soft Tissus Ceph Analysis / Orthodontic Courses by Indian Dental AcademyDocumento155 páginasSoft Tissus Ceph Analysis / Orthodontic Courses by Indian Dental Academyindian dental academy100% (1)
- The Roth Prescription / Orthodontic Courses by Indian Dental AcademyDocumento85 páginasThe Roth Prescription / Orthodontic Courses by Indian Dental Academyindian dental academy100% (2)
- Ss Wire Properties / Orthodontic Courses by Indian Dental AcademyDocumento79 páginasSs Wire Properties / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Radiology in Orthodontics-Dr - Kavitha / Orthodontic Courses by Indian Dental AcademyDocumento85 páginasRadiology in Orthodontics-Dr - Kavitha / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Space Closure3 / Orthodontic Courses by Indian Dental AcademyDocumento51 páginasSpace Closure3 / Orthodontic Courses by Indian Dental Academyindian dental academy100% (4)
- Rapid Molar Intrusion Device / Orthodontic Courses by Indian Dental AcademyDocumento55 páginasRapid Molar Intrusion Device / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Pre-Natal and Post-Natal Development of Maxilla Part 4 / Orthodontic Courses by Indian Dental AcademyDocumento76 páginasPre-Natal and Post-Natal Development of Maxilla Part 4 / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Role of Drugs in Orthodontics / Orthodontic Courses by Indian Dental AcademyDocumento239 páginasRole of Drugs in Orthodontics / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Roth's Prescription / Orthodontic Courses by Indian Dental AcademyDocumento64 páginasRoth's Prescription / Orthodontic Courses by Indian Dental Academyindian dental academy100% (1)
- Root Movement in Orthodontics / Orthodontic Courses by Indian Dental AcademyDocumento93 páginasRoot Movement in Orthodontics / Orthodontic Courses by Indian Dental Academyindian dental academy83% (6)
- Obstructive Sleep Apnea - Dr.M.M.varadharaja / Orthodontic Courses by Indian Dental AcademyDocumento168 páginasObstructive Sleep Apnea - Dr.M.M.varadharaja / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Orthodontic Brackets / Orthodontic Courses by Indian Dental AcademyDocumento102 páginasOrthodontic Brackets / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Orthodontic Adhesives / Orthodontic Courses by Indian Dental AcademyDocumento137 páginasOrthodontic Adhesives / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Pre-Natal and Post-Natal Development of Maxilla Part 2 / Orthodontic Courses by Indian Dental AcademyDocumento72 páginasPre-Natal and Post-Natal Development of Maxilla Part 2 / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Molecular Basis PART 1 / Orthodontic Courses by Indian Dental AcademyDocumento188 páginasMolecular Basis PART 1 / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Orthodontic Wires - Properties / Orthodontic Courses by Indian Dental AcademyDocumento226 páginasOrthodontic Wires - Properties / Orthodontic Courses by Indian Dental Academyindian dental academy100% (1)
- MAA Final / Orthodontic Courses by Indian Dental AcademyDocumento93 páginasMAA Final / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Periodontal Changes in Ortho Treatment / Orthodontic Courses by Indian Dental AcademyDocumento81 páginasPeriodontal Changes in Ortho Treatment / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Implants and Anchorage / Orthodontic Courses by Indian Dental AcademyDocumento52 páginasImplants and Anchorage / Orthodontic Courses by Indian Dental Academyindian dental academy100% (1)
- Mandibular Growth Rotation (2) / Orthodontic Courses by Indian Dental AcademyDocumento28 páginasMandibular Growth Rotation (2) / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Lasers and Its Role in Endodontics / Orthodontic Courses by Indian Dental AcademyDocumento73 páginasLasers and Its Role in Endodontics / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Indices / Orthodontic Courses by Indian Dental AcademyDocumento77 páginasIndices / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Methods of Gaining Space. / Orthodontic Courses by Indian Dental AcademyDocumento70 páginasMethods of Gaining Space. / Orthodontic Courses by Indian Dental Academyindian dental academy100% (2)
- Materials in Orthodontics / Orthodontic Courses by Indian Dental AcademyDocumento124 páginasMaterials in Orthodontics / Orthodontic Courses by Indian Dental Academyindian dental academy100% (2)
- Interceptive Orthodontics 1 / Orthodontic Courses by Indian Dental AcademyDocumento44 páginasInterceptive Orthodontics 1 / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Hybrid Functional Appliance / Orthodontic Courses by Indian Dental AcademyDocumento127 páginasHybrid Functional Appliance / Orthodontic Courses by Indian Dental Academyindian dental academy100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Occupational Health Saftey Management Plan (OHMSP) - NZDocumento29 páginasOccupational Health Saftey Management Plan (OHMSP) - NZRam P0% (1)
- PES5 Manual PDFDocumento44 páginasPES5 Manual PDFaldo riojaAinda não há avaliações
- Adaptable Polarity: Movement, Muscles & Meridians Lateral Line of Fascia & Gallbladder ChannelDocumento98 páginasAdaptable Polarity: Movement, Muscles & Meridians Lateral Line of Fascia & Gallbladder ChannelAngel RuelasAinda não há avaliações
- Chapter 2 - Safe Work Procedure / Risk Assessment: Service ManualDocumento70 páginasChapter 2 - Safe Work Procedure / Risk Assessment: Service Manualjacklyn ade putra100% (1)
- DRM Tool For StudentsDocumento6 páginasDRM Tool For StudentsTricia PrestozaAinda não há avaliações
- ACUTE PAIN - (June 25, 2019) Assessment Nursing Diagnosis Planning Intervention Rationally EvaluationDocumento4 páginasACUTE PAIN - (June 25, 2019) Assessment Nursing Diagnosis Planning Intervention Rationally EvaluationkingpinAinda não há avaliações
- July Free Chapter - Perfect by Rachel JoyceDocumento21 páginasJuly Free Chapter - Perfect by Rachel JoyceRandomHouseAUAinda não há avaliações
- 《إيكو تخطيط الرأس و الدماغ》Documento75 páginas《إيكو تخطيط الرأس و الدماغ》D. GadahAinda não há avaliações
- Swimming at Night by Lucy ClarkeDocumento22 páginasSwimming at Night by Lucy ClarkeSimon and Schuster100% (1)
- Ganglion Cyst OverviewDocumento5 páginasGanglion Cyst OverviewVya MignonetteAinda não há avaliações
- Presentasi Kasus Ujian Bedah Plastik DR Amru Sungkar SPB SpBE - Nadiya Nur G991903042 - September 2019Documento30 páginasPresentasi Kasus Ujian Bedah Plastik DR Amru Sungkar SPB SpBE - Nadiya Nur G991903042 - September 2019Akmalia FatimahAinda não há avaliações
- Kelli Smith Edt 321 Resume UpdateDocumento2 páginasKelli Smith Edt 321 Resume Updateapi-283093639Ainda não há avaliações
- Inflammation and Wound HealingDocumento3 páginasInflammation and Wound HealingPrincess AgarwalAinda não há avaliações
- Anterior Abdominal WallDocumento43 páginasAnterior Abdominal WallDrravikumar BhandariAinda não há avaliações
- Clippard THNTD Instruction Sheet.Documento2 páginasClippard THNTD Instruction Sheet.John Melanathy IIAinda não há avaliações
- Answered - Muscular System Lab Project 04 12 2022Documento17 páginasAnswered - Muscular System Lab Project 04 12 2022NDINDA GODYFREEY NATTOHAinda não há avaliações
- Funny Medical TermsDocumento17 páginasFunny Medical Termswadhe omara100% (1)
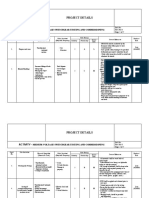
- Risk Assessment Switchgear Testing CommissioningDocumento7 páginasRisk Assessment Switchgear Testing Commissioningaaktgt Mep100% (1)
- Nikhil Ola Tort ProjectDocumento18 páginasNikhil Ola Tort Projectnikhil olaAinda não há avaliações
- Medial Collateral Ligament Injury MCL Rehabilitation Yale 240271 28716Documento8 páginasMedial Collateral Ligament Injury MCL Rehabilitation Yale 240271 28716Raluca Alexandra PlescaAinda não há avaliações
- Homeless Mortality Health Commission Background Reading 20180219Documento28 páginasHomeless Mortality Health Commission Background Reading 20180219auweia1Ainda não há avaliações
- Procedures Used in The Management of DystociaDocumento17 páginasProcedures Used in The Management of DystociaRavi RokkamAinda não há avaliações
- PCRC Conc Lintels For Structural SupportsDocumento24 páginasPCRC Conc Lintels For Structural SupportsZaky MessengerAinda não há avaliações
- Voice Exercises Training CenterDocumento25 páginasVoice Exercises Training CenterFilipe Rovarotto100% (5)
- Hypertrophic Scar & KeloidDocumento3 páginasHypertrophic Scar & KeloidVeroshini TeddyAinda não há avaliações
- John Carlton Power Words Special Report PDFDocumento22 páginasJohn Carlton Power Words Special Report PDFelena alinaAinda não há avaliações
- Asra Fellow Knowledge Test q4 Questions OnlyDocumento4 páginasAsra Fellow Knowledge Test q4 Questions OnlyZohaib ZafarAinda não há avaliações
- Ship Compartmentation and Watertight IntegrityDocumento26 páginasShip Compartmentation and Watertight IntegrityAvinash RaoAinda não há avaliações
- Msds K2cro4 PDFDocumento6 páginasMsds K2cro4 PDFAnonymous U0RczPAinda não há avaliações
- Return To Running Program Steve Cole WM MaryDocumento6 páginasReturn To Running Program Steve Cole WM Marygb tradeAinda não há avaliações