Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Evaluate Instructional Materials ToolDocumento3 páginasEvaluate Instructional Materials ToolDanna Mae Terse Yuzon92% (12)
- Conscious BusinessDocumento19 páginasConscious BusinessparadescartarAinda não há avaliações
- TricycleDocumento10 páginasTricyclechancer01Ainda não há avaliações
- Legal Translation and Bilingual Law Drafting in Hong Kong - Challenges and Interactions in Chinese RegionsDocumento172 páginasLegal Translation and Bilingual Law Drafting in Hong Kong - Challenges and Interactions in Chinese RegionsPui Gwen YeungAinda não há avaliações
- Arc AnimalDocumento1 páginaArc AnimalRohayati A SidekAinda não há avaliações
- Prospect Vaccin Euvax BDocumento3 páginasProspect Vaccin Euvax BlujihaneAinda não há avaliações
- Matlab Course For CHEDocumento95 páginasMatlab Course For CHEAbdullah SalemAinda não há avaliações
- DiverseDocumento200 páginasDiverselujihaneAinda não há avaliações
- Abstract VII 4Documento2 páginasAbstract VII 4lujihaneAinda não há avaliações
- Baculovirus VectorDocumento3 páginasBaculovirus VectoryigitilgazAinda não há avaliações
- Recombinant DNA Has Opened New Horizons in MedicineDocumento2 páginasRecombinant DNA Has Opened New Horizons in MedicinelujihaneAinda não há avaliações
- Recombinant DNA Has Opened New Horizons in MedicineDocumento1 páginaRecombinant DNA Has Opened New Horizons in MedicinelujihaneAinda não há avaliações
- Vaccines: Properties of Ideal VaccineDocumento5 páginasVaccines: Properties of Ideal VaccinelujihaneAinda não há avaliações
- DocumentatieDocumento7 páginasDocumentatielujihaneAinda não há avaliações
- Felicia Ratnaraj - 2013Documento1 páginaFelicia Ratnaraj - 2013lujihaneAinda não há avaliações
- Comparison Prior and Post Vaccination of Inactivated Recombinant Vaccine Against Mannheimiosis in Boer Goats Farm in Sabah 2157 7560.1000173Documento4 páginasComparison Prior and Post Vaccination of Inactivated Recombinant Vaccine Against Mannheimiosis in Boer Goats Farm in Sabah 2157 7560.1000173lujihaneAinda não há avaliações
- DocumentatieDocumento8 páginasDocumentatielujihaneAinda não há avaliações
- Full TextDocumento17 páginasFull TextlujihaneAinda não há avaliações
- Abstract VII 4Documento2 páginasAbstract VII 4lujihaneAinda não há avaliações
- E ChoralDocumento1 páginaE ChorallujihaneAinda não há avaliações
- RecombinationDocumento4 páginasRecombinationlujihaneAinda não há avaliações
- CAST Vaccine Development Issue Paper FINAL REV153Documento12 páginasCAST Vaccine Development Issue Paper FINAL REV153borzaflorinaAinda não há avaliações
- Colistin and Polymyxin BDocumento15 páginasColistin and Polymyxin Blujihane100% (1)
- NMR-1 BasicDocumento52 páginasNMR-1 Basicamit086Ainda não há avaliações
- A Recombiant E. Coli VaccineDocumento9 páginasA Recombiant E. Coli VaccinelujihaneAinda não há avaliações
- WWW - Scert.goa - Gov.in: ST THDocumento2 páginasWWW - Scert.goa - Gov.in: ST THWayne GonsalvesAinda não há avaliações
- Marketing Process: Analysis of The Opportunities in The MarketDocumento2 páginasMarketing Process: Analysis of The Opportunities in The MarketCristine Joy AsduloAinda não há avaliações
- Bahir Dar University School of Civil and Water Resource EngineeringDocumento40 páginasBahir Dar University School of Civil and Water Resource EngineeringMichael AssefaAinda não há avaliações
- Type I and Type II ErrorsDocumento8 páginasType I and Type II ErrorsL'Homme Révolté100% (1)
- Overview of The Development and Mission Application of The Advanced Electric Propulsion System (AEPS)Documento24 páginasOverview of The Development and Mission Application of The Advanced Electric Propulsion System (AEPS)SOURAV GHIMIREYAinda não há avaliações
- Theoryand Paradigmin Social ResearchDocumento18 páginasTheoryand Paradigmin Social ResearchZeline ZephyreAinda não há avaliações
- Ule M. Dela Cruz (DATE/ May 30 2022)Documento25 páginasUle M. Dela Cruz (DATE/ May 30 2022)Ule De La CruzAinda não há avaliações
- Investigating Construction in The Greek AEC IndustryDocumento72 páginasInvestigating Construction in The Greek AEC IndustryAjvaro ContiAinda não há avaliações
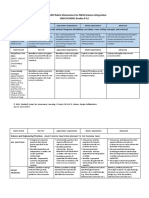
- Ngss Science Integration LDC 9-12 Rubric-3Documento6 páginasNgss Science Integration LDC 9-12 Rubric-3api-318937942Ainda não há avaliações
- Highway Engineering (15Cv63) As Per Choice Based Credit System (CBCS) SchemeDocumento31 páginasHighway Engineering (15Cv63) As Per Choice Based Credit System (CBCS) SchemeRicky MeyerAinda não há avaliações
- Croatian Noble Kindred History BookDocumento3 páginasCroatian Noble Kindred History BookAnonymous PXFOfWAinda não há avaliações
- Religious Attendance, Spirituality, and Major Depression in Canada: A14-Year Follow-Up StudyDocumento9 páginasReligious Attendance, Spirituality, and Major Depression in Canada: A14-Year Follow-Up StudyCatarina C.Ainda não há avaliações
- 12 Ac December 01-31 2019 by @naukriaspirant PDFDocumento442 páginas12 Ac December 01-31 2019 by @naukriaspirant PDFAmit PrasadAinda não há avaliações
- UNICEF WASH Officer Job ProfileDocumento5 páginasUNICEF WASH Officer Job ProfileazizrbgAinda não há avaliações
- Worksheet 8 - Interview QuestionsDocumento4 páginasWorksheet 8 - Interview QuestionsAR_writing_samplesAinda não há avaliações
- A Critical Review of The Scientist Practitioner Model For Counselling PsychologyDocumento13 páginasA Critical Review of The Scientist Practitioner Model For Counselling PsychologySanja DjordjevicAinda não há avaliações
- Session 1 StudentDocumento44 páginasSession 1 StudentYongQing OngAinda não há avaliações
- BE Guidelines For Ethical LeadershipDocumento2 páginasBE Guidelines For Ethical Leadershipits4krishna3776Ainda não há avaliações
- Sucrose Gradient Separation ProtocolDocumento16 páginasSucrose Gradient Separation ProtocolBalaAinda não há avaliações
- Aiaa 2009 1164Documento15 páginasAiaa 2009 1164Michele GiulianiAinda não há avaliações
- Seven Elements For Capacity Development For Disaster Risk ReductionDocumento4 páginasSeven Elements For Capacity Development For Disaster Risk ReductionPer BeckerAinda não há avaliações
- ACFrOgAlSbXHol7X5DCh7AxhfktcUDPYrfN3azOCdL8n w0uIfRwG5eExpx5o5M39eBr6flbL4jKbJQr5lHThcZBkyXMxp-ToA0tTBR4-0kpI 0Pvs52jZmo JZy6vTDinXL3OiGxJSHKeOq WwoDocumento290 páginasACFrOgAlSbXHol7X5DCh7AxhfktcUDPYrfN3azOCdL8n w0uIfRwG5eExpx5o5M39eBr6flbL4jKbJQr5lHThcZBkyXMxp-ToA0tTBR4-0kpI 0Pvs52jZmo JZy6vTDinXL3OiGxJSHKeOq WwoAhmad AbdAinda não há avaliações
- Susan Abed (2012) - Corporate Governance and Earnings Management Jordanian EvidenceDocumento10 páginasSusan Abed (2012) - Corporate Governance and Earnings Management Jordanian Evidenceheryp123Ainda não há avaliações
- Scan SamplingDocumento3 páginasScan Samplingrehan ul haq100% (1)
- Sociology: Tension Between Science and Militant Activism?: Sandro SerpaDocumento8 páginasSociology: Tension Between Science and Militant Activism?: Sandro SerpaHamza ButtAinda não há avaliações
- Traumacare 02 00043Documento12 páginasTraumacare 02 00043Muhammad Nur Ardhi LahabuAinda não há avaliações