Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- ER Nurse ChecklistDocumento3 páginasER Nurse Checklistdocpanchu100% (1)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- M SC Nursing Question Previous Year Paper For RS4Documento10 páginasM SC Nursing Question Previous Year Paper For RS4Vantrigaru Veeresh Bangi100% (4)
- Vitamin D and Bone DiseaseDocumento6 páginasVitamin D and Bone DiseasedocpanchuAinda não há avaliações
- Endogenous Versus Exogenous Growth Factor RegulationDocumento7 páginasEndogenous Versus Exogenous Growth Factor RegulationdocpanchuAinda não há avaliações
- Adult Measures of General Health PDFDocumento30 páginasAdult Measures of General Health PDFdocpanchuAinda não há avaliações
- Current Indications and Outcomes of Total Wrist ArthroplastyDocumento9 páginasCurrent Indications and Outcomes of Total Wrist ArthroplastydocpanchuAinda não há avaliações
- How To Interpret Plain Radiographs in Clinical PracticeDocumento21 páginasHow To Interpret Plain Radiographs in Clinical PracticedocpanchuAinda não há avaliações
- Top 10 Orthopaedic CompaniesDocumento23 páginasTop 10 Orthopaedic CompaniesdocpanchuAinda não há avaliações
- Hip Injuries in Young AthletesDocumento10 páginasHip Injuries in Young AthletesdocpanchuAinda não há avaliações
- Can You Believe What You ReadDocumento3 páginasCan You Believe What You ReaddocpanchuAinda não há avaliações
- Hinduism in South Africa PDFDocumento15 páginasHinduism in South Africa PDFdocpanchuAinda não há avaliações
- Litigation After Hip and Knee ReplacementDocumento5 páginasLitigation After Hip and Knee ReplacementdocpanchuAinda não há avaliações
- Biomarkers in OsteoarthritisDocumento5 páginasBiomarkers in OsteoarthritisdocpanchuAinda não há avaliações
- A Current Review of Molecular Mechanisms Regarding Osteoarthritis and Pain PDFDocumento8 páginasA Current Review of Molecular Mechanisms Regarding Osteoarthritis and Pain PDFdocpanchuAinda não há avaliações
- Adult Measures of General HealthDocumento30 páginasAdult Measures of General HealthdocpanchuAinda não há avaliações
- Lumbar Fusion BrochureDocumento2 páginasLumbar Fusion BrochuredocpanchuAinda não há avaliações
- Charge Nurse ResponsibilitiesDocumento4 páginasCharge Nurse ResponsibilitiesdocpanchuAinda não há avaliações
- A Current Review of Molecular Mechanisms Regarding Osteoarthritis and PainDocumento8 páginasA Current Review of Molecular Mechanisms Regarding Osteoarthritis and PaindocpanchuAinda não há avaliações
- 2 Operating Theatres HCADocumento6 páginas2 Operating Theatres HCAdocpanchuAinda não há avaliações
- Trauma Brochure (English)Documento2 páginasTrauma Brochure (English)docpanchuAinda não há avaliações
- Casts & Splints WhoDocumento4 páginasCasts & Splints WhodocpanchuAinda não há avaliações
- Anabolic Agents and Bone QualityDocumento10 páginasAnabolic Agents and Bone QualitydocpanchuAinda não há avaliações
- Hip Knee BookletDocumento24 páginasHip Knee BookletdocpanchuAinda não há avaliações
- Lumbar Laminectomy BrochureDocumento2 páginasLumbar Laminectomy BrochuredocpanchuAinda não há avaliações
- Trauma Service and Department BrochureDocumento4 páginasTrauma Service and Department BrochuredocpanchuAinda não há avaliações
- Back CommandmentsDocumento4 páginasBack CommandmentsdocpanchuAinda não há avaliações
- Arthritis and Joint ReplacementDocumento35 páginasArthritis and Joint ReplacementdocpanchuAinda não há avaliações
- Hip Knee BookletDocumento24 páginasHip Knee BookletdocpanchuAinda não há avaliações
- A Model For Co-Management 4-19-2011Documento39 páginasA Model For Co-Management 4-19-2011docpanchuAinda não há avaliações
- Review of EboDocumento7 páginasReview of EbodocpanchuAinda não há avaliações
- Resuscitative ThoracotomyDocumento7 páginasResuscitative ThoracotomyRobert ChristevenAinda não há avaliações
- ABPS 500: Examination BlueprintsDocumento16 páginasABPS 500: Examination BlueprintsGene ChoiAinda não há avaliações
- 2010 BasicDocumento536 páginas2010 Basicskypilot1433Ainda não há avaliações
- 2 Thrombosed HemorrhoidsDocumento5 páginas2 Thrombosed HemorrhoidsMarko LovrićAinda não há avaliações
- CV JafDocumento3 páginasCV JaffreannAinda não há avaliações
- Discharge Plan LatestDocumento4 páginasDischarge Plan LatestBESA JERIC FLORESAinda não há avaliações
- Beldner 2020Documento10 páginasBeldner 2020Salsabila HMAinda não há avaliações
- Product Price List 2021Documento64 páginasProduct Price List 2021hariAinda não há avaliações
- Doctors Time Table MAY 2017Documento2 páginasDoctors Time Table MAY 2017Sanjy AroraAinda não há avaliações
- Analisis Penyebab Keterlambatan Mulai Operasi PertDocumento12 páginasAnalisis Penyebab Keterlambatan Mulai Operasi Pertdwi tatangAinda não há avaliações
- Lap Chole Case StudyDocumento3 páginasLap Chole Case StudyKinshuki Jain100% (1)
- BCQsDocumento9 páginasBCQsFarrukh Ali Khan0% (1)
- JTCVS Information For Authors 2019 Revised 8-16-19Documento35 páginasJTCVS Information For Authors 2019 Revised 8-16-19irmelodyAinda não há avaliações
- Chapter 2 and 1Documento31 páginasChapter 2 and 1AduAinda não há avaliações
- 3d Laparoscopic Conference Malaysia 2023Documento7 páginas3d Laparoscopic Conference Malaysia 2023Muhammad Irfanuddin IbrahimAinda não há avaliações
- Patient PositioningDocumento35 páginasPatient PositioningDajour CollinsAinda não há avaliações
- Fernandez-Vega Eye InstituteDocumento16 páginasFernandez-Vega Eye InstituteFabricio Eric ParraAinda não há avaliações
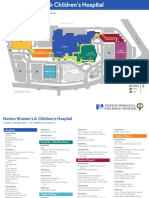
- NWCH Campus Map 1Documento2 páginasNWCH Campus Map 1Sara DiabAinda não há avaliações
- Your Arthroscopic Shoulder Surgery,: A Helpful GuideDocumento12 páginasYour Arthroscopic Shoulder Surgery,: A Helpful GuideAle XyyAinda não há avaliações
- Lista de Precios Arthrex Consumibles 2022Documento32 páginasLista de Precios Arthrex Consumibles 2022Gerardo OlagueAinda não há avaliações
- Green Light Surgical GuideDocumento88 páginasGreen Light Surgical GuidekbrinaldiAinda não há avaliações
- Allograft Vs Autograft 2022Documento11 páginasAllograft Vs Autograft 2022Ahmed MortadaAinda não há avaliações
- NSW Surgical PlumDocumento20 páginasNSW Surgical PlumTheodora DolianitisAinda não há avaliações
- Editorial - 2008 - Operative Techniques in General Surgery PDFDocumento1 páginaEditorial - 2008 - Operative Techniques in General Surgery PDFMaykon PereiraAinda não há avaliações
- Jaw Surgery Singapore - TES ClinicDocumento9 páginasJaw Surgery Singapore - TES ClinicV Line Face - TES Clinic SingaporeAinda não há avaliações
- Postoperative Paralytic IleusDocumento9 páginasPostoperative Paralytic IleusazisaaiAinda não há avaliações
- What Is Community Health?: Art. 25 Sec. 1Documento17 páginasWhat Is Community Health?: Art. 25 Sec. 1Yuuki Chitose (tai-kun)Ainda não há avaliações
- 1647-Article Text-3369-1-10-20220320Documento5 páginas1647-Article Text-3369-1-10-20220320Eshan BhaleraoAinda não há avaliações
- Policy On Management of The Frenulum inDocumento6 páginasPolicy On Management of The Frenulum inمعتزباللهAinda não há avaliações