Você também pode gostar
- Hipotensi Orthostatik NeurogenikDocumento8 páginasHipotensi Orthostatik NeurogenikayuniputriAinda não há avaliações
- Mechanisms, Causes, and Evaluation of Orthostatic Hypotension - UpToDateDocumento20 páginasMechanisms, Causes, and Evaluation of Orthostatic Hypotension - UpToDateCipriano Di MauroAinda não há avaliações
- A Review of The Etiology, Asssociated Comorbidities, andDocumento13 páginasA Review of The Etiology, Asssociated Comorbidities, andFrancis RomanosAinda não há avaliações
- Hipotensi PDFDocumento6 páginasHipotensi PDFimahAinda não há avaliações
- PRIN PBL Week 11 Tutorial 1Documento3 páginasPRIN PBL Week 11 Tutorial 1jonx225Ainda não há avaliações
- Pathophysiology of Heart FailureDocumento2 páginasPathophysiology of Heart Failurewayanesa9Ainda não há avaliações
- АГ, атеросклероз удDocumento74 páginasАГ, атеросклероз удsoumyajitchakraborty0238Ainda não há avaliações
- Hypertensive Encephalopathy: Presentation DDX Workup Treatment MedicationDocumento8 páginasHypertensive Encephalopathy: Presentation DDX Workup Treatment MedicationMoh SuriyawalAinda não há avaliações
- Pathophysiology Diagnosis and Treatment of Orthostatic Hypotension and Vasovagal Syncope1Documento17 páginasPathophysiology Diagnosis and Treatment of Orthostatic Hypotension and Vasovagal Syncope1Idha AAinda não há avaliações
- Neurohormonal Hypothesis in Heart FailureDocumento11 páginasNeurohormonal Hypothesis in Heart FailureCypress Trixia Mananquil MacapagalAinda não há avaliações
- Cardiovascular Autonomic Dysfunction in Parkinson's DiseaseDocumento7 páginasCardiovascular Autonomic Dysfunction in Parkinson's DiseaseCocosul Cocosului CocosaruluiAinda não há avaliações
- CH27 FinalDocumento8 páginasCH27 FinalDiogoBeirãoAinda não há avaliações
- Cardiovascular Dysfunction in Spinal Cord DisordersDocumento12 páginasCardiovascular Dysfunction in Spinal Cord DisordersGerardo SilvaAinda não há avaliações
- Disautonomia en Adulto Mayor 2018Documento13 páginasDisautonomia en Adulto Mayor 2018Carlos BucaraAinda não há avaliações
- Heart Failure Pathophysiology ExplainedDocumento42 páginasHeart Failure Pathophysiology ExplainedParsa EbrahimpourAinda não há avaliações
- POTS Current Concepts Trends in CVMDocumento5 páginasPOTS Current Concepts Trends in CVMmperlethAinda não há avaliações
- J Neurol Neurosurg Psychiatry 2013 Asahina 674 80Documento8 páginasJ Neurol Neurosurg Psychiatry 2013 Asahina 674 80doraemonraniAinda não há avaliações
- Congestive Heart Failure: Diagnosis, Pathophysiology, Therapy, and Implications For Respiratory CareDocumento10 páginasCongestive Heart Failure: Diagnosis, Pathophysiology, Therapy, and Implications For Respiratory CareKevinDilianSugandaAinda não há avaliações
- Malignant Hypertension: Hypertensive EmergenciesDocumento7 páginasMalignant Hypertension: Hypertensive EmergenciesAbdul QuyyumAinda não há avaliações
- Peer Review Process: Author: Section Editor: Deputy EditorDocumento14 páginasPeer Review Process: Author: Section Editor: Deputy EditorLuis Enrique Caceres AlavrezAinda não há avaliações
- Is Postural Orthostatic Tachycardia Syndrome (POTS) A Central Nervous System Disorder?Documento8 páginasIs Postural Orthostatic Tachycardia Syndrome (POTS) A Central Nervous System Disorder?LinaConejomutanterosaAinda não há avaliações
- Treatment OptionsDocumento17 páginasTreatment OptionsAnonymous bbeAZHxZAinda não há avaliações
- Inappropriate Sinus TachycardiaDocumento23 páginasInappropriate Sinus TachycardiaOnon EssayedAinda não há avaliações
- Neurologic Manifestations of Hyperthyroidism and GravesDocumento3 páginasNeurologic Manifestations of Hyperthyroidism and GravesAde YonataAinda não há avaliações
- Medical Guide to Postural Tachycardia Syndrome (PoTSDocumento12 páginasMedical Guide to Postural Tachycardia Syndrome (PoTSAttis PhrygiaAinda não há avaliações
- Diff DS AH - Eh. TreatmentDocumento80 páginasDiff DS AH - Eh. TreatmentCastleKGAinda não há avaliações
- Abnormalities of Angiotensin Regulation in PotsDocumento14 páginasAbnormalities of Angiotensin Regulation in Potsiri_balAinda não há avaliações
- MJMHS 0626Documento7 páginasMJMHS 0626lilydariniAinda não há avaliações
- Jurnal FisioDocumento8 páginasJurnal Fisiorizkya amanahAinda não há avaliações
- 4ea7cdc044aebf27f87d94a2 PDFDocumento7 páginas4ea7cdc044aebf27f87d94a2 PDFTaufiqur Rohman ChimeraAinda não há avaliações
- Pharmacotherapy of Heart FailureDocumento17 páginasPharmacotherapy of Heart FailurelisaAinda não há avaliações
- Signs and SymptomsDocumento16 páginasSigns and SymptomsRose AnnAinda não há avaliações
- Syncope - Electrocardiographic and Clinical CorrelationDocumento16 páginasSyncope - Electrocardiographic and Clinical CorrelationNANDY LUZ FERIA DIAZAinda não há avaliações
- Heart Failure - AhaDocumento77 páginasHeart Failure - AhaChendy Endriansa100% (1)
- How To Manage A Patient With OrthostaticDocumento18 páginasHow To Manage A Patient With OrthostaticReza Oktarizal100% (2)
- 1-s2.0-S003537872301144X-mainDocumento12 páginas1-s2.0-S003537872301144X-mainSergioAinda não há avaliações
- The Effect of Cilostazol On Right Heart FunctionDocumento43 páginasThe Effect of Cilostazol On Right Heart FunctionGunawan YogaAinda não há avaliações
- Parkinson's & Movement Disorders-Harrison's NeurologyDocumento23 páginasParkinson's & Movement Disorders-Harrison's Neurologyindia2puppyAinda não há avaliações
- Neuromodulation in Treatment of Hypertension by Acupuncture: A Neurophysiological ProspectiveDocumento8 páginasNeuromodulation in Treatment of Hypertension by Acupuncture: A Neurophysiological Prospectivewillv4Ainda não há avaliações
- Molecular Neurobiology of DepressionDocumento9 páginasMolecular Neurobiology of DepressionFlyefs AttikosAinda não há avaliações
- Materi English 1Documento11 páginasMateri English 1WINARDIAinda não há avaliações
- Stupor and Coma in Adults: Author: Section Editors: Deputy EditorDocumento30 páginasStupor and Coma in Adults: Author: Section Editors: Deputy EditorYessenia BarrantesAinda não há avaliações
- Role of Sleep-Wake Cycle On Blood Pressure Circadian Rhythms and HypertensionDocumento13 páginasRole of Sleep-Wake Cycle On Blood Pressure Circadian Rhythms and HypertensionFarah AhmadAinda não há avaliações
- Drugs Used in Heart Failure: Pharmacology (2) PHAR 342Documento19 páginasDrugs Used in Heart Failure: Pharmacology (2) PHAR 342Dana HamarshehAinda não há avaliações
- Peripheral Autoregulatory ComponentsDocumento2 páginasPeripheral Autoregulatory ComponentsDebbyNovriozaAinda não há avaliações
- PRES (Posterior Reversible Encephalopathy Syndrome) and Eclampsia-ReviewDocumento5 páginasPRES (Posterior Reversible Encephalopathy Syndrome) and Eclampsia-ReviewAvicena M IqbalAinda não há avaliações
- Chronic Baroreflex Activation Restores Spontaneous Baroreflex Control and Variability of Heart Rate in Obesity-Induced HypertensionDocumento10 páginasChronic Baroreflex Activation Restores Spontaneous Baroreflex Control and Variability of Heart Rate in Obesity-Induced HypertensionCaesar Catalin CaratasuAinda não há avaliações
- Fatigue: Normal and Abnormal FatigueDocumento8 páginasFatigue: Normal and Abnormal FatigueMt. ZulfiqorAinda não há avaliações
- Proyecto de Investigación Del Sistema CardiovascularDocumento3 páginasProyecto de Investigación Del Sistema CardiovascularNatalia quirogaAinda não há avaliações
- Fisiopatologia de La Falla CardiacaDocumento28 páginasFisiopatologia de La Falla CardiacaDANIELA ANDREA MARTINEZ FUENTESAinda não há avaliações
- Screen for Secondary Causes of HypertensionDocumento12 páginasScreen for Secondary Causes of HypertensionMelissaHuayapaAAinda não há avaliações
- Clinical Autonomic and Mitochondrial Disorders: Diagnosis, Prevention, and Treatment for Mind-Body WellnessNo EverandClinical Autonomic and Mitochondrial Disorders: Diagnosis, Prevention, and Treatment for Mind-Body WellnessAinda não há avaliações
- Unit 2 Heart Failure: StructureDocumento29 páginasUnit 2 Heart Failure: StructurebtaleraAinda não há avaliações
- Anti Hypertensive ThesisDocumento85 páginasAnti Hypertensive Thesiskartik369Ainda não há avaliações
- Heart Failure TodayDocumento54 páginasHeart Failure TodaypoolchagoAinda não há avaliações
- Search Termsearch Database: Limits Advanced Journal List HelpDocumento21 páginasSearch Termsearch Database: Limits Advanced Journal List Helpحسام جبار مجيدAinda não há avaliações
- The Human Sympathetic Nervous System: Its Relevance in Hypertension and Heart FailureDocumento10 páginasThe Human Sympathetic Nervous System: Its Relevance in Hypertension and Heart FailureadeAinda não há avaliações
- Uncontrolled Blood Pressure: Recognizing and Treating Hypertensive EmergenciesDocumento2 páginasUncontrolled Blood Pressure: Recognizing and Treating Hypertensive Emergenciesmhassan8154Ainda não há avaliações
- Hipertensi: A. Hypertension A.1 Definition of HypertensionDocumento12 páginasHipertensi: A. Hypertension A.1 Definition of HypertensionIrwan SyahputraAinda não há avaliações
- Pathophysiology of Heart Failure - Neurohumoral Adaptations PDFDocumento10 páginasPathophysiology of Heart Failure - Neurohumoral Adaptations PDFcristianamihailaAinda não há avaliações
- Cell Transport RevisionDocumento32 páginasCell Transport RevisionramadanAinda não há avaliações
- 6 - Hemodynamic Disorders PDFDocumento66 páginas6 - Hemodynamic Disorders PDFNogra CarlAinda não há avaliações
- Membrane Transport Mechanisms and HomeostasisDocumento29 páginasMembrane Transport Mechanisms and Homeostasisramadan100% (1)
- 357 Man 07Documento28 páginas357 Man 07ramadanAinda não há avaliações
- Ijms 15 03989Documento18 páginasIjms 15 03989ramadanAinda não há avaliações
- DR Ramadan ObjectivesDocumento3 páginasDR Ramadan ObjectivesramadanAinda não há avaliações
- 1Documento7 páginas1ramadanAinda não há avaliações
- 04a CartilageDocumento22 páginas04a CartilageramadanAinda não há avaliações
- Renal Physiology RevisionDocumento6 páginasRenal Physiology RevisionramadanAinda não há avaliações
- Endocrine QuestionsDocumento4 páginasEndocrine QuestionsramadanAinda não há avaliações
- NBME Physio QsDocumento7 páginasNBME Physio QsramadanAinda não há avaliações
- Human Anatomy: The CellDocumento33 páginasHuman Anatomy: The CellramadanAinda não há avaliações
- Preparation of The Mitochondrial FractionDocumento1 páginaPreparation of The Mitochondrial FractionramadanAinda não há avaliações
- Exercise Cardio Topic 9Documento2 páginasExercise Cardio Topic 9ramadanAinda não há avaliações
- Study of The Possible Cardioprotective Effects of Insulin, ATP, and - Arginine Against Isoproterenol-Induced Myocardial InfarctionDocumento7 páginasStudy of The Possible Cardioprotective Effects of Insulin, ATP, and - Arginine Against Isoproterenol-Induced Myocardial InfarctionramadanAinda não há avaliações
- Management of Poisoning and Drug Overdose - 2 PDFDocumento24 páginasManagement of Poisoning and Drug Overdose - 2 PDFramadanAinda não há avaliações
- Exercise Digestive Topic 2Documento6 páginasExercise Digestive Topic 2ramadan0% (1)
- Exam2 98Documento8 páginasExam2 98ramadanAinda não há avaliações
- Biochem SpecificationDocumento2 páginasBiochem SpecificationramadanAinda não há avaliações
- Changes of Ghrelin and Leptin Levels in Plasma by Cigarette Smoke in RatsDocumento8 páginasChanges of Ghrelin and Leptin Levels in Plasma by Cigarette Smoke in RatsramadanAinda não há avaliações
- 274 Renal Physiology - Part 2Documento11 páginas274 Renal Physiology - Part 2ramadanAinda não há avaliações
- Intestine Krebs-Ringer's Buffer Solution CompositionDocumento1 páginaIntestine Krebs-Ringer's Buffer Solution CompositionramadanAinda não há avaliações
- Renal PhysiologyDocumento37 páginasRenal PhysiologyramadanAinda não há avaliações
- Respiratory PhysiologyDocumento38 páginasRespiratory Physiologyramadan100% (3)
- The Respiratory System Part 2Documento25 páginasThe Respiratory System Part 2ramadanAinda não há avaliações
- Thorax00105 0035 PDFDocumento4 páginasThorax00105 0035 PDFramadanAinda não há avaliações
- EMG IntroductionDocumento6 páginasEMG IntroductionramadanAinda não há avaliações
- Respiratory and Gastrointestinal Complications of Caustic Ingestion in ChildrenDocumento3 páginasRespiratory and Gastrointestinal Complications of Caustic Ingestion in ChildrenramadanAinda não há avaliações
- Corrosive Acid Ingestion in Clinical and Endoscopic Study: Man ADocumento5 páginasCorrosive Acid Ingestion in Clinical and Endoscopic Study: Man AramadanAinda não há avaliações
- Child Development: Resilience & Risk, A Course SyllabusDocumento17 páginasChild Development: Resilience & Risk, A Course SyllabusJane GilgunAinda não há avaliações
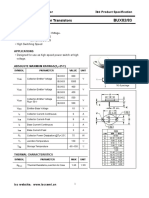
- Isc BUX82/83: Isc Silicon NPN Power TransistorsDocumento2 páginasIsc BUX82/83: Isc Silicon NPN Power TransistorsCarlos HCAinda não há avaliações
- Molecular Biology: Robert F. WeaverDocumento60 páginasMolecular Biology: Robert F. WeaverSidharth KhannaAinda não há avaliações
- CHAPTER 6 Maintenance Management: Introduction, Importance, Types & ReliabilityDocumento29 páginasCHAPTER 6 Maintenance Management: Introduction, Importance, Types & Reliabilitynur aidaAinda não há avaliações
- Processing Cacao Pod Husk into Low-Methoxyl PectinDocumento9 páginasProcessing Cacao Pod Husk into Low-Methoxyl PectinEmmanuel PlazaAinda não há avaliações
- MHWirth PileTopDrillRigs Brochure Web2Documento12 páginasMHWirth PileTopDrillRigs Brochure Web2geobyun100% (1)
- General Biology 1: Quarter 1 - Module - : Title: Cell CycleDocumento27 páginasGeneral Biology 1: Quarter 1 - Module - : Title: Cell CycleRea A. Bilan0% (1)
- Experi Men 22Documento7 páginasExperi Men 22bernardAinda não há avaliações
- Environmental Pollution Control (ET ZC362 - WILP Course) : BITS PilaniDocumento41 páginasEnvironmental Pollution Control (ET ZC362 - WILP Course) : BITS Pilanisa_arunkumarAinda não há avaliações
- Public Safety BriefingDocumento23 páginasPublic Safety BriefingHNNAinda não há avaliações
- 5090 w11 Ms 62Documento3 páginas5090 w11 Ms 62mstudy123456Ainda não há avaliações
- Rotex Brochure PDFDocumento4 páginasRotex Brochure PDFestramilsolutionAinda não há avaliações
- Effects of Air and Noise PollutionDocumento6 páginasEffects of Air and Noise Pollutionhaiqa malikAinda não há avaliações
- Indian Economy On The Eve of IndependenceDocumento5 páginasIndian Economy On The Eve of IndependenceAshiga RajendaranAinda não há avaliações
- Methyldopa Drug DataDocumento3 páginasMethyldopa Drug DataLaurel Joshua Reyes DauzAinda não há avaliações
- Level I Questions Thermal and Infrared Testing Method: Southern Inspection ServicesDocumento8 páginasLevel I Questions Thermal and Infrared Testing Method: Southern Inspection Servicesprabhakaran.SAinda não há avaliações
- ANGLICISMSDocumento14 páginasANGLICISMSManuel Jorquera100% (1)
- C9880046 Signed OfferLetterDocumento8 páginasC9880046 Signed OfferLetterẞhûpâthi RëddyAinda não há avaliações
- Crude Palm Oil MSDS Provides Safety InformationDocumento3 páginasCrude Palm Oil MSDS Provides Safety InformationCarlos MontanoAinda não há avaliações
- Bearing From Copper AlloyDocumento7 páginasBearing From Copper AlloyPhung Tuan AnhAinda não há avaliações
- Uco Bank Final (Simple Charts)Documento40 páginasUco Bank Final (Simple Charts)gopal8726Ainda não há avaliações
- Eastern RlyDocumento25 páginasEastern Rlyshivam.jhawar95Ainda não há avaliações
- Charles LawDocumento12 páginasCharles LawLerr Real RelleAinda não há avaliações
- RPH Finals Quiz BeeDocumento29 páginasRPH Finals Quiz BeeJoshua Liann EscalanteAinda não há avaliações
- Harmonized "Cluster" Document: For Electrical Connectors Conductive Plated CoatingsDocumento22 páginasHarmonized "Cluster" Document: For Electrical Connectors Conductive Plated CoatingsFrederico CésarAinda não há avaliações
- Thermocold AWC PROZONE Tech PDFDocumento44 páginasThermocold AWC PROZONE Tech PDFAlexAinda não há avaliações
- SWOT Analysis AuchanDocumento2 páginasSWOT Analysis AuchanDaniela DogaruAinda não há avaliações
- 17 Quarter 1 Module 17-ANAEROBICDocumento20 páginas17 Quarter 1 Module 17-ANAEROBICMah Jane DivinaAinda não há avaliações
- Cell Membrane TransportDocumento37 páginasCell Membrane TransportMaya AwadAinda não há avaliações
- Fever With Rash in Table Form.Documento4 páginasFever With Rash in Table Form.Azizan HannyAinda não há avaliações