Você também pode gostar
- Pediatric Abusive Head Trauma, Volume 2: Medical Mimics Pocket AtlasNo EverandPediatric Abusive Head Trauma, Volume 2: Medical Mimics Pocket AtlasAinda não há avaliações
- CASES (Long Form)Documento7 páginasCASES (Long Form)KiieEemAinda não há avaliações
- PRC TinaDocumento4 páginasPRC TinaCristina L. JaysonAinda não há avaliações
- PRC Form PDFDocumento4 páginasPRC Form PDFShariff Bernardo SarikinAinda não há avaliações
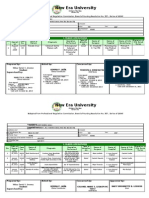
- WMSU Nursing FormsDocumento4 páginasWMSU Nursing FormsreraysAinda não há avaliações
- Major or Scrub, Circu PRC - VSMMC, CCMC, MaternityDocumento6 páginasMajor or Scrub, Circu PRC - VSMMC, CCMC, MaternityJellou MacAinda não há avaliações
- UZ Nursing FormsDocumento6 páginasUZ Nursing FormsRaf AylaniAinda não há avaliações
- Brent Hospital and Colleges IncorporatedDocumento4 páginasBrent Hospital and Colleges IncorporatedAlessandra MoonAinda não há avaliações
- Mindanao Sanitarium Nursing ClinicalsDocumento1 páginaMindanao Sanitarium Nursing ClinicalsCristina L. JaysonAinda não há avaliações
- Cases Baby Vince NursingDocumento5 páginasCases Baby Vince NursingSarah FabrosAinda não há avaliações
- WWW Arellano Edu PHDocumento18 páginasWWW Arellano Edu PHBungits AkoAinda não há avaliações
- WMSU Nursing FormsDocumento5 páginasWMSU Nursing FormsJenny S. SaquinAinda não há avaliações
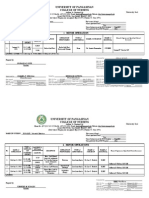
- University of Pangasinan College of Nursing: Minor OperationDocumento6 páginasUniversity of Pangasinan College of Nursing: Minor OperationJohnedel RosalesAinda não há avaliações
- New PRC Form SampleDocumento8 páginasNew PRC Form SampleLanie Esteban EspejoAinda não há avaliações
- FINAL PRC Plain (Blank)Documento6 páginasFINAL PRC Plain (Blank)Rez ApegoAinda não há avaliações
- PRC Initial DataDocumento5 páginasPRC Initial DataBryan Dave Rama JumeroAinda não há avaliações
- WinlynDocumento12 páginasWinlynWil MaeAinda não há avaliações
- CasesDocumento3 páginasCasesBeGie MamBaAinda não há avaliações
- MemeDocumento7 páginasMemeDiolan Novero BagorioAinda não há avaliações
- PRC - Dumlao, MarjorieDocumento5 páginasPRC - Dumlao, MarjorieMarjorie DumlaoAinda não há avaliações
- PRC Form CasesDocumento5 páginasPRC Form CasesAyen Fajardo-HernalAinda não há avaliações
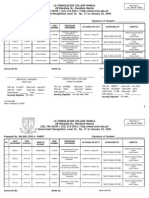
- Nursing Records from La Consolacion College ManilaDocumento5 páginasNursing Records from La Consolacion College ManilaAr DamotAinda não há avaliações
- ORDocumento20 páginasORTrish AldonAinda não há avaliações
- Lorma Colleges: ODC Form 1A Actual Delivery FormDocumento1 páginaLorma Colleges: ODC Form 1A Actual Delivery FormXTA_RICKYAinda não há avaliações
- MELVYNDocumento6 páginasMELVYNJohnedel RosalesAinda não há avaliações
- ORDocumento4 páginasORJoana Marie A. LaoAinda não há avaliações
- Nursing student clinical recordsDocumento9 páginasNursing student clinical recordsJean MoralesAinda não há avaliações
- PRCDocumento6 páginasPRCKate ChavezAinda não há avaliações
- Palasol 7 (Final)Documento6 páginasPalasol 7 (Final)Afreah BebzAinda não há avaliações
- PRC Form Cmo 14 IrishDocumento6 páginasPRC Form Cmo 14 IrishJonathan ObañaAinda não há avaliações
- PRC FormsDocumento5 páginasPRC FormsKevinJanCelestinoAinda não há avaliações
- University of The Visayas: Republic of The Philippines Professional Regulation Commission Board of NursingDocumento6 páginasUniversity of The Visayas: Republic of The Philippines Professional Regulation Commission Board of Nursingjames_Luvz17Ainda não há avaliações
- Southeast Asian College College of Nursing: Jessica Sarah A. JavierDocumento4 páginasSoutheast Asian College College of Nursing: Jessica Sarah A. JavierSarah JavierAinda não há avaliações
- Villar PRC Cases (DONE)Documento5 páginasVillar PRC Cases (DONE)Meijie Vino ManiegoAinda não há avaliações
- PRC Form For Nursing Students Planning To Take The Philippine Nurse's Licensure Examination University of Bohol, College of Nursing, Tagbilaran CityDocumento13 páginasPRC Form For Nursing Students Planning To Take The Philippine Nurse's Licensure Examination University of Bohol, College of Nursing, Tagbilaran CityMark Johnuel DuavisAinda não há avaliações
- Cases Blank FormDocumento6 páginasCases Blank FormIara CruzAinda não há avaliações
- PRC Forms JC - 1Documento6 páginasPRC Forms JC - 1Rhea VillanuevaAinda não há avaliações
- Western Mindanao State UniversityDocumento4 páginasWestern Mindanao State UniversityJehannaMarEnggingAbdurahmanAinda não há avaliações
- Dadang - or CasesDocumento3 páginasDadang - or Casesadang1021Ainda não há avaliações
- PRC Form Ralph NewaaaaaaaaaaaaaaaaaaaaaDocumento13 páginasPRC Form Ralph NewaaaaaaaaaaaaaaaaaaaaaJabez TyAinda não há avaliações
- Minor or Format TemplateDocumento2 páginasMinor or Format TemplateKwesi YasayAinda não há avaliações
- Case KidotDocumento7 páginasCase KidotcabantasAinda não há avaliações
- Roy Cord Dress DR in BRTTHDocumento8 páginasRoy Cord Dress DR in BRTTHIbrahim RegachoAinda não há avaliações
- New PRC (2) IvyDocumento6 páginasNew PRC (2) IvyJess L PayagAinda não há avaliações
- Republic of The Philippines University Town, Northern Samar: Odc Form 1A Actual Delivery FormDocumento5 páginasRepublic of The Philippines University Town, Northern Samar: Odc Form 1A Actual Delivery FormrianicoamAinda não há avaliações
- "The Institution For Better Life": Northern Christian College College of NursingDocumento5 páginas"The Institution For Better Life": Northern Christian College College of NursingMorayata AlishabulaAinda não há avaliações
- Medical Colleges of Northern PhillipinesDocumento5 páginasMedical Colleges of Northern Phillipinesbarbiegirl9497Ainda não há avaliações
- Roy Circulating or in BRTTHDocumento7 páginasRoy Circulating or in BRTTHIbrahim RegachoAinda não há avaliações
- I. Major Operations: Urdaneta City UniversityDocumento11 páginasI. Major Operations: Urdaneta City UniversityEdgar GarciaAinda não há avaliações
- Adapted By: Far Eastern University: Cephalic in Labor Low Transverse Cesarean Section PrimaryDocumento5 páginasAdapted By: Far Eastern University: Cephalic in Labor Low Transverse Cesarean Section PrimaryArvee SimanganAinda não há avaliações
- Jeng 1Documento8 páginasJeng 1Marianne BaquilalaAinda não há avaliações
- Beth PRC FormDocumento11 páginasBeth PRC FormNev Bryan DapitanAinda não há avaliações
- Max Suniel ST., Carmen, Cagayan de Oro CityDocumento18 páginasMax Suniel ST., Carmen, Cagayan de Oro CityTinAinda não há avaliações
- C.C.D 6137 Gladys Anne Cristine P. AquinoDocumento6 páginasC.C.D 6137 Gladys Anne Cristine P. Aquinoroneldayo62Ainda não há avaliações
- PRC FormDocumento6 páginasPRC FormMarisCacheroAinda não há avaliações
- ST. RITA HOSPITAL CLINICAL RECORDSDocumento6 páginasST. RITA HOSPITAL CLINICAL RECORDSJomari CarreonAinda não há avaliações
- Zamboanga City Medical Center, Zamboanga City: Surgical Procedure PerformedDocumento2 páginasZamboanga City Medical Center, Zamboanga City: Surgical Procedure PerformedEdmund RufinoAinda não há avaliações
- Assist 4Documento1 páginaAssist 4Elleb Nataly MerchedAinda não há avaliações
- Zamboanga City Medical Center, Zamboanga City: Nature of DeliveryDocumento7 páginasZamboanga City Medical Center, Zamboanga City: Nature of DeliverySharf WangAinda não há avaliações
- Energy ThumpsDocumento3 páginasEnergy ThumpsTink De NeverlandAinda não há avaliações
- G128 0066721 MSDSDocumento8 páginasG128 0066721 MSDSfiguev2208Ainda não há avaliações
- Halozyme Therapeutics, Inc. 2009 Investor Day PresentationDocumento88 páginasHalozyme Therapeutics, Inc. 2009 Investor Day Presentationsstrumello7395Ainda não há avaliações
- Nursing Care Plan: Problem Identified: Difficulty of BreathingDocumento1 páginaNursing Care Plan: Problem Identified: Difficulty of BreathingCaroline ChaAinda não há avaliações
- Acid Group of Remedies in HomoeopathyDocumento5 páginasAcid Group of Remedies in HomoeopathyNagender UpadhyayAinda não há avaliações
- Science: Quarter 2 - Module 1Documento20 páginasScience: Quarter 2 - Module 1Kate BatacAinda não há avaliações
- Laporan Diet Pasca BedahDocumento13 páginasLaporan Diet Pasca BedahYuliza RosalinaAinda não há avaliações
- Steroid Tapering and Supportive Treatment Guidance V1.0 PDFDocumento1 páginaSteroid Tapering and Supportive Treatment Guidance V1.0 PDFNthutagaol TrusAinda não há avaliações
- Clsi 2012Documento50 páginasClsi 2012niluh suwasanti100% (1)
- Referral for dietitian assessment of swallowing riskDocumento72 páginasReferral for dietitian assessment of swallowing riskjykaAinda não há avaliações
- Bipolar and Related Disorder: Recio, Kate M. Far Eastern University - Cavite PSY1831-ADocumento20 páginasBipolar and Related Disorder: Recio, Kate M. Far Eastern University - Cavite PSY1831-AKate RecioAinda não há avaliações
- 1 Hygene and SanitationDocumento22 páginas1 Hygene and SanitationJammil Ud-ulonAinda não há avaliações
- Khushboo PPT Covid 19Documento17 páginasKhushboo PPT Covid 19Birlal SinghAinda não há avaliações
- Achilles Tendon Conditions Signs and SymptomsDocumento1 páginaAchilles Tendon Conditions Signs and SymptomsTessa DagutAinda não há avaliações
- Managing Pain After AppendectomyDocumento2 páginasManaging Pain After AppendectomyChatoh SanaoAinda não há avaliações
- SenokotDocumento1 páginaSenokotKatie McPeek100% (1)
- History and P.E. of The Integumentary SystemDocumento6 páginasHistory and P.E. of The Integumentary SystempazucenaAinda não há avaliações
- Drug Study Quinine SulfateDocumento7 páginasDrug Study Quinine SulfateKathlyn_Matic_6376Ainda não há avaliações
- International Classification of Diseases 9Documento6 páginasInternational Classification of Diseases 9Carlos Alberto ZepedaAinda não há avaliações
- Kala-Azar (Leishmaniasis) Symptoms, Signs, DiagnosisDocumento36 páginasKala-Azar (Leishmaniasis) Symptoms, Signs, Diagnosisatulbd2006Ainda não há avaliações
- MODUL 1 FKG UnairDocumento61 páginasMODUL 1 FKG UnairLaurensia NovenAinda não há avaliações
- Glossary of EMTDocumento5 páginasGlossary of EMTErnan BaldomeroAinda não há avaliações
- Perbedaan Kepadatan Lalat Yang Hinggap Pada Fly Grill Yang Berbeda Warna Di Pasar SrimangunanDocumento80 páginasPerbedaan Kepadatan Lalat Yang Hinggap Pada Fly Grill Yang Berbeda Warna Di Pasar SrimangunanIrina MayasisianaAinda não há avaliações
- Cheat Sheet 2Documento5 páginasCheat Sheet 2Katelyn HillAinda não há avaliações
- Chapter 1-Assessment A. Nursing Health History Demographic DataDocumento11 páginasChapter 1-Assessment A. Nursing Health History Demographic DataxxkaceAinda não há avaliações
- Neoadjuvant Chemoradiotherapy Plus Surgery Versus Surgery Alone For Oesophageal or Junctional Cancer (CROSS) Long-Term Results of A Randomised Controlled TrialDocumento9 páginasNeoadjuvant Chemoradiotherapy Plus Surgery Versus Surgery Alone For Oesophageal or Junctional Cancer (CROSS) Long-Term Results of A Randomised Controlled TrialSergioAinda não há avaliações
- 3595 Article 14344 1 10 20230529Documento4 páginas3595 Article 14344 1 10 20230529ReendiIshqAinda não há avaliações
- Daftar PustakaDocumento6 páginasDaftar PustakaChintiaAinda não há avaliações
- Hamer - Five Laws - Cancer Congress PDFDocumento23 páginasHamer - Five Laws - Cancer Congress PDFFelipe Gomes100% (1)
- Aubf Module 3 Laboratory Assignment - Macabanding - PrincessDocumento5 páginasAubf Module 3 Laboratory Assignment - Macabanding - PrincessNailah MacabandingAinda não há avaliações