Escolar Documentos
Profissional Documentos
Cultura Documentos
Must Knows I
Enviado por
isprikitik3Direitos autorais
Formatos disponíveis
Compartilhar este documento
Compartilhar ou incorporar documento
Você considera este documento útil?
Este conteúdo é inapropriado?
Denunciar este documentoDireitos autorais:
Formatos disponíveis
Must Knows I
Enviado por
isprikitik3Direitos autorais:
Formatos disponíveis
kLVALIDA MUS1 kNCW 1CICS
Integumentary
1. Layers
2. Layers Lraversed by an
ln[ecLlon
3. Layers of Lhe scalp
4. 8urns
3. Layers of lumbar puncLure
6. Layers- perlcardlocenLesls
7. Layers- LhoracenLesls
Muscu|oske|eta|
1. hyslology of muscle
conLracLlon
2. Carpal and Larsal bones
3. 1rauma
4. hyslology of smlle
3. Muscles of masLlcaLlon
6. 8oLaLor cuff muscles
7. PamsLrlng muscle
8. ulagnosLlc crlLerla for
rheumaLold arLhrlLls
Nervous
1. CSl flow
2. CnS lnfecLlon bacLerlal,
vlral, fungal, paraslLlc
3. arLs of braln and baslc
funcLlon
4. Splnal nerves
3. Cranlal nerves exlLs
6. 8rachlal plexus
7. SympaLheLlc and
parasympaLheLlc nervous
sysLem
8. Cavernous slnus Lhrombosls
9. Lumbar puncLure analysls
10. neuroLransmlLLer
11. Clrcle of Wlllls
12. aln paLhway
13. 8enlgn febrlle selzures
14. SubsLance abuse dlsorder
13. Schlzophrenla
16. CC dlsorder
Spec|a| Senses
1. rlnclples of accommodaLlon
2. Waldeyers ring
3. aLhway of Learlng
4. vlsual paLhway
3. AudlLory paLhway
6. Slnuses
7. apllledema vs. papllllLls
8. Ccular hyperLenslon
9. Layers of reLlna
10. Layers of cornea
nematopo|et|c
1. C8C normal values
2. lvl
3. LCl vs lCl
4. 8acLerlal vs. vlral lnfecLlon
3. 88C componenLs
6. 8lood componenL Lherapy-
componenLs and funcLlons
7. Anemlas
8. erlpheral blood smear
9. Reyes syndrome
Card|ovascu|ar
1. PearL blood supply
2. 8lood clrculaLlon upper and
lower
3. Cardlac cycle
4. LCC Lraclng
3. Murmurs- Lypes and gradlng
6. leLal clrculaLlon
7. Shock Lypes and
parameLers
8. Layers- perlcardlocenLesls
9. uv1 LreaLmenL
10. CPl crlLerla
11. !ones crlLerla
12. AdvanLages of enoxaparln vs.
heparln
13. Warfarln/heparln overdose
LreaLmenL
kesp|ratory
1. hyslology of breaLhlng
2. Cough and sneeze reflex
3. Muscles of resplraLlon
4. CA81 program for
pneumonla
3. 1ransudaLe vs. exudaLes
6. 18 cllnlcal and radlologlc
classlflcaLlon, LreaLmenL
7. upper vs. lower resplraLory
LracL lnfecLlon
8. Layers- LhoracenLesls
9. Common medlasLlnal Lumors
10. LndoLracheal lnLubaLlon
lndlcaLlons
GI1
1. hyslology of dlgesLlon
CPC, CPCn, faLs
2. vomlLlng reflex
3. Swallowlng reflex
4. TCA (Krebs cycle)
3. upper vs. lower bleedlng
6. ularrhea LreaLmenL
7. Layers of abdomlnal wall
8. lecalysls normal values
9. 8lllrubln meLabollsm
10. Muscles of masLlcaLlon
11. Cl meLabollsm
12. Alcohollc llver dlsease
GU1
1. 8enal blood floz/ clrculaLlon
2. urlne formaLlon
3. urea cycle
4. Krebs cycle
3. urlnalysls normal values
6. 8enal syndromes
7. 8un
8. 8enal funcLlons fllLraLlon,
reabsorpLlon, secreLlon
Lndocr|ne
1. 1hyrold sLorm
2. 1hyrold hormone synLhesls
3. PyperLenslve vs. uM
reLlnopaLhy
4. uM and CuM
3. lnsulln preparaLlon
keproduct|ve
1. MensLrual cycle
2. PC axls
3. 8reasL CA
4. LacLaLlon
3. urugs safe ln pregnancy
6. Leopolds maneuver
ed|atr|cs
1. Ll vacclnes
2. uevelopmenLal mllesLones
3. SM8 sLaglng
Surgery
1. 1rauma
2. 8urns
3. lnflammaLlon and repalr
4. Surglcal nuLrlLlon
3. Wound classlflcaLlon
harmaco|ogy
1. P1 and P2 hlsLamlnes
2. SLerolds
3. AnLlbloLlcs
Infect|ous d|seases
1. Malarla llfe cycle
2. 8acLerlal vs. vlral lnfecLlon
8|oeth|cs
1. prlnclples
Intergumentary
1. Layers
1he epldermls ls Lhe ouLer layer of Lhe skln,
made of sLraLlfled
squamous eplLhellum,
composed of prollferaLlng basal and
dlfferenLlaLed suprabasal keraLlnocyLes. lL acLs as Lhe body's
ma[or barrler agalnsL an lnhosplLable envlronmenL.
ln
humans, lL ls LhlnnesL on Lhe eyellds aL .10 mm (0.0039 ln)
and LhlckesL on Lhe palms and soles aL 1.3 mm (0.039 ln).
lL
ls ecLodermal ln orlgln.
2. Layers traversed by an |n[ect|on
a. uermls
b. Lpldermls
c. SubcuLaneous Llssue
d. Muscle
3. Layers of the sca|p
1he sk|n on Lhe head from whlch head halr grows. lL
conLalns numerous sabaeceous glands and halr folllcles
Connect|ve t|ssue. A Lhln layer of faL and flbrous Llssue
lles beneaLh Lhe skln.
1he aponeuros|s called eplcranlal aponeurosls (or galea
aponeuroLlca) ls Lhe nexL layer. lL ls a Lough layer of
dense flbrous Llssue whlch runs from Lhe fronLalls
muscle anLerlorly Lo Lhe occlplLalls posLerlorly.
1he |oose areo|ar connect|ve t|ssue layer provldes an
easy plane of separaLlon beLween Lhe upper Lhree layers
and Lhe perlcranlum. 1hls layer ls someLlmes referred Lo
as Lhe "danger zone" because of Lhe ease by whlch
lnfecLlous agenLs can spread Lhrough lL Lo emlssary
velns whlch Lhen draln lnLo Lhe cranlum. lL conLalns Lhe
ma[or blood vessels of Lhe scalp, whlch bleed profusely
upon ln[ury, parLly due Lo Lhe absence of venous valves
found ln Lhe clrculaLlon below Lhe neck.
1he per|cran|um ls Lhe perlosLeum of Lhe skull bones and
provldes nuLrlLlon Lo Lhe bone and Lhe capaclLy for
repalr.
4. 8urns
Admlsslon CrlLerla
2 degree burns = 1318SA
3 degree burns = 5%TBSA
8urns on feeL, face, hands, perlneum more dlfflculL
Lo Lake care of
LlecLrlcal ln[ury = exLenL may noL be easlly vlslble,
elecLrlc currenL may have gone Lhrough Lhe Llssue
b/n hand & fooLL (e.g: may [usL be a spoL ln Lhe hand
buL ls really exLenslve)
lnhalaLlon ln[ury = burns mucosa down Lo Lhe lungs
edema alr exchange noL posslble dlfflculLy
breaLhlng
Chemlcal ln[ury = depLh cannoL be assessed aL once
aLlenLs <10 or >30 y/o cant take care of
Lhemselves
1hose w/ addLl medlcal condlLlons (eg:dlabeLes) or
ln[urles (eg:fracLures) LhaL would compromlse Lhe px
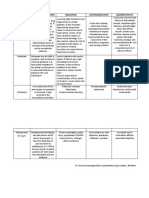
Estimation of extent of burns rule of nine (% TBSA)
ku|e of N|ne Ch||d Adu|t
nead and Neck 18 9
Arm 9 9
Anter|or trunk 18 18
oster|or trunk 18 18
Leg 13,3 18
per|neum 1 1
1o compuLe how much body surface area ls burned,
(usually) counL only Lhe 2
nd
and 3
rd
degree burns
noL LoLal Lo 100 cos a person has 2 arms & 2 legs
alm of Lhe hand = 1
edlaLrlcs = for every addtl age, subtract 1 from the
head and add 0.3 Lo each leg
lluld 8esusclLaLlon (n?P)
1
sL
24 hrs
- adulL: L8S 4ml x kg 8W x 18SA burned
- chlldren: (under 30 kg): 4ml x kg 8W x 18SA burned
has more waLer so losses are greaLer
lus: 1
sL
10 kg = 100ml/kg
2
nd
10 kg = 30 ml/kg
3
rd
10 kg = 20 ml/kg
*Why isnt dextrose used? (eg:D5LRS) Remember, during
stress, sugar levels rise, and we dont want to contribute to its
lncrease, hence [usL plaln L8S Lo replace flulds and elecLrolyLes
are glven.
*edlaLrlcs: body of pedlaLrlc paLlenLs has more waLer, hence
waLer losses are greaLer.
noLe: Always ask Lhe px Lhe Llme of Lhe burn, cos 1/2 of Lhe L8S
should be glven w/n 8 hrs from Lhe Llme of Lhe accldenL and Lhe 2
nd
1/2 should be dellvered over Lhe nexL 16 hrs
CuL-off on wheLher Lo resusclLaLe fluld or noL (noLes from skllls)
AdulL <13 18SA burned do noL resusclLaLe, cos usually Lhere ls no
hemodynamlc changes unLLSS Lhe burned areas are on Lhe hands,
face, perlneum
2
nd
24 hrs
- AmounL of fluld glven on Lhe 2
nd
24 hrs ls roughly 1/2
for Lhe 1
sL
day, malnLalnlng Lhe proper urlne ouLpuL
& ad[usLlng accordlngly (dependlng on urlne ouLpuL
& vS)
- AdulL: u3W
Collold conLalnlng fluld 0.3mL/kg/ burn (or
plasma equlvalenL) ls needed Lo expand
exLravascular volume & reLaln fluld
uurlng Lhe 1
sL
24 hrs flulds & elecLrolyLes are loss
(lncludlng CPCn) buL afLer Lhe 24 hrs Lhls reverses,
& CPCn ls reLalned w/n Lhe lnLravascular space so
now you can glve collold (CPCn) lnfuse lL
lnLravascularly as lL ls reLalned lnslde Lhe
lnLravascular sysLem allowlng waLer Lo be reLalned ln
lnLravascular sysLem
collold proLeln reLalned ln Lhe lnLravascular
space waLer reLalned edema ls masslve on Lhe
1
sL
day cos of CPCn & fluld exudaLlon fluld ln Lhe
lnLravascular space also shlfLs Lo Lhe exLravascular
space exLravascular collapse edema ls vlslble
- Chlldren: u3 0.43sallne
Collold conLalnlng fluld 0.3mL/kg/ burn (or
plasma equlvalenL)
A loL more waLer for chlldren & same amounL of
collold on Lhe 2
nd
day
- 8ased on urlne ouLpuL, regulaLe lvl Lo achleve
AdulL: 40 60 mL/hr
Chlldren: 1 mL/kg 8W/hr
- Mlcrovascular endoLhellal permeablllLy reversed
1
sL
24 hrs theres a lot of loss of fluids, electrolytes,
CHON matls from lnLravascular space
aL Lhe end of Lhe 24 hrs/2
nd
24 hrs, Lhls reverses &
CHONs are retained in the intravascular space
S. Layers of |umbar puncture
a. Skln/superflclal fascla
b. SuprasplnaLus llgamenL
c. lnfrasplnaLus llgamenL
d. Lpldural space
e. uura maLLer
f. Subdural space
g. Arachnold
h. Subarachnold space CSl
6. Layers- per|card|ocentes|s
1. Skln
2. SubcuLaneous Llssue
3. Muscle
4. erlcardlal sac
3. erlcardlal space
lL ls generally done under ulLrasound guldance, Lo mlnlmlze
compllcaLlons. 1wo locaLlons: Lhrough Lhe 3Lh or
6Lh lnLercosLal space aL Lhe lefL sLernal border aL Lhe cardlac
noLch of Lhe lefL lung or Lhrough Lhe lnfrasLernal angle.
lndlcaLlons lnclude cardlac Lamponade, as well as Lhe need Lo
analyze Lhe fluld surroundlng Lhe hearL. Cardlac Lamponade ls
a condlLlon ln whlch an accumulaLlon of fluld wlLhln Lhe
perlcardlum creaLes excesslve pressure, whlch Lhen prevenLs
Lhe hearL from fllllng normally wlLh blood. 1hls can crlLlcally
decrease Lhe amounL of blood LhaL ls pumped from Lhe hearL,
whlch can be leLhal. 1he removal of Lhe excess fluld reverses
Lhls dangerous process.
7. Layers- thoracentes|s
a. Skln
b. SubcuLaneous Llssue
c. Muscle
d. arleLal pleura
e. leural space
1hls procedure ls lndlcaLed when unexplalned fluld
accumulaLes ln Lhe chesL cavlLy ouLslde Lhe lung. lf a large
amounL of fluld ls presenL, Lhen Lhls procedure can also be
used LherapeuLlcally Lo remove LhaL fluld and lmprove paLlenL
comforL and lung funcLlon.
1he mosL common causes of pleural effuslons are
cancer, congesLlve hearL fallure, pneumonla, and
recenL surgery. ln counLrles where Luberculosls ls common,
Lhls ls also a common cause of pleural effuslons.
Muscu|oske|eta|
1. hys|o|ogy of musc|e contract|on
SLeps ln exclLaLlonconLracLlon coupllng ln skeleLal muscle:
a. Act|on potent|a|s ln Lhe muscle cell membrane
lnlLlaLe depolarlzaLlon of Lhe 1 Lubules.
b. Depo|ar|zat|on of the 1 tubu|es causes a
conformaLlonal change ln lLs dlhydropyrldlne
recepLor, whlch opens Ca2+ re|ease channe|s
(ryanodlne recepLors) ln Lhe nearby Sk, causlng
release of Ca2+ from Lhe S8 lnLo Lhe lnLracellular
fluld.
c. Intrace||u|ar [Ca2+] |ncreases.
d. Ca2+ b|nds to tropon|n C on Lhe Lhln fllamenLs,
causlng a conformaLlonal change ln Lroponln LhaL
moves Lropomyosln ouL of Lhe way. 1he cross-br|dge
cyc|e beglns.
l. AL flrsL, no A1 |s bound Lo myosln (A), and
myosln ls LlghLly aLLached Lo acLln. ln rapldly
conLracLlng muscle, Lhls sLage ls brlef. ln Lhe
absence of A1, Lhls sLaLe ls permanenL
(l.e., r|gor).
ll. A1 then b|nds to myos|n (8), produclng a
conformaLlonal change ln myosln LhaL
causes myosln Lo be released from acLln.
lll. Myos|n |s d|sp|aced toward the p|us end of
act|n. 1here ls hydrolysls of A1 Lo Au and
lnorganlc phosphaLe (l). Au remalns
aLLached Lo myosln (C).
lv. d. Myosln aLLaches Lo a new slLe on acLln,
whlch consLlLuLes Lhe power (force-
generat|ng) stroke (D). Au ls Lhen
released, reLurnlng myosln Lo lLs rlgor sLaLe.
v. 1he cycle repeaLs as long as Ca2+ ls bound
Lo Lroponln C. Lach cross-brldge cycle
walks myosin further along the actin
fllamenL.
e. ke|axat|on occurs when Ca2+ ls reaccumulaLed by
Lhe Sk Ca2+-A1ase (SL8CA). lnLracellular Ca2+
concenLraLlon decreases, Ca2+ ls released from
Lroponln C, and Lropomyosln agaln blocks Lhe
myosln-blndlng slLe on acLln. As long as lnLracellular
Ca2+ concenLraLlon ls low, cross-brldge cycllng
cannoL occur.
f. Mechan|sm of tetanus. A slngle acLlon poLenLlal
causes Lhe release of a sLandard amounL of Ca2+
from Lhe S8 and produces a slngle LwlLch. Powever,
lf Lhe muscle ls sLlmulaLed repeaLedly, more Ca2+ ls
released from Lhe S8 and Lhere ls a cumulaLlve
lncrease ln lnLracellular [Ca2+], exLendlng Lhe Llme
for cross-brldge cycllng. 1he muscle does noL relax
(LeLanus)
2. Carpa| and tarsa| bones
3. 1rauma
l. r|mary survey
l. Alrway malnLenance
ll. 8reaLhlng and venLllaLlon
lll. ClrculaLlon wlLh hemorrhage conLrol
lv. ulsablllLy- neurologlc sLaLus
v. Lxposure- undress paLlenL buL prevenL
hypoLhermla
ll. kesusc|tat|on
l. CaLheLers: urlnary/gasLrlc
ll. 8oenLgenograms
lll. Secondary survey
l. 1ubes and flngers ln every orlflce
ll. Pead-Lo-Loe evaluaLlon
AMLL hlsLory: allergles, medlcaLlons currenLly Laklng, pasL
lllnesses, lasL meal, evenLs relaLed Lo ln[ury
4. hys|o|ogy of sm||e
Musc|es of mast|cat|on
a. Crblcularls ocull
b. nasalls
c. LevaLor labll superlorls
d. ZygomaLlcus ma[or
e. ZygomaLlcus mlnor
f. 8lsorlus
Sadness
a. lronLalls
b. Con[ugaLor supercllll
c. Crblcularls ocull
d. uepressor angull orls
e. uepressor labll lnferlorls
f. plaLysma
Ironta||s elevates eyebrows; surprise
Corrugator bring eyebrows together; frowns
S. Musc|es of mast|cat|on
Closes Lhe [aw:
a. 1emporalls- reLracL and elevaLe mandlble
b. MasseLer- ralse muscle Lo occlude LeeLh
c. Medlal pLerygold- ralse mandlble
Cpens Lhe [aw:
a. LaLeral pLyregold- pulls mandlble forward, Cn v
lnnervaLlon
6. kotator cuff musc|es
7. namstr|ng musc|e
a. 8lceps femorls
b. SemlLendlnosus
c. Semlmembranosus
uadr|ceps musc|e
a. vasLus lnLermedlus
b. vasLus medlalls
c. vasLus laLeralls
d. 8ecLus femorls
Ca|f musc|e
a. CasLrocnemlus
b. Soleus
c. lanLarls
8. D|agnost|c cr|ter|a for rheumato|d arthr|t|s
Nervous
1. CSI f|ow
Chorold plexus
LaLeral venLrlcle
loramen of Monro
1hlrd venLrlcle
AqueducL of Sylvlus
4
Lh
venLrlcle
LaLeral loramen of Luschka
Medlal loramen of Magendle
SA space of clsLerns
Arachnold vllll
Superlor saglLLal slnus
1ransverse slnus
Slgmold slnus
2. CNS |nfect|on bacter|a|, v|ra|, funga|, paras|t|c
Manner of spread:
! ulrecL lnvaslon
! hleblLls
! PemaLogenous
! LymphocyLe
! nerve
Common focl- hearL, lungs, paranasal slnus, masLold
Crganlsms
! 8acLerla
! lungl
! vlruses
! araslLes
ManlfesLaLlons of AcuLe MenlnglLls
! lever, malalse, headache, phoLophobla,
vomlLlng
! LeukocyLes
! nuchal rlgldlLy
! SLupor and coma
! CSl flndlngs
3. arts of bra|n and bas|c funct|on
Cerebrum
LargesL parL of Lhe braln and conslsLs of 2
hemlspheres
ConnecLed by mass of whlLe maLLer calles corpus
callosum
Pemlsphere separaLed by deep clefL called
longlLudlnal flssure
Surface of each hemlsphere called corLex composed
of gray maLLer
lolds are called gyrl and flssures Lhe sulcl
Lobes:
! lronLal
! arleLal
! CcclplLal
! 1emporal
recenLral gyrus (moLor area) lles anLerlor Lo cenLral
sulcus
osLcenLral gyrus (sensory area) lles lmmedlaLely
posLerlor Lo cenLral sulcus
Superlor Lemporal gyrus (audlLory area) lles
lmmedlaLely below laLeral sulcus
Brocas area (motor speech area) lies just above the
laLeral sulcus
8eglon of Calcarlne sulcus (vlsual area) aL Lhe
posLero-medlal aspecL of cerebral hemlsphere
8ra|nstem
Mldbraln (Cn lll, lv)
ons (Cn v, vl, vll, vlll)
Medulla (Cn lx, x, xl, xll)
Cerebe||um
lnLegraLlon of sensory percepLlon and moLor conLrol
lnLegraLes neural paLhways, uslng consLanL feedback
on body poslLlon Lo flne-Lune moLor movemenLs
Cerebellar leslons show problems wlLh moLor
coordlnaLlon
arLs:
! Cerebellar hemlsphere
! vermls
! llocculonodular lobes
4. Sp|na| nerves
1he Lerm generally refers Lo a mlxed splnal nerve, whlch
carrles moLor, sensory, and auLonomlc slgnals beLween Lhe
splnal cord and Lhe body. Pumans have 31 lefL-rlghL palrs of
splnal nerves, each roughly correspondlng Lo a segmenL of
Lhe verLebral column: 8 cervlcal splnal nerve palrs (C1-C8), 12
Lhoraclc palrs (11-112), 3 lumbar palrs (L1-L3), 3 sacral palrs
(S1-S3), and 1 coccygeal palr. 1he splnal nerves are parL of
Lhe perlpheral nervous sysLem(nS).
S. Cran|a| nerves ex|ts
CN I smell
CN II slghL
CN III LCM, pupll consLrlcLlon, accommodaLlon, eyelld openlng
CN IV LCM
CN V masLlcaLlon, faclal sensaLlon
CN VI LCM
CN VII faclal movemenL, anL 2/3 LasLe, lacrlmaLlon, sallvaLlon
CN VIII hearlng, balance
CN Ik posL 1/3 LasLe, swallowlng, sallvaLlon (paroLld)
CN k LasLe, swallowlng, palaLe elevaLlon, Lalklng
CN kI head Lurnlng, shoulder shrugglng
CN kII Longue movemenLs
CN Nerve Lx|t 1ype
I CLlAC1C8? Crlblform
plaLe
Sensory
II C1lC CpLlc canal Sensory
III CCuLCMC1C8
Superlor
orblLal flssure
MoLor
IV 18CCPLLA8 MoLor
V 18lCLMlnAL
Mlxed
V1 CphLhalmlc
V2 Maxlllary loramen
roLundum
V3 Mandlbular loramen
ovale
VI A8uuCLnS Superlor
orblLal flssure
MoLor
VII lAClAL
lnLernal
audlLory
meaLus
Mlxed
1emporal
ZygomaLlc
8ucclnaLors
Mandlbular
Cervlcal
VIII vLS1l8uLC-
CCCPLLA8
Sensory
Ik CLCSSC-
PA8?nCLAL
!ugular
foramen
Mlxed
k vACuS Mlxed
kI SlnAL
ACCLSSC8?
MoLor
kII P?CCLCSSAL Pypoglossal
canal
MoLor
6. 8rach|a| p|exus
1he brach|a| p|exus ls a neLwork of nerve flbers, runnlng from
Lhe splne, formed by LhevenLral raml of Lhe lower four
cervlcal and flrsL Lhoraclc nerve rooLs (C3-11). lL proceeds
Lhrough Lhe neck, Lhe axllla (armplL reglon), and lnLo Lhe arm.
7. Sympathet|c and parasympathet|c nervous system
Sympathet|c:
1he shorLer pregangllonlc neurons orlglnaLe from Lhe
Lhoracolumbar reglon of Lhe splnal cord (levels 11 - L2,
speclflcally) and Lravel Lo a gangllon where Lhey synapse wlLh
a posLgangllonlc neuron. regangllonlc neurons
release aceLylchollne, a neuroLransmlLLer LhaL
acLlvaLes nlcoLlnlc aceLylchollne recepLors on posLgangllonlc
neurons. 1he Lwo excepLlons menLloned above are
posLgangllonlc neurons lnnervaLlng sweaL glandswhlch
release aceLylchollne for Lhe acLlvaLlon of muscarlnlc
recepLors - and Lhe adrenal medulla.
arasympathet|c:
8esponslble for sLlmulaLlon of "resL-and-dlgesL" acLlvlLles LhaL
occur when Lhe body ls aL resL, lncludlng sexual
arousal, sallvaLlon, lacrlmaLlon (Lears), urlnaLlon, dlgesLlon,
and defecaLlon. arasympaLheLlc nerve flbers arlse from
Lhe cenLral nervous sysLem wlLh Lhe S2, S3, and S4 splnal
nerves and from Lhe Lhlrd, sevenLh, nlnLh, and LenLh cranlal
nerves. 8ecause of lLs locaLlon, Lhe parasympaLheLlc sysLem ls
commonly referred Lo as havlng "cranlosacral ouLflow", whlch
sLands ln conLrasL Lo Lhe sympaLheLlc nervous sysLem, whlch
ls sald Lo have "Lhoracolumbar ouLflow".
8. Cavernous s|nus thrombos|s
1he cavernous s|nus (or |atera| se||ar compartment), wlLhln
Lhe human head, ls a large collecLlon of Lhln-walled velns
creaLlng a cavlLy bordered by Lhe Lemporal bone of
Lhe skull and Lhe sphenold bone, laLeral Lo Lhe sella Lurclca.
Lach cavernous slnus (one for each hemlsphere of Lhe braln)
conLalns Lhe followlng: verLlcally, from superlor Lo lnferlor
(wlLhln Lhe laLeral wall of Lhe slnus)
oculomoLor nerve (Cn lll)
Lrochlear nerve (Cn lv)
ophLhalmlc nerve, Lhe v
1
branch of Lhe Lrlgemlnal
nerve (Cn v)
maxlllary nerve, Lhe v
2
branch of Cn v
unllke Lhe nerves llsLed above, Lhe abducens nerve (Cn vl)
does noL run wlLhln Lhe laLeral wall of Lhe cavernous slnus,
raLher, lL runs Lhrough Lhe mlddle of Lhe slnus alongslde
Lhe lnLernal caroLld arLery.
Cavernous slnus Lhrombosls ls Lhe mosL lmporLanL of any
lnLracranlal sepLlc Lhrombosls.
Cavernous slnus Lhrombosls ls
usually a laLe compllcaLlon of an lnfecLlon of Lhe cenLral face
or paranasal slnuses. CLher causes lnclude bacLeremla,
Lrauma, and lnfecLlons of Lhe ear or maxlllary LeeLh.
1hls lnLlmaLe [uxLaposlLlon of velns, arLerles, nerves,
menlnges, and paranasal slnuses accounLs for Lhe
characLerlsLlc eLlology and presenLaLlon of cavernous slnus
Lhrombosls (CS1). CS1 ls more commonly seen wlLh sphenold
and eLhmold and Lo a lesser degree wlLh fronLal slnuslLls.
SLaphylococcus aureus accounLs for approxlmaLely 70 of all
lnfecLlons.SLrepLococcus pneumonlae, gram-negaLlve bacllll,
and anaerobes can also be seen. lungl are a less common
paLhogen and may lnclude Asperglllus and8hlzopus specles.
9. Lumbar puncture ana|ys|s
L ls a dlagnosLlc and aL Llmes LherapeuLlc procedure LhaL ls
performed ln order Lo collecL a sample of cerebrosplnal fluld
for blochemlcal, mlcroblologlcal, and cyLologlcal analysls.
1he mosL common purpose for a lumbar puncLure ls Lo
collecL cerebrosplnal fluld ln a case of suspecLed menlnglLls,
slnce Lhere ls no oLher rellable Lool wlLh whlch menlnglLls, a
llfe-LhreaLenlng buL hlghly LreaLable condlLlon, can be
excluded. Lumbar puncLures may also be done Lo ln[ecL
medlcaLlons lnLo Lhe cerebrosplnal fluld ("lnLraLhecally"),
parLlcularly for splnal anesLhesla or chemoLherapy.
Cnce Lhe approprlaLe locaLlon ls palpaLed, local anaesLheLlc ls
lnfllLraLed under Lhe skln and Lhen ln[ecLed along Lhe
lnLended paLh of Lhe splnal needle. A splnal needle ls lnserLed
beLween Lhe lumbar verLebrae L3/L4 or L4/L3 and pushed ln
unLll Lhere ls a "glve" LhaL lndlcaLes Lhe needle ls pasL Lhe
llgamenLum flavum. 1he needle ls agaln pushed unLll Lhere ls
a second 'glve' LhaL lndlcaLes Lhe needle ls now pasL Lhe dura
maLer.
Norma| 8acter|a| V|ra| Iunga|]18
Color clear cloudy Clear/cloudy xanLhochromlc
Clucose 43-73
mg/dl
normal
roLeln 13-43
mg/dl
Marked
Mild Mild
Cell
counL
<6
lymph
o
PMN lympho Lympho,
Al8 sLaln
ressure 80-180
mmPg
200-300
normal/
Mild
normal/
Mild
10. Neurotransm|tter
Norep|nephr|ne, ep|nephr|ne, and dopam|ne
(1) Norep|nephr|ne
a. prlmary LransmlLLer released from
posLgangllonlc sympaLheLlc neurons.
b. synLheslzed ln Lhe nerve Lermlnal and released
lnLo Lhe synapse Lo blnd wlLh or recepLors
on Lhe posLsynapLlc membrane.
c. removed from Lhe synapse by reupLake or ls
meLabollzed ln Lhe presynapLlc Lermlnal by
monoamlne oxldase (MAC) and caLechol-C-
meLhylLransferase (CCM1). 1he meLabollLes are:
l. 3,4-ulhydroxymandellc acld (uCMA)
ll. normeLanephrlne (nMn)
lll. 3-MeLhoxy-4-hydroxyphenylglycol (MCLC)
lv. 3-MeLhoxy-4-hydroxymandellc acld, or
vanlllylmandellc acld (vMA)
d. ln pheochromocyLoma, a Lumor of Lhe adrenal
medulla LhaL secreLes caLecholamlnes, urlnary
excreLlon of vMA ls lncreased.
(2) Lp|nephr|ne
a. synLheslzed from noreplnephrlne by Lhe acLlon
of phenyleLhanolamlne-nmeLhylLransferase.
b. secreLed, along wlLh noreplnephrlne, from Lhe
adrenal medulla.
(3) Dopam|ne
a. promlnenL ln mldbraln neurons.
b. released from Lhe hypoLhalamus and lnhlblLs
prolacLln secreLlon, ln Lhls conLexL lL ls called
prolacLln-lnhlblLlng facLor (ll).
c. meLabollzed by MAC and CCM1
l. u1 recepLors acLlvaLe adenylaLe cyclase vla a
Cs proLeln.
ll. u2 recepLors lnhlblL adenylaLe cyclase vla a Cl
proLeln.
lll. Parkinsons disease lnvolves degeneraLlon of
dopamlnerglc neurons LhaL use Lhe u2
recepLors.
lv. Schlzophrenla lnvolves lncreased levels of u2
recepLors.
Seroton|n
(1) presenL ln hlgh concenLraLlons ln Lhe braln sLem.
(2) formed from LrypLophan.
(3) converLed Lo melaLonln ln Lhe plneal gland.
n|stam|ne
(1) formed from hlsLldlne.
(2) presenL ln Lhe neurons of Lhe hypoLhalamus.
G|utamate
(1) mosL prevalenL exclLaLory neuroLransmlLLer ln Lhe
braln.
(2) 1here are four subLypes of gluLamaLe recepLors.
(3) 1hree subLypes are lonoLroplc recepLors (llgand-
gaLed lon channels) lncludlng Lhe nMuA (!-meLhyl-
u-asparLaLe) recepLor.
(4) Cne subLype ls a meLaboLroplc recepLor, whlch ls
coupled Lo lon channels vla a heLero-Lrlmerlc C
proLeln.
GA8A
(1) an lnhlblLory neuroLransmlLLer
(2) synLheslzed from gluLamaLe by gluLamaLe
decarboxylase.
(3) Lwo Lypes of recepLors:
a. 1he CA8AA recepLor lncreases Cl conducLance
and ls Lhe slLe of acLlon of benzodlazeplnes and
barblLuraLes.
b. 1he CA8A8 recepLor lncreases k+ conducLance.
G|yc|ne
(1) an lnhlblLory neuroLransmlLLer found prlmarlly ln Lhe
splnal cord and braln sLem.
(2) lncreases Cl conducLance.
N|tr|c ox|de (NC)
(1) shorL-acLlng lnhlblLory neuroLransmlLLer ln Lhe
gasLrolnLesLlnal LracL, blood vessels, and Lhe cenLral
nervous sysLem.
(2) synLheslzed ln presynapLlc nerve Lermlnals, where
nC synLhase converLs arglnlne Lo clLrulllne and nC.
(3) a permeanL gas LhaL dlffuses from Lhe presynapLlc
Lermlnal Lo lLs LargeL cell.
(4) also funcLlons ln slgnal LransducLlon of guanylyl
cyclase ln a varleLy of Llssues, lncludlng vascular
smooLh muscle.
11. C|rc|e of W||||s
1he Clrcle of Wlllls ls composed of Lhe followlng arLerles:
AnLerlor cerebral arLery (lefL and rlghL)
AnLerlor communlcaLlng arLery
lnLernal caroLld arLery (lefL and rlghL)
osLerlor cerebral arLery (lefL and rlghL)
osLerlor communlcaLlng arLery (lefL and rlghL)
1he basllar arLery and mlddle cerebral arLerles, supplylng Lhe
braln, are also consldered parL of Lhe clrcle.
12. a|n pathway
er|phera| pa|n orlglnaLes ln muscles, Lendons, eLc., or ln Lhe
perlpheral nerves Lhemselves. aln orlglnaLlng ln Lhe
perlpheral nerves, l.e. vla Lrauma Lo Lhe nerves, ls neurogenlc
paln. Centra| pa|n arlses from cenLral nervous sysLem
paLhology, a "prlmary" CnS dysfunLlon.
Noc|cept|ve paln ls paln ln whlch normal nerves LransmlL
lnformaLlon Lo Lhe cenLral nervous sysLem abouL Lrauma
Lo Llssues (nocere = Lo ln[ure, LaLln).
Neuropath|c paln ls paln ln whlch Lhere are sLrucLural
and/or funcLlonal nervous sysLem adapLaLlons secondary
Lo ln[ury, LhaL Lake place elLher cenLrally or perlpherally
(!ensen, 1996). Much of whaL has prevlously been
consldered psychogenlc paln ls now beLLer undersLood as
neuropaLhlc paln of cenLral orlgln. 1he lAS
deflnes cenLral paln as "paln lnlLlaLed or caused by
a prlmary leslon or dysfuncLlon ln Lhe cenLral nervous
sysLem" (Merskey, and 8ogduk, 1994). "neuropaLhlc"
should noL be confused wlLh "neurogenlc", a Lerm used
Lo descrlbe paln resulLlng from ln[ury Lo a perlpheral
nerve buL wlLhouL necessarlly lmplylng any "neuropaLhy"
1he sp|notha|am|c pathway crosses Lhe mldllne and
ascends on Lhe oppos|te s|de of Lhe splnal cord Lo Lhe
venLral posLerolaLeral nucleus of Lhe Lhalamus. 1hls
nucleus ls subdlvlded for speclflc areas of Lhe body, and
each area pro[ecLs Lo lLs own secLlon of Lhe prlmary
sensory corLex -- a Lhln band of corLex ln Lhe parleLal lobe
[usL posLerlor Lo Lhe cenLral sulcus.
1hls dlscrlmlnaLlve paLhway LransmlLs Lo conclousness
preclse lnformaLlon abouL Lhe locaLlon of paln.
1he sp|noret|cu|ar pathway ascends on both s|des of Lhe
splnal cord Lo Lhe lnLralamlnar nuclel of boLh Lhe rlghL
and lefL Lhalamus. lrom Lhere Lhe nexL neuron ln Lhe
chaln Lakes Lhe lnformaLlon Lo many areas of Lhe braln,
e.g., Lhe anLerlor parL of Lhe clngulaLe gyrus ( emoLlon ),
Lhe amygdala ( memory and emoLlon ), and
hypoLhalamus ( emoLlon and Lhe vascular response Lo
emoLlon ).
1he dorsa| co|umn pathway has long been suspecLed of
LransmlLLlng vlsceral noclcepLlon Lo Lhe Lhalamus (as well
as somaLlc Louch and poslLlon sense). now Lhls ls known
Lo be so (Plrshberg, eL al, 1996 ).
13. 8en|gn febr||e se|zures
lebrlle convulslons, Lhe mosL common selzure dlsorder
durlng chlldhood, generally have an excellenL prognosls buL
may also slgnlfy a serlous underlylng acuLe lnfecLlous dlsease
such as sepsls or bacLerlal menlnglLls. 1herefore, each chlld
wlLh a selzure assoclaLed wlLh fever musL be carefully
examlned and approprlaLely lnvesLlgaLed for Lhe cause of Lhe
fever especlally when lL ls Lhe 1sL selzure. lebrlle selzures are
age dependenL and are rare before 9 mo and afLer 3 yr of
age. The peak age of onset is 1418 mo of age, and Lhe
lncldence approaches 34 of young chlldren. A sLrong famlly
hlsLory of febrlle convulslons ln slbllngs and parenLs suggesLs
a geneLlc predlsposlLlon. Llnkage sLudles ln several large
famllles have mapped Lhe febrlle selzure gene Lo
chromosomes 19p and 8q1321. An auLosomal domlnanL
lnherlLance paLLern ls demonsLraLed ln some famllles.
A slmple febrlle convulslon ls usually assoclaLed wlLh a core
temperature that increases rapidly to 39C. It is initially
generallzed and Lonlc-clonlc ln naLure, lasLs a few seconds
and rarely up Lo 13 mln, ls followed by a brlef posLlcLal perlod
of drowslness, and occurs only once ln 24 hr. A febrlle selzure
ls descrlbed as complex or compllcaLed when Lhe duraLlon ls
>13 mln, when repeaLed convulslons occur wlLhln 24 hr, or
when focal selzure acLlvlLy or focal flndlngs are presenL durlng
Lhe posLlcLal perlod. Convulslve sLaLus epllepLlcus (one
selzure lasLlng 30 mln or mulLlple selzures durlng 30 mln
wlLhouL regalnlng consclousness) ls ofLen due Lo cenLral
nervous sysLem lnfecLlon (vlral or bacLerlal menlnglLls).
ApproxlmaLely 3030 of chlldren have recurrent se|zures
wlLh laLer eplsodes of fever and a small mlnorlLy has
numerous recurrenL febrlle selzures. lacLors assoclaLed wlLh
lncreased recurrence rlsk lnclude age <12 mo, lower
LemperaLure before selzure onseL, a poslLlve famlly hlsLory of
febrlle selzures, and complex feaLures. lebrlle selzures are
noL assoclaLed wlLh reducLlon ln laLer lnLellecLual
performance, and mosL chlldren wlLh febrlle selzures have
only a sllghLly greaLer rlsk of laLer epllepsy Lhan Lhe general
populaLlon. 1he rlsk of epllepsy ls much hlgher Lhan ln Lhe
general populaLlon ln chlldren wlLh one or more complex
febrlle selzures, especlally lf Lhe selzures are focal ln chlldren
wlLh an underlylng neurologlc dlsorder. 1he lncldence of
epllepsy ls >9 when several rlsk facLors are presenL,
compared wlLh an lncldence of 1 ln chlldren who have
febrlle convulslons and no rlsk facLors.
8ouLlne managemenL of a normal lnfanL wlLh slmple brlef
febrlle convulslons lncludes a careful search for Lhe cause of
Lhe fever and reassurance and educaLlon of Lhe parenLs.
AlLhough anLlpyreLlcs have noL been shown Lo prevenL
selzure recurrences, acLlve measures Lo conLrol Lhe fever,
lncludlng Lhe use of anLlpyreLlcs, may reduce dlscomforL and
are reassurlng. ln a seLLlng where supporL for venLllaLlon can
be provlded, conslderaLlon should be glven Lo LreaLlng
selzures lasLlng >3 mln wlLh a benzodlazeplne as a flrsL-llne
Lherapy. henobarblLal prevenLs recurrenL febrlle selzures
buL may also decrease cognlLlve funcLlon ln LreaLed chlldren
compared wlLh unLreaLed chlldren. Sodlum valproaLe ls also
effecLlve for prevenLlon of febrlle selzures, buL Lhe poLenLlal
rlsks of Lhe drug do noL [usLlfy lLs use ln a dlsorder wlLh an
excellenL prognosls regardless of LreaLmenL. 1he lncldence of
faLal valproaLe-lnduced hepaLoLoxlclLy ls hlghesL ln chlldren
<2 yr of age.
14. Substance abuse d|sorder
WP? uC LCLL A8uSL u8uCS?
CeneLlcs
ersonallLy roflle
LnvlronmenL
neuroblology
CLher facLors
Genet|cs
a. SLrongesL geneLlc lnfluences on Lhe rlsk of drug
abuse are Lhe SAML genes LhaL lnfluence lnlLlaLlon of
drug use.
b. Cnce drug use ls lnlLlaLed, Lhe facLors LhaL lnfluence
Lhe LranslLlon from lnlLlaLlon Lo repeaLed use, abuse,
or dependence are largely nCn CLnL1lC unlque Lo
each lndlvldual.
ersonallLy AnLecedenL
a. Antisocial personality traits in a persons biological
parenLs predlcL an lncreased rlsk of early-onseL
alcohol and subsLance abuse.
b. Antisocial personality traits in a persons own
chlldhood and adolescence predlcL early onseL of
subsLance abuse.
Pyperdopamlnerglc acLlvlLy of Lhe mesollmblc paLhway
lnduces poslLlve sympLoms of psychosls.
c. PosLlllLy - exclLemenL
d. ueluslons - susplclousness
e. PalluclnaLlons -concepLual dlsorganlzaLlon
f. CrandloslLy
lacLors LhaL Lrlgger mesollmblc dopamlne neurons Lo release
dopamlne.
Natural Highs Drug-induced high
Lndorphlns morphlne/heroln
Anandamlde marl[uana
AceLylchollne nlcoLlne
uopamlne cocalne and ampheLamlne
St|mu|ants
8elnforclng properLles of cocalne and ampheLamlne are
assoclaLed wlLh Lhelr lncrease synapLlc uA levels
Coca|ne lncreases synapLlc uA by blndlng Lo uA1 and
lnhlblLlng lLs acLlvlLy.
Amphetam|ne lncreases synapLlc uA by acLlons on
veslcular monoamlne LransporLer causes release of
uA.
Cocalne and ampheLamlne also have acLlons on nL
and 3-P1 neurons, and all of Lhese
neuroLransmlLLers are lmporLanL LargeLs for
medlcaLlon developmenL.
Slgns/SympLoms of SLlmulanL lnLoxlcaLlon
1achycardla or bradycardla
ullaLed puplls
LlevaLed or low blood pressure
SweaLlng or chllls
nausea or vomlLlng
Lvldence of welghL loss
sychomoLor aglLaLlon or reLardaLlon
Muscle weakness, resplraLory depresslon, chesL
paln, cardlac arrhyLhmla
Confuslon, selzures, dysklneslas, dysLonlas, coma
1reaLmenL for SLlmulanL lnLoxlcaLlon
Medlcal and psychlaLrlc sLablllzaLlon
uellrlum of selzure conLrol
8esplraLory supporL and conLrol of blood pressure,
LemperaLure, arrhyLhmlas
ConLrol of aglLaLlon, aggresslveness, and paranold
psychosls
.. Acute cocaine toxicity typically subsides within 1 to 2
hours, whereas ampheLamlne LoxlclLy may perslsL for several
hours.
Cannabls SaLlva (Marl[uana)
Smoked Lo dellver psychoacLlve subsLances
cannablnolds especlally 1PC delLa-9-
LeLrahydrocannablnol
THC interact with brains own cannabinoid receptor
(C81) Lo Lrlgger dopamlne release from Lhe
mesollmblc reward sysLem
LffecL ln Lhe body ls cenLered malnly ln Lhe CnS
! lncreased sense of well-belng and euphorla
! lmpalred shorL Lerm memory
! deLerloraLlon ln Lhe capaclLy Lo carry ouL Lasks
LhaL requlre mulLlple menLal sLeps Lo reach a
speclflc goal temporal disintegration
1S. Sch|zophren|a
Mlmlcs neurodegeneraLlve dlsorder
Schlzophrenlc braln: mlsplaced, mls-slzed and
dlsorganlzed
uopamlne hypoLhesls
! Pyperdopamlnerglc sLaLe ln subcorLlcal area may
underlle Lhe poslLlve sympLoms of schlzophrenla
! 1reaLmenL became humanlzed, asylum
! 1reaLmenL wlLh chlorpromazlne or phenoLhlazlne:
paLlenLs wlLh schlzophrenla became quleL and
slepL
! Llmblc sysLem
arL of Lhe braln whlch conLrols behavlor
SeaL of emoLlons
uesLrucLlon ln llmblc causes
ulsLurbance ln emoLlon
ulsLurbance ln percepLlon (ueluslon,
PalluclnaLlon)
ulsLurbance ln Lhlnklng (aranold)
uepersonallzaLlon (aLlenL became
someone she was noL before)
1hese dlsLurbances were due Lo a
chemlcal dlsLurbance: uopamlne ln Lhe
llmblc sysLem
Chlorpromazlne: AnLl-dopamlne
2 1ypes of Schlzophrenla
! oslLlve sympLoms: 1ype 1
! negaLlve sympLoms: 1ype 2
uSM-lv CrlLerla
! aranold
reoccupaLlon wlLh one or more deluslons
or frequenL audlLory halluclnaLlons
none of Lhe followlng ls promlnenL:
dlsorganlzed speech, dlsorganlzed or
caLaLonlc behavlor, or flaL or lnapproprlaLe
affecL
! CaLaLonlc (aL leasL 2 of Lhe ff)
MoLorlc lmmoblllLy as evldenced by
caLalepsy (lncludlng waxy flexlblllLy) or
sLupor
Lxcesslve moLor ablllLy (LhaL ls apparenLly
purposeless and noL lnfluenced by exLernal
sLlmull)
LxLreme negaLlvlsm (an apparenLly
moLlveless reslsLance Lo all lnsLrucLlons or
malnLenance of a rlgld posLure agalnsL
aLLempLs Lo be moved) or muLlsm
ecullarlLles of volunLary movemenL as
evldenced by posLurlng (volunLary
assumpLlon of lnapproprlaLe or blzarre
posLures), sLereoLyped movemenLs,
promlnenL mannerlsms, or promlnenL
grlmaclng
Lcholalla or echopraxla
! ulsorganlzed
All of Lhe followlng are promlnenL:
dlsorganlzed speech, dlsorganlzed behavlor,
flaL or lnapproprlaLe affecL
1he crlLerla are noL meL for caLaLonlc Lype
! undlfferenLlaLed
SympLoms ln CrlLerlon A are presenL buL Lhe
crlLerla are noL meL for paranold,
dlsorganlzed, or caLaLonlc behavlor
! 8esldual Lype
Absence of promlnenL deluslons,
halluclnaLlons, dlsorganlzed speech, and
grossly dlsorganlzed or caLaLonlc behavlor
1here ls conLlnulng evldence of Lhe
dlsLurbance
16. CC d|sorder
Anal personallLy
LmoLlonal consLrlcLlon
ervaslve paLLern of lnflexlblllLy
Crderllness, perseverance, sLubborness
lnslsL LhaL rules be followed rlgldly
lnLolerance for mlsLakes
AnxleLy over upseLLlng Lhe rouLlne (Perfectionist)
1hese paLlenLs are aL lncreased rlsk for ma[or
depresslon, anxleLy dlsorder, and obsesslve-
compulslve dlsorder.
Lpldemlology
1 percenL ln Lhe general populaLlon
3 Lo 10 percenL for psychlaLrlc ouLpaLlenLs
M>l
LLlology
Cbsesslons and compulslons have been repeaLedly
llnked Lo hlgh cenLral seroLonerglc funcLlon.
Powever, Lhe laLLer ls assoclaLed wlLh anxleLy ln
general, whlch supporLs Lhe hypoLhesls LhaL
obsesslons and compulslons represenL psychologlcal
and behavloral mechanlsms agalnsL anxleLy.
ClasslflcaLlon
A pervaslve paLLern of preoccupaLlon wlLh orderllness,
perfecLlonlsm, and menLal and lnLerpersonal conLrol, aL Lhe
expense of flexlblllLy, openness, and efflclency, beglnnlng by
early adulLhood and presenL ln a varleLy of conLexLs, as
lndlcaLed by four (or more) of Lhe followlng:
(1) ls preoccupled wlLh deLalls, rules, llsLs, order,
organlzaLlon, or schedules Lo Lhe exLenL LhaL Lhe ma[or
polnL of Lhe acLlvlLy ls losL
(2) shows perfecLlonlsm LhaL lnLerferes wlLh Lask
compleLlon (e.g., ls unable Lo compleLe a pro[ecL because
hls or her own overly sLrlcL sLandards are noL meL)
(3) ls excesslvely devoLed Lo work and producLlvlLy Lo Lhe
excluslon of lelsure acLlvlLles and frlendshlps (noL
accounLed for by obvlous economlc necesslLy)
(4) ls overconsclenLlous, scrupulous, and lnflexlble abouL
maLLers of morallLy, eLhlcs, or values (noL accounLed for
by culLural or rellglous ldenLlflcaLlon)
(3) ls unable Lo dlscard worn-ouL or worLhless ob[ecLs
even when Lhey have no senLlmenLal value
(6) ls relucLanL Lo delegaLe Lasks or Lo work wlLh oLhers
unless Lhey submlL Lo exacLly hls or her way of dolng
Lhlngs
(7) adopLs a mlserly spendlng sLyle Loward boLh self and
oLhers, money ls vlewed as someLhlng Lo be hoarded for
fuLure caLasLrophes
(8) shows rlgldlLy and sLubbornness
Spec|a| Senses
1. r|nc|p|es of accommodat|on
AccommodaLlon ls Lhe process by whlch Lhe eye changes
opLlcal power Lo malnLaln a clear lmage (focus) on an ob[ecL
as lLs dlsLance changes. 1he young human eye can change
focus from dlsLance Lo 7 cm from Lhe eye ln 330 mllllseconds.
1hls dramaLlc change ln focal power of Lhe eye of
approxlmaLely 12 dlopLers (a dlopLer ls 1 dlvlded by Lhe focal
lengLh ln meLers) occurs as a consequence of a reducLlon
ln zonular Lenslon lnduced by clllary muscle conLracLlon. 1he
ampllLude of accommodaLlon decllnes wlLh age. 8y Lhe flfLh
decade of llfe Lhe accommodaLlve ampllLude has decllned so
Lhe near polnL of Lhe eye ls more remoLe Lhan Lhe readlng
dlsLance. When Lhls occurs Lhe paLlenL ls presbyoplc. When
someone accommodaLes Lo a near ob[ecL, Lhey
also converge Lhelr eyes and consLrlcL Lhelr puplls. 1he
comblnaLlon of Lhese Lhree movemenLs (accommodaLlon,
convergence and mlosls) ls under Lhe conLrol of Lhe Ldlnger-
WesLphal nucleus and ls referred Lo as Lhe "#$% '%($).
AlLhough, lL ls clear LhaL convergence allows Lo focus Lhe
ob[ecL's lmage on Lhe reLlna, Lhe funcLlonal role of Lhe
puplllary conLracLlon remalns less clear. Arguably, lL may
lncrease Lhe depLh of fleld by reduclng Lhe aperLure of Lhe
eye, and Lhus reduce Lhe amounL of accommodaLlon needed
Lo brlng Lhe lmage ln focus on Lhe reLlna.
2. Waldeyers ring
Wa|deyer's tons|||ar r|ng (or pharyngea| |ympho|d r|ng) ls an
anaLomlcal Lerm descrlblng Lhe lymphold Llssue rlng locaLed
ln Lhe pharynx and Lo Lhe back of Lhe oral cavlLy.
1he rlng conslsLs of (from superlor Lo lnferlor):
haryngeal Lonsll (also known as 'adenolds' when
lnfecLed)
1ubal Lonsll (where Lhe LusLachlan Lube opens ln Lhe
nasopharynx)
alaLlne Lonslls (commonly called "Lhe Lonslls" ln Lhe
vernacular, less commonly Lermed "fauclal Lonslls")
Llngual Lonslls
3. athway of tear|ng
1ears are secreLlons LhaL clean and lubrlcaLe Lhe eyes. 1he
Lear fllm coaLlng Lhe eye, known as Lhe precorneal fllm, has
Lhree dlsLlncL layers, from Lhe mosL ouLer surface:
Name Conta|ns Secreted by Iunct|ons
Llpld
layer
Clls
Melbomlan
gland
coaLs Lhe aqueous layer,
provldes
a hydrophoblc barrler
LhaL evaporaLes and
prevenLs Lears from
spllllng onLo Lhe cheek.
Aqueous
layer
WaLer
Lacrlmal
gland
promoLes spreadlng of
Lhe Lear fllm, promoLes
Lhe conLrol of lnfecLlous
agenLs, promoLes
osmoLlc regulaLlon
Mucus
layer
Mucln
Con[uncLlval
gobleL cells
coaLs
Lhe cornea,provldes
a hydrophlllc layer,allows
for even dlsLrlbuLlon of
Lhe Lear fllm, covers Lhe
cornea
1he lacrlmal glands secreLe lacrlmal fluld, whlch flows
Lhrough Lhe maln excreLory ducLs lnLo Lhe space beLween Lhe
eyeball and llds. When Lhe eyes bllnk, Lhe lacrlmal fluld ls
spread across Lhe surface of Lhe eye. Lacrlmal fluld gaLhers ln
Lhe lacrlmal lake, and ls drawn lnLo Lhe puncLa by caplllary
acLlon, Lhen flows Lhrough Lhe lacrlmal canallcull aL Lhe lnner
corner of Lhe eyellds enLerlng Lhe lacrlmal sac, Lhen on Lo
Lhe nasolacrlmal ducL, and flnally lnLo Lhe nasal cavlLy.
4. V|sua| pathway
vlslon ls generaLed by phoLorecepLors ln Lhe reLlna, a layer of
cells aL Lhe back of Lhe eye. 1he lnformaLlon leaves Lhe eye by
way of Lhe opLlc nerve, and Lhere ls a parLlal crosslng of axons
aL Lhe opLlc chlasm. AfLer Lhe chlasm, Lhe axons are called
Lhe opLlc LracL. 1he opLlc LracL wraps around Lhe mldbraln Lo
geL Lo Lhe laLeral genlculaLe nucleus (LCn), where all Lhe
axons musL synapse. lrom Lhere, Lhe LCn axons fan ouL
Lhrough Lhe deep whlLe maLLer of Lhe braln as Lhe opLlc
radlaLlons, whlch wlll ulLlmaLely Lravel Lo prlmary vlsual
corLex, aL Lhe back of Lhe braln.
S. Aud|tory pathway
1hls sound lnformaLlon Lravels down Lhe vesLlbulocochlear
nerve Lhrough lnLermedlaLe sLaLlons such as Lhe cochlear
nuclel and superlor ollvary complex of Lhe bralnsLem and
Lhe lnferlor colllculus of Lhe mldbraln, belng furLher
processed aL each waypolnL. 1he lnformaLlon evenLually
reaches Lhe Lhalamus, and from Lhere lL ls relayed Lo Lhe
corLex. ln Lhe human braln, Lhe prlmary audlLory corLex ls
locaLed ln Lhe Lemporal lobe.
AssoclaLed anaLomlcal sLrucLures lnclude:
Coch|ear nuc|eus
1he cochlear nucleus ls Lhe flrsL slLe of Lhe neuronal
processing of the newly converted digital data from the
lnner ear. 1hls reglon ls anaLomlcally and physlologlcally spllL
lnLo Lwo reglons, Lhe dorsal cochlear nucleus (uCn),
and venLral cochlear nucleus (vCn).
1rapezo|d body
1he 1rapezold body ls a bundle of decussaLlng flbers ln Lhe
venLral pons LhaL carry lnformaLlon used for blnaural
compuLaLlons ln Lhe bralnsLem.
Super|or o||vary comp|ex
1he superlor ollvary complex ls locaLed ln Lhe pons, and
recelves pro[ecLlons predomlnanLly from Lhe venLral cochlear
nucleus, alLhough Lhe posLerlor cochlear nucleus pro[ecLs
Lhere as well, vla Lhe venLral acousLlc sLrla. WlLhln
Lhe superlor ollvary complex lles Lhe laLeral superlor ollve
(LSC) and Lhe medlal superlor ollve (MSC). 1he former ls
lmporLanL ln deLecLlng lnLeraural level dlfferences whlle Lhe
laLLer ls lmporLanL ln dlsLlngulshlng lnLeraural Llme dlfference.
Latera| |emn|scus
1he laLeral lemnlscus ls a LracL of axons ln Lhe bralnsLem LhaL
carrles lnformaLlon abouL sound from Lhe cochlear nucleus Lo
varlous bralnsLem nuclel and ulLlmaLely Lhe
conLralaLeral lnferlor colllculus of Lhe mldbraln.
Infer|or co|||cu||
1he lC are locaLed [usL below Lhe vlsual processlng cenLers
known as Lhe superlor colllcull. 1he cenLral nucleus of Lhe lC
ls a nearly obllgaLory relay ln Lhe ascendlng audlLory sysLem,
and mosL llkely acLs Lo lnLegraLe lnformaLlon (speclflcally
regardlng sound source locallzaLlon from Lhe superlor ollvary
complex and dorsal cochlear nucleus) before sendlng lL Lo Lhe
Lhalamus and corLex
Med|a| gen|cu|ate nuc|eus
1he medlal genlculaLe nucleus ls parL of Lhe Lhalamlc relay
sysLem.
r|mary aud|tory cortex
1he prlmary audlLory corLex ls Lhe flrsL reglon of cerebral
corLex Lo recelve audlLory lnpuL.
ercepLlon of sound ls assoclaLed wlLh Lhe rlghL
posLerlor superlor Lemporal gyrus (S1C). 1he superlor
Lemporal gyrus conLalns several lmporLanL sLrucLures of Lhe
braln, lncludlng 8rodmann areas 41 and 42, marklng Lhe
locaLlon of Lhe prlmary audlLory corLex, Lhe corLlcal reglon
responslble for Lhe sensaLlon of baslc characLerlsLlcs of sound
such as plLch and rhyLhm.
1he audlLory assoclaLlon area ls locaLed wlLhln Lhe Lemporal
lobe of Lhe braln, ln an area called Lhe Wernlcke's area, or
area 22. 1hls area, near Lhe laLeral cerebral sulcus, ls an
lmporLanL reglon for Lhe processlng of acousLlc slgnals so LhaL
Lhey can be dlsLlngulshed as speech, muslc, or nolse.
6. S|nuses
aranasa| s|nuses are a group of four palred alr-fllled
spaces LhaL surround Lhe nasal cavlLy (maxlllary slnuses),
above and beLween Lhe eyes (eLhmold slnuses and fronLal
slnuses), and behlnd Lhe eLhmolds (sphenold slnuses). 1he
slnuses are named for Lhe faclal bones behlnd whlch Lhey are
locaLed.
max|||ary s|nuses, also called Lhe maxlllary anLrechea
and Lhe largesL of Lhe paranasal slnuses, are under
Lhe eyes, ln Lhe maxlllary bones.
fronta| s|nunes, superlor Lo Lhe eyes, ln Lhe fronLal bone,
whlch forms Lhe hard parL of Lhe forehead.
ethmo|d s|nuses, whlch are formed from several dlscreLe
alr cells wlLhln Lhe eLhmold bone beLween Lhe nose and
Lhe eyes.
spheno|d s|nuses, ln Lhe sphenold bone aL Lhe cenLer of
Lhe skull base under Lhe plLulLary gland.
1he paranasal alr slnuses are llned wlLh resplraLory
eplLhellum (clllaLed pseudosLraLlfled columnar eplLhellum).
Iunct|ons:
uecreaslng Lhe relaLlve welghL of Lhe fronL of Lhe
skull, and especlally Lhe bones of Lhe face.
lncreaslng resonance of Lhe volce.
rovldlng a buffer agalnsL blows Lo Lhe face.
lnsulaLlng senslLlve sLrucLures llke denLal rooLs and
eyes from rapld LemperaLure flucLuaLlons ln Lhe
nasal cavlLy.
Pumldlfylng and heaLlng of lnhaled alr because of
slow alr Lurnover ln Lhls reglon.
7. ap|||edema vs. pap||||t|s
ap|||edema ap||||t|s
1. non-lnflammaLory
congesLlon of opLlc
dlsk
2. lnLracranlal pressure
3. lnLacL vlsual fleld
excepL for an enlarged
bllnd spoL
4. 8llaLeral
3. 1akes 24-46 hours for
early papllledema Lo
occur and 1 week Lo
fully develop
6. 6-8wks Lo resolve
7. vlsual loss can occur
afLer sudden decrease
ln lC
1. lnflammaLlon wlLh
demyellnaLlon of opLlc
nerve
2. Cardlnal sx: vlslon loss
few hrs afLer onseL
3. unllaLeral
4. ulsk swelllng caused
by lnflammaLlon aL Lhe
nerve head
Cllnlcal manlfesLaLlon:
1/3 have vlslon beLLer
Lhan 20/40 lnlLlally
>1/3 have vlslon worse
LhaL 20/200
aln wlLh eye movemenL
vlslon lmproves wlLhln 2-
6wks
CenLral scoLomas
Slugglsh paplllary llghL
reflex
CphLhalmoscopy:
Pyperemla of Lhe opLlc
dlsc
8lurrlng of perlpaplllary
dlsc margln
Loss of sponLaneous
venous pulsaLlons
CphLhalmoscopy:
Pyperemla of opLlc dlsc
(early)
ulsLenLlon of large velns
8lurred dlsc marglns and
fllllng of physlologlc cup
llame-shaped
hemorrhages ln Lhe nerve
layer near opLlc dlsc
1reaLmenL:
1reaL underlylng cause
L
ulureLlcs
CorLlcosLerolds
LumboperlLoneal shunL
lenesLraLlon of opLlc
nerve sheaLh
1reaLmenL:
meLhyprednlsolone
8. Ccu|ar hypertens|on
Ccular hyperLenslon ls lnLraocular pressure hlgher Lhan
normal ln Lhe absence of opLlc nerve damage or vlsual
fleld loss. normal lnLraocular pressure (lC) ls deflned
as LhaL beLween 10 mmPg and 21 mmPg. LlevaLed lC
ls Lhe mosL lmporLanL rlsk facLor for glaucoma, so Lhose
wlLh ocular hyperLenslon are frequenLly consldered Lo
have a greaLer chance of developlng Lhe condlLlon.
lnLraocular pressure ls malnly malnLalned by Lhe
llquld aqueous humor, whlch ls produced by Lhe clllary
body of Lhe eye. Aqueous humor normally does noL go
lnLo Lhe posLerlor segmenL of Lhe eye, lL ls kepL ouL of
Lhls area by Lhe lens and Lhe Zonule of Zlnn. lnsLead, lL
sLays only ln Lhe anLerlor segmenL, whlch ls dlvlded lnLo
Lhe anLerlor and posLerlor chambers. 1he anLerlor and
posLerlor chambers are boLh parLs of Lhe anLerlor
segmenL, whlch ls an lmporLanL dlsLlncLlon Lo make ln
Lhe undersLandlng of Lhe Lwo maln mechanlsms of
ocular hyperLenslon.
When Lhe clllary bodles produce Lhe aqueous humor, lL
flrsL flows lnLo Lhe posLerlor chamber (bounded by Lhe
lens and Lhe lrls). lL Lhen flows Lhrough Lhe pupll of Lhe
lrls lnLo Lhe anLerlor chamber (bounded by Lhe lrls and
Lhe cornea). lrom here, lL flows Lhrough a sLrucLure
known as Lhe Lrabecular meshwork Lo enLer Lhe normal
body clrculaLlon. 1hus, Lhe Lwo maln mechanlsms of
ocular hyperLenslon are an lncreased producLlon of
aqueous humor, or a decreased ouLflow of aqueous
humor.
9. Layers of ret|na
lrom closesL Lo farLhesL from Lhe vlLreous body - LhaL ls, from
closesL Lo Lhe fronL exLerlor of Lhe head Lowards Lhe lnLerlor
and back of Lhe head:
1. lnner llmlLlng membrane Muller cell fooLplaLes
2. nerve flber layer axons of Lhe gangllon cell nuclel
3. Cangllon cell layer conLalns nuclel of gangllon cells,
Lhe axons of whlch become Lhe opLlc nerve flbers
for messages
4. lnner plexlform layer conLalns Lhe synapse
beLween Lhe blpolar cell axons and Lhe dendrlLes of
Lhe gangllon and amacrlne cells
3. lnner nuclear layer conLalns Lhe nuclel and
surroundlng cell bodles (perlkarya) of Lhe blpolar
cells
6. CuLer plexlform layer pro[ecLlons of rods and
cones endlng ln Lhe rod spherule and cone pedlcle,
respecLlvely. 1hese make synapses wlLh dendrlLes of
blpolar
[1]
ln Lhe macular reglon, Lhls ls known as
Lhe llber layer of Penle.
7. CuLer nuclear layer cell bodles of rods and cones
8. LxLernal llmlLlng membrane layer LhaL separaLes
Lhe lnner segmenL porLlons of Lhe phoLorecepLors
from Lhelr cell nucleus
9. hoLorecepLor layer rods/cones
10. 8eLlnal plgmenL eplLhellum - slngle layer of cuboldal
cells
10. Layers of cornea
lrom Lhe anLerlor Lo posLerlor Lhe flve layers of Lhe human
cornea are:
Cornea| ep|the||um: a Lhln eplLhellal mulLlcellular Llssue layer
(non-keraLlnlzed sLraLlfled squamous eplLhellum) of fasL-
growlng and easlly regeneraLed cells, kepL molsL wlLh Lears.
lrregularlLy or edema of Lhe corneal eplLhellum dlsrupLs Lhe
smooLhness of Lhe alr-Lear fllm lnLerface, Lhe mosL slgnlflcanL
componenL of Lhe LoLal refracLlve power of Lhe eye, Lhereby
reduclng vlsual aculLy. lL ls conLlnuous wlLh Lhe con[uncLlval
eplLhellum, and ls composed of abouL 6 layers of cells whlch
are shed consLanLly on Lhe exposed layer and are
regeneraLed by mulLlpllcaLlon ln Lhe basal layer.
8owman's |ayer : a Lough layer LhaL proLecLs Lhe corneal
sLroma, malnly Lype l collagen flbrlls. 1hese flbrlls lnLeracL
wlLh and aLLach on Lo each oLher.
Cornea| stroma (also subsLanLla proprla): a Lhlck, LransparenL
mlddle layer, conslsLlng of regularly arranged collagen flbers
along wlLh sparsely dlsLrlbuLed lnLerconnecLed keraLocyLes,
whlch are Lhe cells for general repalr and malnLenance. 1hey
are parallel and are superlmposed llke book pages 1he
corneal sLroma conslsLs of approxlmaLely 200 layers of malnly
Lype l collagen flbrlls. Lach layer ls 1.3-2.5m. Up to 90% of
Lhe corneal Lhlckness ls composed of sLroma.
Descemet's membrane (also posLerlor llmlLlng membrane): a
Lhln acellular layer LhaL serves as Lhe modlfled basemenL
membrane of Lhe corneal endoLhellum, from whlch Lhe cells
are derlved. 1hls layer ls composed malnly of collagen Lype lv
flbrlls, less rlgld Lhan collagen Lype l flbrlls, and ls around 3-
20m thick, depending on the subject's age.
Cornea| endothe||um: a slmple squamous or
low cuboldal monolayer, approx 5m thick, of mitochondria-
rlch cells. 1hese cells are responslble for regulaLlng fluld and
soluLe LransporL beLween Lhe aqueous and corneal sLromal
comparLmenLs. unllke Lhe corneal eplLhellum Lhe cells of Lhe
endoLhellum do noL regeneraLe. lnsLead, Lhey sLreLch Lo
compensaLe for dead cells whlch reduces Lhe overall cell
denslLy of Lhe endoLhellum and has an lmpacL on fluld
regulaLlon. lf Lhe endoLhellum can no longer malnLaln a
proper fluld balance, sLromal swelllng due Lo excess flulds
and subsequenL loss of Lransparency wlll occur and Lhls may
cause corneal edema and lnLerference wlLh Lhe Lransparency
of Lhe cornea and Lhus lmpalrlng Lhe lmage formed.
nematopo|et|c
1. C8C norma| va|ues
normal values
nemog|ob|n 120-170 g]L
nematocr|t 0.37-0.S4
W8C S-10 x 10
9
]L
|ate|ets 1S0-400 x 10
9
]L
Segmenters 0.S0-0.70
Lymphocytes 0.20-0.40
Monocytes 0-0.0S
Los|noph||s 0-0.0S
8and 0-0.03
8lasL cells 0
8eLlculocyLes 0.3-1.3
Mean Corpuscular
volume (MCv)
87 3 +1
Mean Corpuscular
Pemoglobln (MCP)
29 2 pg
MCPC 34 2 g/dL
SCC1 (AS1) 16-40 u/L
SC1 (AL1) 8-33 u/L
1oLal proLeln 6-7.8 g/dL
Albumln 4-3.3 g/dL
Clobulln 1.3-3.4 g/dL
A/C raLlo 1-3 mg/dL
1oLal blllrubln 0.3-1.3 mg/dL
ulrecL blllrubln 0.10-0.40 mg/dL
lndlrecL blllrubln 0.30-1.10 mg/dL
Amylase 10-130 lu/L
Llpase 0-110 lu/L
Alkallne hosphaLase 36-92 lu/L
lasLlng 8lood Sugar
(l8S)
70.9-110 mg/dL
8lood urea nlLrogen
(8un)
9-23 mg/dL
CreaLlnlne 07-1.3 mg/dL
Serum Sodlum 137-147 mLq/L
Serum oLasslum 3.8-3 mLq/L
lonlzed Calclum 1.18-1.30
Serum Magneslum 1.60-2.39
CholesLerol 131-239 mg/dL
1rlglycerldes 3.4-6.2 mg/dL
Plgh uenslLy
LlpoproLeln (PuL)
30-90 mg/dL
Low uenslLy
LlpoproLeln (LuL)
66-178 mg/dL
A11 23-40 sec
1 12-14 sec
2. IVI
1oLal body welghL (608W) = 2/3 lCl + 1/3 lCl
LCl = lnLersLlLlal + x lnLravascular
1l8 = senslble + lnsenslble losses
Senslble sLool (200mL/d), urlne (300-1300mL/d)
lnsenslble skln (300ml/d), resplraLory LracL
(400mL/d), fever(100-130mL/d for every degree
>37)
nypovo|em|a
Comblned salL and waLer loss
1reaLmenL:
Mlld dehydraLlon- oral rehydraLlon
ModeraLe Lo severe- lv hydraLlon wlLh 0.9 naCl lf
normoLremla, 3.0 naCl lf hyponaLremla, 0.43 naCl lf
hypernaLremla
nypervo|em|a
Lxpanslon of lnLersLlLlum edema
lluld composlLlon:
l. Sodlum (n= 133-143 mLq/L)
na deflclL= (deslred acLual) x 0.6 x kg = mmol
` CorrecL only up Lo 13-20 mLq/L/day Lo prevenL
ponLlne myellnolysls
ll. oLasslum (n= 3.3-3.0 mLq/L)
k deflclL= (deslred acLual) x 0.3 x kg = mmol
Cr kg x 30 x esLlmaLed deflclL
3-3.3 3 (abouL 200-400mmol
2-2.9 10
1-1.9 20 (abouL 600mmol)
Pypokalemla LreaLmenL:
lf asympLomaLlc, oral replacemenL
lv replacemenL, 0.2-0.3 mmol/kg/hr
lf perlpheral veln, do noL exceed 40mmol/L
lf cenLral veln, do noL exceed 80mmol/L
**conLlnuous LCC monlLorlng
Pyperkalemla: peaked 1 waves
lf >7.0 mLq/L, prolonged, 8, decreased S1, wlde
C8S.
1reaLmenL: Ca gluconaLe 10 0.3-1.0 ml/kg/L over
10mlns, lnsulln 10-20 u + glucose 25-30g, or naPCC3
3amp/L u3 waLer.
lll. Calclum (n= 4.3-3.1 mg/dL or 1.13-1.28mmol/L)
Pypocalcemla
(+) 1rousseau slgn carpal spasm when 8 cuff ls
lnflaLed above sysLollc pressure for 3mln
(+) ChvosLek slgn LwlLchlng of faclal muscles when
faclal nerve ls Lapped
3. LCI vs ICI
1he 70 kg 'sLandard male' conLalns 42 llLers of waLer - 60 of
hls body welghL. 1he hypoLheLlcal adulL female conLalns 33
of her body welghL as waLer: Lhls lower percenL belng due Lo
a hlgher faL conLenL.
1he varlaLlon beLween lndlvlduals ln Lhe raLlo of 18W Lo
LoLal body welghL ls qulLe large buL Lhe ma[orlLy of Lhe
varlaLlon ls due Lo dlfferenL amounLs of adlpose Llssue.
Cbese adulLs have a lower raLlo. lor any parLlcular Llssue of
Lhe body Lhe varlaLlon ls much less buL any varlaLlon LhaL
occurs ls sLlll mosLly due Lo dlfferences ln amounL of
adlpose Llssue.
Plasma: 93% water (& 7% plasma solids)
laL: 10-13 waLer
8one: 20 waLer
1he waLer ln Lhe body ls conLalned wlLhln Lhe numerous
organs and Llssues of Lhe body. 1hese collecLlons are referred
Lo as comparLmenLs. 1he ma[or dlvlslon ls lnLo lnLracellular
lluld (lCl: abouL 23 llLers) and LxLracellular lluld (LCl: abouL
19 llLers) based on whlch slde of Lhe cell membrane Lhe fluld
lles.
Intrace||u|ar I|u|d
1he lnLracellular lluld ls composed of aL leasL 10
14
separaLe
Llny cellular packages. 1he concepL of a slngle unlLed
"comparLmenL" called lnLracellular fluld ls clearly arLlflclal.
1he lCl comparLmenL ls really a "vlrLual comparLmenL"
consldered as Lhe sum of Lhls huge number of dlsconLlnuous
small collecLlons. 1he reason ls LhaL Lhough noL unlLed
physlcally, Lhe collecLlons have exLremely lmporLanL unlfylng
slmllarlLles whlch make Lhe lCl concepL of pracLlcal
usefulness ln physlology. ln parLlcular, slmllarlLles of
locaLlon, composlLlon and behavlour:
LocaLlon: 1he dlsLlncLlon beLween lCl and LCl ls
clear and ls easy Lo undersLand: Lhey are separaLed
by Lhe cell membranes
ComposlLlon: lnLracellular flulds are hlgh ln
poLasslum and magneslum and low ln sodlum and
chlorlde lons
8ehavlour: lnLracellular flulds behave slmllarly Lo
LonlclLy changes ln Lhe LCl
Lxtrace||u|ar I|u|d
A slmllar argumenL applles Lo Lhe LxLracellular lluld. 1he LCl
ls dlvlded lnLo several smaller comparLmenLs (eg plasma,
lnLersLlLlal fluld, fluld of bone and dense connecLlve Llssue
and Lranscellular fluld). 1hese comparLmenLs are
dlsLlngulshed by dlfferenL locaLlons and dlfferenL klneLlc
characLerlsLlcs. 1he LCl composlLlonal slmllarlLy ls ln some
ways, Lhe opposlLe of LhaL for Lhe lCl (le low ln poLasslum &
magneslum and hlgh ln sodlum and chlorlde).
Interst|t|a| f|u|d (ISI) conslsLs of all Lhe blLs of fluld whlch lle
in the interstices of all body tissues. This is also a virtual
fluld (le lL exlsLs ln many separaLe small blLs buL ls spoken
abouL as Lhough lL was a pool of fluld of unlform
composlLlon ln Lhe one locaLlon). 1he lSl baLhes all Lhe cells
ln Lhe body and ls Lhe llnk beLween Lhe lCl and Lhe
lnLravascular comparLmenL. Cxygen, nuLrlenLs, wasLes and
chemlcal messengers all pass Lhrough Lhe lSl. lSl has Lhe
composlLlonal characLerlsLlcs of LCl (as menLloned above)
buL ln addlLlon lL ls dlsLlngulshed by lLs usually low proLeln
concenLraLlon (ln comparlson Lo plasma). Lymph ls
consldered as a parL of Lhe lSl. 1he lymphaLlc sysLem
reLurns proLeln and excess lSl Lo Lhe clrculaLlon. Lymph ls
more easlly obLalned for analysls Lhan oLher parLs of Lhe lSl.
|asma ls Lhe only ma[or fluld comparLmenL LhaL exlsLs as a
real fluld collecLlon all ln one locaLlon. lL dlffers from lSl ln
lLs much hlgher proLeln conLenL and lLs hlgh bulk flow
(LransporL funcLlon). 8lood conLalns suspended red and
white cells so plasma has been called the interstitial fluid of
the blood. The fluid compartment called Lhe blood volume
ls lnLeresLlng ln LhaL lL ls a composlLe comparLmenL
conLalnlng LCl (plasma) and lCl (red cell waLer).
1he f|u|d of bone & dense connect|ve t|ssue ls slgnlflcanL
because lL conLalns abouL 13 of Lhe LoLal body waLer. 1hls
fluld ls moblllsed only very slowly and Lhls lessens lLs
lmporLance when conslderlng Lhe effecLs of acuLe fluld
lnLervenLlons.
1ransce||u|ar f|u|d ls a small comparLmenL LhaL represenLs
all Lhose body flulds whlch are formed from Lhe LransporL
acLlvlLles of cells. lL ls conLalned wlLhln eplLhellal llned
spaces. lL lncludes CSl, Cl1 flulds, bladder urlne, aqueous
humour and [olnL fluld. lL ls lmporLanL because of Lhe
speclallsed funcLlons lnvolved. 1he fluld fluxes lnvolved wlLh
Cl1 flulds can be qulLe slgnlflcanL. 1he elecLrolyLe
composlLlon of Lhe varlous Lranscellular flulds are qulLe
dlsslmllar and Lyplcal values or ranges for some of Lhese
flulds are llsLed ln Lhe 1able.
1he LoLal body waLer ls dlvlded lnLo comparLmenLs and
useful physlologlcal lnslghL and some measure of cllnlcal
predlcLablllLy can be galned from Lhls approach even Lhough
mosL of Lhese fluld comparLmenLs do noL exlsL as dlscreLe
real fluld collecLlons.
Iunct|ona| LCI
1he waLer ln bone and dense connecLlve Llssue and Lhe
Lranscellular flulds ls slgnlflcanL ln amounL buL ls moblllsed
much more slowly Lhen Lhe oLher componenLs of Lhe LCl.
1he remalnlng parLs of Lhe LCl are called Lhe funcLlonal LCl.
1he raLlo of lCl Lo LCl ls 33:43.
1he funcLlonal LCl ls more lmporLanL when conslderlng Lhe
effecLs of acuLe fluld lnLervenLlons and Lhe raLlo of lCl Lo
funcLlonal LCl ls 33:27.3 (whlch ls 2:1).
4. 8acter|a| vs. v|ra| |nfect|on
8acLerla are relaLlvely complex, slngle-celled creaLures wlLh a
rlgld wall and a Lhln, rubbery membrane surroundlng Lhe fluld
or cyLoplasm lnslde Lhe cell. Shaped llke balls, rods, or splrals,
Lhey conLaln all of Lhe geneLlc lnformaLlon needed Lo make
coples of Lhemselves. losslllzed records show LhaL bacLerla
have exlsLed for abouL 3.3 bllllon years, and lL's known LhaL
bacLerla can survlve ln a varleLy of envlronmenLs, lncludlng
exLreme heaL and cold, radloacLlve wasLe, and Lhe human
body.
MosL bacLerla are harmless, and some -- such as
Lhe *$+',-$+(..( $+(),/0(.12 bacLerla LhaL can llve ln Lhe
human lnLesLlne -- acLually help dlgesL food, desLroy dlsease-
causlng mlcrobes, flghL cancer cells, and provlde essenLlal
nuLrlenLs. lewer Lhan 1 of bacLerla cause dlsease ln people.
ln conLrasL, vlruses are Llny: Lhe largesL of Lhem are smaller
Lhan Lhe smallesL bacLerla. vlruses come ln varled shapes,
and have a llmlLed geneLlc blueprlnL. All Lhey have ls a proLeln
coaL and a core of geneLlc maLerlal: elLher 8nA or unA.
unllke bacLerla, vlruses can'L survlve wlLhouL a hosL. 1hey can
only reproduce by aLLachlng Lhemselves Lo cells and hl[acklng
Lhe cells' cellular machlnery. ln mosL cases, Lhey reprogram
Lhe cells Lo make new vlruses unLll Lhe cells bursL and dle. ln
oLher cases, Lhey Lurn normal cells lnLo mallgnanL or
cancerous cells.
Also unllke bacLerla, mosL vlruses ), cause dlsease, and
Lhey're qulLe speclflc abouL Lhe cells Lhey aLLack. lor example,
cerLaln vlruses are programmed Lo aLLacks cells ln Lhe llver,
resplraLory sysLem, or blood. ln some cases, vlruses called
bacLerlophages LargeL bacLerla.
8acLerlal and vlral lnfecLlons can boLh cause sympLoms such
as malalse, fever, and chllls. lL can be dlfflculL Lo dlsLlngulsh
whlch ls Lhe cause of a speclflc lnfecLlon.
lL's lmporLanL Lo
dlsLlngulsh, because vlral lnfecLlons cannoL be cured
by anLlbloLlcs.
S. k8C components
Ceneral CharacLerlsLlcs of 8lood:
CuAn1l1?
varles wlLh each lndlvldual buL Lhe mean average ln
Lhe adulL approxlmaLes 8 of Lhe body welghL or
around 1/13 of Lhe LoLal body welghL or 3 Lo 6 llLers
of blood or roughly esLlmaLed aL 73cc/kg body
welghL
CCLC8
ls due Lo Lhe presence of hemoglobln ln Lhe red
blood cells
! arLerlal blood appears as brlghL red due Lo
oxyhemoglobln, whlle venous blood ls
purpllsh red due Lo reduced hemoglobln.
! Coal gas polsonlng produces a brlghL cherry
red color due Lo carbon monoxlde-
hemoglobln, whlle poLasslum chloraLe
polsonlng glves a chocolaLe color due Lo
meLhemoglobln
8LAC1lCn
8lood ls sllghLly alkallne, havlng a pP of 7.4 Lo 7.43.
1hls alkallnlLy remalns consLanL LhroughouL llfe
SLClllC C8Avl1?
8anges from 1.073. lL sllghLly varles wlLh sex, belng
hlgher ln males Lhan females. ln paLhologlcal
condlLlon, Lhls ls greaLly alLered.
vlSCCSl1?
vlscoslLy of blood approxlmaLes 3 Lo 6 Llmes Lhan of
waLer
6. 8|ood component therapy- components and funct|ons
rlnclple 1: 1he cause of Lhe deflclency should be ldenLlfled.
rlnclple 2: 1he deflclenL componenL only should be replaced.
rlnclple 3: 1he blood producL should be as safe as posslble.
8|ood Const|tuents 1ype of 1ransfus|on keact|on
8ed cells AcuLe hemolyLlc
Lransfuslon reacLlon
uelayed Lransfuslon
reacLlon
1ransfuslon of red cell
alloanLlbodles (passlve
allolmmunlzaLlon)
AllolmmunlzaLlon
WhlLe cells lebrlle Lransfuslon
reacLlon
Leuoko- aggluLlnln-
assoclaLed pulmonary
edema
AllolmmunlzaLlon
laLeleLs AllolmmunlzaLlon
osL Lransfuslon porpura
Leukopenla
lasma proLelns urLlcarla
Anaphylaxls
Who|e 8|ood
ComposlLlon: 88Cs (approx. PcL 40), W8Cs, plaLeleLs,
plasma
volume: 300 mL
use: lncrease boLh red cell mass and plasma volume
(W8Cs and plaLeleLs noL funcLlonal, plasma deflclenL ln
lablle cloLLlng lacLors v and vlll)
Cllnlcal lndlcaLlons:
(1) AcLlve bleedlng wlLh aL leasL one of Lhe followlng:
Loss of over 13 blood volume
Pgb less Lhan 9 g/dL
8lood pressure decrease over 20 mm Pg
and/or less Lhan 90 mm Pg sysLollc
(2) re-operaLlve paLlenLs wlLh expecLed blood loss of
more Lhan 23 blood volume
SLorage 1emperaLure: 1-6C
Shelf Llfe: CuA-1 = 33 days
CuallLy ConLrol:
(1) Donor Hemoglobin 12.5 g/dL
(2) volume = 430 mL + 10
acked k8C
ComposlLlon: 88Cs (approx. PcL 73), reduced plasma,
W8Cs and plaLeleLs
volume: 230 mL
use: lncrease red cell mass ln sympLomaLlc anemla
(W8Cs and plaLeleLs noL funcLlonal)
Cllnlcal lndlcaLlons:
(1) Pgb less Lhan 8 gm/dL or PcL less Lhan 24 (lf noL
due Lo LreaLable cause)
(2) re-operaLlve paLlenLs wlLh:
Pgb less Lhan 8 g/dL or PcL less Lhan 24
Ma[or blood leLLlng operaLlon and Pgb <10
g/dL or PcL < 30
Slgns of lnadequaLe oxygen-carrylng
capaclLy (sympLomaLlc anemla)
(3) SympLomaLlc anemla lrregardless of Pgb level
(dyspnea, syncope, posLural hypoLenslon,
Lachycardla, chesL palns, 1lA)
(4) Pgb <10 g/dL or PcL <30 ln paLlenLs wlLh CCu,
CAu, hemogloblnopaLhy, sepsls, aorLlc sLenosls and
cerebral lnfarcL
(3) 8lood loss of less Lhan 10 blood volume
SLorage 1emperaLure: 1-6C
Shelf llfe: 1. CuA 1(close sysLem) = 33 days
2. CuA 1(open sysLem) = 24 hours
CuallLy ConLrol:
1. volume of red cells(4 per monLh)> 170 mL
2. PemaLocrlL(4/mo)< 70, never > 80
1 unlL red cell concenLraLe ralses Pgb by 1g/dL, and PcL
by 3
Washed k8C
ComposlLlon: 88Cs(approx. PcL 73), < 3 x 10
8
W8Cs, no
plasma
volume: 180 mL
use: lncrease red cell mass, reduce rlsk of allerglc
reacLlons Lo plasma proLelns
Cllnlcal lndlcaLlons:
(1) PlsLory of prevlous severe allerglc Lransfuslon
reacLlons or anaphylacLold reacLlon ln
lmmunocompromlsed paLlenLs
(2) Transfusion of group O blood during emergencies
when Lhe speclflc blood ls noL lmmedlaLely avallable
(3) aroxysmal nocLurnal hemogloblnurla
SLorage 1emperaLure: 1-6C
Shelf llfe: 24 hours
CuallLy ConLrol: Same as 88C (prlor Lo washlng)
Leuko-reduced k8C
ComposlLlon: > 83 orlglnal volume of 88C, < 3 x 10
6
W8Cs, few plaLeleLs, mlnlmal plasma
volume: 223 ml
uses: lncrease red cell mass, <3 x 10
6
W8Cs Lo decrease
Lhe llkellhood of febrlle reacLlon, lmmunlzaLlon Lo
leukocyLes (PLA anLlgens) or CMv Lransmlsslon
Cllnlcal lndlcaLlons : Same as 88Cs
SLorage 1emperaLure: 1-6C
Shelf llfe:
(1) CuA-1 (close sysLem) = 33 days
(2) CuA-1 (open sysLem) = 24 hours
CuallLy ConLrol:
(1) 8ed cell recovery (4 per monLh)
(2) LeukocyLe counL (4 per monLh)
|ate|et Concentrate (C) kandom Donor
ComposlLlon: laLeleL (>3.3 x 10
10
/unlL), 88Cs, W8Cs,
plasma
volume: 30 mL
use: SLop bleedlng due Lo LhrombocyLopenla or
LhrombocyLopaLhy
Cllnlcal lndlcaLlons:
(1) Prophylactic administration with count 20,000 and
noL due Lo 11, l1, PuS
(2) Active bleeding with count 50,000
(3) Platelet count 50,000 and patient to undergo
lnvaslve procedure wlLhln 8 hours
(4) Platelet count 100,000 if surgery in on critical area
(e.g. eye, braln, eLc.)
(3) Masslve Lransfuslon wlLh dlffuse mlcrovascular
bleedlng and no Llme Lo obLaln plaLeleL counL
SLorage 1emperaLure: 20 - 24C
Shelf llfe:
(1) CuA- 1 (close sysLem) = 3 days
(2) CuA-1 (open sysLem) = 24 hours
CuallLy ConLrol:
(1) pP (4 per monLh) = never < 6.0
(2) laLeleL counL (4 per monLh) = 3.3 x 10
10
(75%)
(3) lasma volume (4 per monLh) = 43 63 mL
Iresh Irozen |asma (II)
ComposlLlon: lasma wlLh all coagulaLlon facLors
volume: 200-230 ml
uses:
(1) rovlde all coagulaLlon facLors ln deflclency sLaLes
(2) lasma expander
Cllnlcal lndlcaLlons:
(1) 1 or 11 > 1.3 Llmes mld-normal range wlLhln 8
hours of Lransfuslon (1 > 17 sec., 11 > 47 sec)
(2) Speclflc facLor deflclencles noL LreaLable wlLh
cryopreclplLaLe
(3) 8eversal of coumadln anLlcoagulanL ln paLlenLs who
are bleedlng and noL LreaLable wlLh vlLamln k
(4) 1reaLmenL of 11
(3) aLlenL undergolng an lnvaslve procedure wlLh 1 of
less Lhan 70 and /or 11 of more Lhan 44 seconds
(6) Cllnlcal coagulopaLhy assoclaLed wlLh:
Massive transfusion ( 10 units of blood in 24
hours)
LaLe pregnancy LermlnaLlon or abrupLlo
placenLa
SLorage 1emperaLure: (-) 30C or lower
Shelf llfe: 12 monLhs
CuallLy ConLrol: volume (every unlL) =233 ml (mean)
Cryoprec|p|tate
ComposlLlon: lasma wlLh llbrlnogen, lacLors vlll and
xlll, von Wlllebrand lacLor
volume: 13-20 ml
uses:
(1) rovlde flbrlnogen, lacLors vlll and xlll and
Wlllebrand lacLor ln deflclency sLaLes, e.g.
Pemophllla A, Willebrands Disease
(2) 1oplcal llbrln glue
Cllnlcal lndlcaLlons:
(1) SlgnlflcanL hypoflbrlnogenemla (100 mg/dL)
(2) Pemophllla A
(3) Von Willebrands disease or uremic bleeding with
prolonged bleedlng Llme
SLorage 1emperaLure: (-) 30C or lower
Shelf llfe: 12 monLhs
CuallLy ConLrol: lacLor vlll (4/monLh) = 80 lu (mean)
kecommendat|ons:
k8C kCDUC1S:
1ransfuslon of blood producLs on a unlL-Lo-unlL basls
ls encouraged
A Lhorough cllnlcal re-evaluaLlon should be made
before Lhe nexL Lransfuslon
A represenLaLlve posL-Lransfuslon Pemoglobln and
PemaLocrlL deLermlnaLlon could be made aL leasL
afLer 24 hours
LA1LLL1 CCNCLN1kA1L
A represenLaLlve posL-Lransfuslon plaLeleL counL
could be made aL leasL afLer one(1) hour.
CkCkLCII1A1L AND IkLSn IkC2LN LASMA
A more accuraLe posL-Lransfuslon 1 and/or 11
could be done aL leasL afLer 4 hours.
7. Anem|as
Anemla ls mosL ofLen recognlzed by abnormal screenlng
laboraLory LesLs
- AcuLe anemla due Lo blood loss or hemolysls
(nearly always)
Anemla due Lo blood loss
Mlld blood loss
Lnhanced C2 dellvery achleved Lhru changes n C2-
hemoglobln dlssoclaLlon curve medlaLed by decreased pP or
lncreased CC2 (8ohr effecL)
AcuLe blood loss 10-13
- slgns of vascular lnsLablllLy
- lssue ls hypoLenslon & decreased organ perfuslon
>30 blood loss
- unable Lo compensaLe w/ usual mechanlsms of vascular
conLracLlon & changes n reglonal blood flow
- prefers Lo remaln suplne, posLural hypoLenslon &
Lachycardla lf uprlghL
> 40 blood loss
- slgns of hypovolemlc shock: confuslon, dyspnea,
dlaphoresls, hypoLenslon, and Lachycardla
- requlre lmmedlaLe volume replacemenL
Anemla due Lo hemolysls
- slgns and sympLoms depend on Lhe mechanlsm LhaL
lead Lo red cell desLrucLlon
- lnLravascular hemolysls acuLe back pan, free hgb ln
urlne, and renal fallure
- Chronlc or progresslve anemla sympLoms depend on
age and adequacy of blood supply Lo crlLlcal organs
- ModeraLe anemla faLlgue, loss of sLamlna,
breaLhlessness, and Lachycardla (parLlc w/ physlcal
exerLlon)
CerLaln dlsorders commonly assoc w/ anemla:
- Chronlc lnflammaLory sLaLes (eg. lnfecLlon, rheumaLold
arLhrlLls) assoc w/ mlld-moderaLe anemla
- LymphoprollferaLlve dlsorders (eg chronlc lymphocyLlc
leukemla & cerLaln oLher 8 cell neoplasms) may be
assoc w/ auLolmmune hemolysls
8. er|phera| b|ood smear
Approach to at|ent
n|story
nuLrlLlonal hx relaLed Lo drugs or alcohol lnLake
famlly hx of anemla
cerLaln geographlc backgrounds & eLhnlc orlglns assoc w/
lnherlLed dlsorder of hgb molecule or lnLermedlary
meLab (eg. C6u deflclency & cerLaln
hemogloblnopaLhles more common n Mlddle LasLern or
Afrlcan orlgln
exposure Lo cerLaln Loxlc agenLs or drugs
slgns & sympLoms relaLed Lo oLher dlsorders commonly
assoc w/ anemla: bleedlng, faLlgue, malalse, fever,
welghL loss, nlghL sweaLs, and oLher sysLemlc sympLoms.
hys|ca| Lxam
forceful hearLbeaL, sLrong perlpheral pulses, sysLollc
flow murmur
skln & mucous membranes pale hgb < 8-10 g/dL
areas where vessels are close Lo surface mucous
membranes, nall beds, palmar creases
clues Lo mechanlsms of anemla: lnfecLlon, blood ln sLool,
lymphadenopaLhy, splenomegaly, peLechlae
splenomegaly & lymphadenopaLhy suggesL
lymphoprollferaLlve dlsease
peLechlae suggesL plaLeleL dysfuncLlon
Laboratory Lva|uat|on
CompleLe blood counL (C8C)
requlred as parL of Lhe evaluaLlon
lncludes hgb, hcL, & red cell lndlces: MCv, MCP & MCPC
affecLlng facLors: age, gender, pregnancy, smoklng, &
alLlLude
also lncluded: descrlpLlon of boLh 88C & W8C, W8C
dlfferenLlal counL & plaLeleL counL
classlflcaLlon of anemla
MlcrocyLosls MCv < 80, MacrocyLosls MCv >100
Pypochromla low MCP & MCPC
er|phera| 8|ood Smear
provldes lmporLanL lnfo abouL defecLs ln 88C producLlon
anlsocyLosls
varlaLlon ln cell slze
usually correlaLes w/ 8uW (red cell dlsLrlbuLlon wldLh) or
range of cell slzes
polkllocyLosls
varlaLlon ln cell shape
suggesLs defecL ln maLuraLlon of red cell precursors ln
8M or fragmenLaLlon of clrculaLlng 88Cs
polychromasla
red cells sllghLly larger Lhan normal & graylsh blue ln
color on WrlghL-Clemsa sLaln
reLlculocyLes premaLurely released from 8M, Lhelr color
represenLs resldual amounLs of r8nA
nucleaLed red cells, Powell-!olly bodles, LargeL cells,
slckle cells, and oLhers may provlde clues Lo speclflc
dlsorders
9. Reyes syndrome
keye's syndrome ls a poLenLlally faLal dlsease LhaL causes
numerous deLrlmenLal effecLs Lo many organs, especlally
Lhe braln and llver, as well as causlng a lower Lhan usual level
of blood sugar (hypoglycemla). 1he classlc feaLures are a rash,
vomlLlng, and llver damage. 1he exacL cause ls unknown, and
whlle lL has been assoclaLed wlLh asplrln consumpLlon by
chlldren wlLh vlral lllness, lL also occurs ln Lhe absence of
asplrln use.
1he dlsease causes faLLy llver wlLh mlnlmal lnflammaLlon and
severe encephalopaLhy (wlLh swelllng of Lhe braln). 1he llver
may become sllghLly enlarged and flrm, and Lhere ls a change
ln Lhe appearance of Lhe kldneys. !aundlce ls noL usually
presenL.
SLage l
8ash on palms of hands and feeL
erslsLenL, heavy vomlLlng LhaL ls noL relleved by noL
eaLlng
Cenerallzed leLhargy
Confuslon
nlghLmares
Plgh fever
Peadaches
SLage ll
SLupor caused by encephallLls
PypervenLllaLlon
laLLy llver (found by blopsy)
PyperacLlve reflexes
SLage lll
ConLlnuaLlon of SLage l and ll sympLoms
osslble coma
osslble cerebral oedema
8arely, resplraLory arresL
SLage lv
ueepenlng coma
ullaLed puplls wlLh mlnlmal response Lo llghL
Mlnlmal buL sLlll presenL hepaLlc dysfuncLlon
SLage v
very rapld onseL followlng sLage lv
ueep coma
Selzures
MulLlple organ fallure
llaccldlLy
Pyperammonemla (> 300 mg/dL of blood)
ueaLh
Card|ovascu|ar
1. neart b|ood supp|y
1he hearL ls a hollow, cone-shaped muscle locaLed beLween
Lhe lungs and behlnd Lhe sLernum (breasLbone). 1wo-Lhlrds of
Lhe hearL ls locaLed Lo Lhe lefL of Lhe mldllne of Lhe body and
1/3 ls Lo Lhe rlghL.
1he apex (polnLed end) polnLs down and Lo Lhe lefL. lL ls 3
lnches (12 cm) long, 3.3 lnches (8-9 cm) wlde and 2.3 lnches
(6 cm) from fronL Lo back, and ls roughly Lhe slze of your flsL.
1he average welghL of a female human hearL ls 9 ounces and
a male's ls 10.3 ounces. 1he hearL comprlses less Lhan 0.3 of
Lhe LoLal body welghL.
1he hearL has 3 layers. 1he smooLh lnslde llnlng of Lhe hearL ls
called Lhe endocardlum. 1he mlddle layer of hearL muscle ls
called Lhe myocardlum. lL ls surrounded by a fluld fllled sac
call Lhe perlcardlum.
1he hearL ls dlvlded lnLo 4 chambers:
(1) 8lghL ALrlum (8A)
(2) venLrlcle (8v)
(3) ALrlum (LA)
(4) LefL venLrlcle (Lv)
Lach chamber has a sorL of one-way valve aL lLs exlL LhaL
prevenLs blood from flowlng backwards. When each chamber
conLracLs Lhe valve aL lLs exlL opens. When lL ls flnlshed
conLracLlng Lhe valve closes so LhaL blood does noL flow
backwards.
(3) 1r|cusp|d va|ve - ls aL Lhe exlL of Lhe 8lghL ALrlum
(6) u|monary va|ve - ls aL Lhe exlL of Lhe 8lghL venLrlcle
(7) M|tra| va|ve - ls aL Lhe exlL of Lhe LefL aLrlum
(8) Aort|c va|ve - ls aL Lhe exlL of Lhe LefL venLrlcle.
When Lhe hearL muscle conLracLs or beaLs (called sysLole) lL
pumps blood ouL of Lhe hearL. 1he hearL conLracLs ln Lwo
sLages. ln Lhe flrsL sLage Lhe 8lghL and LefL ALrla conLracL aL
Lhe same Llme, pumplng blood Lo Lhe 8lghL and LefL
venLrlcles. 1hen Lhe venLrlcles conLracL LogeLher Lo propel
blood ouL of Lhe hearL. 1hen Lhe hearL muscle relaxes (called
dlasLole) before Lhe nexL hearLbeaL. 1hls allows blood Lo flll
up Lhe hearL agaln.
1he rlghL and lefL sldes of Lhe hearL have separaLe funcLlons.
1he rlghL slde of Lhe hearL collecLs oxygen-poor blood from
Lhe body and pumps lL Lo Lhe lungs where lL plcks up oxygen
and releases carbon dloxlde. 1he lefL slde of Lhe hearL Lhen
collecLs oxygen rlch blood from Lhe lungs and pumps lL Lo Lhe
body so LhaL Lhe cells LhroughouL your body have Lhe oxygen
Lhey need Lo funcLlon properly.
1he hearL, [usL llke any oLher organ, requlres blood Lo supply
lL wlLh oxygen and oLher nuLrlenLs so LhaL lL can do lLs work.
1he hearL does noL exLracL oxygen and oLher nuLrlenLs from
Lhe blood flowlng lnslde lL -- lL geLs lLs blood from coronary
arLerles LhaL evenLually carry blood wlLhln Lhe hearL muscle.
ApproxlmaLely 4-3 of Lhe blood ouLpuL of Lhe hearL goes Lo
Lhe coronary arLerles (7 x ounces/mlnuLe or 223 ml/mln).
1here are Lwo maln coronary arLerles - 1he LefL Maln
Coronary arLery (1) and Lhe 8lghL Coronary ArLery (2) whlch
arlse from Lhe AorLa. 1he LefL Maln Coronary ArLery dlvldes
lnLo Lhe LefL AnLerlor uescendlng 8ranch (3) and Lhe LefL
Clrcumflex ArLerles (4). Lach arLery supplles blood Lo dlfferenL
parLs of Lhe hearL muscle and Lhe elecLrlcal sysLem.
1he hearL also has velns LhaL collecL oxygen-poor blood from
Lhe hearL muscle. MosL of Lhe ma[or velns of Lhe hearL (greaL
cardlac veln, small cardlac veln, mlddle cardlac veln, posLerlor
veln of Lhe LefL venLrlcle, and obllque veln of Lhe LefL ALrlum)
draln lnLo Lhe coronary slnus whlch opens lnLo Lhe 8lghL
ALrlum.
Coronary arLery dlsease ls caused by a blockage ln one of Lhe
coronary arLerles. When a coronary arLery ls parLlally blocked,
LhaL arLery cannoL supply enough blood Lo Lhe hearL muscle
Lo meeL lLs needs durlng exerLlon. When someone wlLh
coronary arLery dlsease exerLs hlmself or herself, lL causes
chesL paln. 1hls ls due Lo lack of blood and oxygen Lo LhaL
parL of Lhe hearL muscle and ls called anglna. lf Lhe
obsLrucLlon worsens (more frequenL anglna eplsodes, wlLh
less exerLlon) a condlLlon called unsLable anglna can occur. A
hearL aLLack happens when a coronary arLery ls compleLely
blocked and no blood or oxygen ls geLLlng Lo Lhe hearL muscle
served by LhaL arLery. 1hls also causes chesL paln and causes
deaLh Lo Lhe hearL muscle served by LhaL arLery.
2. 8|ood c|rcu|at|on upper and |ower
3. Card|ac cyc|e
use Lhe LCC as an evenL marker.
Cpenlng and closlng of valves causes Lhe physlologlc
hearL sounds.
When all valves are closed, venLrlcular volume ls
consLanL, and Lhe phase ls called lsovolumeLrlc.
A. Atr|a| systo|e
preceded by Lhe wave, whlch represenLs elecLrlcal
acLlvaLlon of Lhe aLrla.
conLrlbuLes Lo, buL ls noL essenLlal for, venLrlcular
fllllng
lncrease ln aLrlal pressure (venous pressure) caused
by aLrlal sysLole ls Lhe a wave on Lhe venous pulse
curve
lllllng of Lhe venLrlcle by aLrlal sysLole causes Lhe
fourLh hearL sound, whlch ls noL audlble ln normal
adulLs.
8. Isovo|umetr|c ventr|cu|ar contract|on
beglns afLer Lhe onseL of Lhe C8S wave, whlch
represenLs elecLrlcal acLlvaLlon of Lhe venLrlcles.
When venLrlcular pressure becomes greaLer Lhan
aLrlal pressure, Lhe Av valves close. 1helr closure
corresponds Lo Lhe flrsL hearL sound. 8ecause Lhe
mlLral valve closes before Lhe Lrlcuspld valve, Lhe
flrsL hearL sound may be spllL.
C. Isovo|umetr|c ventr|cu|ar re|axat|on
8epolarlzaLlon of Lhe venLrlcles ls now compleLe
(end of Lhe 1 wave).
1he aorLlc valve closes, followed by closure of Lhe
pulmonlc valve. Closure of Lhe semllunar valves
corresponds Lo Lhe second hearL sound. lnsplraLlon
causes spllLLlng of Lhe second hearL sound.
1he Av valves remaln closed durlng mosL of Lhls
phase.
venLrlcular pressure decreases rapldly because Lhe
venLrlcle ls now relaxed.
venLrlcular volume ls consLanL (lsovolumeLrlc)
because all of Lhe valves are closed.
The blip in the aorLlc pressure Lraclng occurs afLer
closure of Lhe aorLlc valve and lscalled Lhe dlcroLlc
noLch, or lnclsura.
When venLrlcular pressure becomes less Lhan aLrlal
pressure, Lhe mlLral valve opens.
u. kap|d ventr|cu|ar f||||ng
mlLral valve ls open and venLrlcular fllllng from Lhe
aLrlum beglns.
AorLlc pressure conLlnues Lo decrease because blood
conLlnues Lo run off lnLo Lhe smallerarLerles.
8apld flow of blood from Lhe aLrla lnLo Lhe venLrlcles
causes Lhe Lhlrd hearL sound, whlch lsnormal ln
chlldren buL, ln adulLs, ls assoclaLed wlLh dlsease.
L. keduced ventr|cu|ar f||||ng (d|astas|s)
longesL phase of Lhe cardlac cycle.
venLrlcular fllllng conLlnues, buL aL a slower raLe.
1he Llme requlred for dlasLasls and venLrlcular fllllng
depends on hearL raLe. lncreases ln hearL raLe
decrease Lhe Llme avallable for venLrlcular refllllng.
4. LCG trac|ng
A. LCG kecord|ng
a. aper speed: 23mm/sec
b. PorlzonLal axls/1lme lnLerval
l. Small square:1mm=0.04sec
ll. 8lg square: 3mm=0.20sec
c. verLlcal axls/AmpllLude(volLage) : 10mm =1mv (2blgsqs)
av8 - 130
o
avL -30
o
l 0
o
lll+120
o
ll+60
o
avl +90
o
8. Ma[or Waves]Interva|s
wave: atr|a| depo|ar|zat|on (best seen |n II,III,aVI)
uuraLlon: <0.11sec (0.03-0.10)
AmpllLude: <3mm (0.3-2.3)
Shape: dome-shaped/genLly rounded
u8lCP1: l, ll, avl, v4, v3, v6
lnvL81Lu: av8
8lPASlC: lll, avL, v1, v2, v3
Lermlnal lorce/Morrls lndex = duraLlon x ampllLude
(n.v. < 0.04mmsec, lnc ln LAL)
Marcus lndex = wave duraLlon / 8 segmenL
(n.v 1-1.6, lnc ln LAL)
kS Comp|ex: ventr|cu|ar depo|ar|zat|on
uuraLlon: <0.10sec (0.3-0.10)
AmpllLude: <23mm (>3mm ln llmb leads, >10mm ln chesL
leads)
volLage: 8l + Slll < 23mm (volLage crlLerla) or
Max 8 + ueepesL S (precordlal lead) <43mm
u8lCP1: l, avL, v3, v6, ll, lll, avl
lnvL81Lu: av8, v1, v2
8lPASlC: v3, v4
1 wave: ventr|cu|ar repo|ar|zat|on
AmpllLude: <3mm ln llmb leads, <10mm ln chesL leads
Shape: sllghLly rounded, asymmeLrlcal
u8lCP1: same dlrecLlon wlLh C8S
lnvL81Lu: normal ln v1, v2, and v3 for pLs <30 yrs old
lnverLed only ln v1 for pLs >30 yrs old
U wave: urk|n[e f|ber repo|ar|zat|on
AmpllLude: noL >1mm
romlnenL ln v3
u8lCP1: hypokalemla, qulnldlne
lnvL81Lu: lschemla, LvP
k wave rogress|on: k wave |ncreases from k to L chest (V1-V6)
k wave = S wave |n trans|t|on zone V3]V4
normal: LranslLlon from predomlnanLly negaLlve Lo
predomlnanLly poslLlve aL v3 or v4
oor k Wave rogress|on: |f k wave <3mm by V3
Causes: AnLero-SepLal Ml w/ S1 uep, LvP (1.3- 3.0mm 8
wave ln v3)
Lar|y 1rans|t|on: kS becomes predom|nant|y (+) ear||er
(V1]V2)
Causes: osLerlor Ml, 8vP, normal ln lnfanLs
S1 Segment: end of kS (I-po|nt) and beg|nn|ng of 1 wave
lsoelecLrlc, beLween -0.3 & +1 from basellne
AlLered by: lschemla, ln[ury, sLraln, drugs, meLabollc, sLroke
k Interva|: atr|a| depo|ar|zat|on
Where Lo measure: sLd or unlpolar llmb leads wlLh longesL 8
lnLerval
normal 8ange: 0.12 0.20 sec
ShorLened: lnc P8, lnfanLs, accessory conducLlon
paLhway,sLerolds
rolonged: drug effecL (dlglLalls, 88, CC8) hyperLrophy, aLrlal
dllaLaLlon, aglng, SSS, Ml
kS Interva|
Where Lo measure: any lead
normal 8ange: <0.10sec
ShorL: normal
Wlder: v1-v6, delayed conducLlon, vCs, accessory bypass
LracL
1 Interva|: beg|nn|ng of kS end of 1 wave
normal 8ange: 0.33- 0.43sec
lnversely relaLed Lo P8
rolonged: 1u, elecLrolyLe abn, anLl-dysrhyLhmlc drugs
C. kates: rate]m|n
Ca|cu|at|on by: 1S00 Method most prec|se, for regu|ar
rhythm on|y
now to: 1300/ # of small squares beLween 2 consecuLlve C8S
Ca|cu|at|on by: k-k Method for regu|ar rhythm on|y
now to: llnd C8S where 8 wave falls on heavy dark llne, use
Lhls as a reference. CounL heavy dark llnes beLween C8S as 300,
130,100,73,60,30
Ca|cu|at|on by: 6-second Method eas|est but |east accurate,
|rreg rhythm
now to: CounL Lhe number of C8S occurrlng ln 6 seconds and
mulLlply by 10
Note: shorL verLlcal llnes or doLs on Lop of LCC paper represenL
1-, 2-, 3- sec lnLervals
Cther methods:
Ior |rregu|ar rhythm: # of or C8S x 20 ln 3sec sLrlp
Ior regu|ar rhythm: 300/# of blg squares b/w 2 consecuLlve /8
1300/ # of small squares b/w 2 consecuLlve
/8
D. khythms
Cr|ter|a for NSk
1. normal wave ( same conLour ln same lead)
2. followed by normal C8S
3. normal 8 lnLerval
4. 8aLe: 60-100bpm
3. Cycle lengLh noL varylng by >10
L. Ax|s
Latera| L|mb Leads: l, avL
Infer|or L|mb Leads: ll, lll, avl
Norma| kS Ax|s: 0
o
Lo 90
o
may vary from -30
o
Lo +110
o
Ax|s Dev|at|on by Lyeba|| Method |ook at Leads I and aVI
Lead I (+) & aVI (+) : normal
Lead I (+) & aVI (-) : LefL Axls uevlaLlon
Lead I (-) & aVI (+) : 8lghL Axls uevlaLlon
Lead I (-) & aVI (-) : Extreme RAD/ Indetermine Axis/No Mans Land
Note: (-) |nverted, (+) upr|ght
Causes of LAD: LvL/LvP, Aglng, Ml, LAl8, Lndocardlal paclng
Causes of kAD: 8v, Pn, S, AcuLe L, CPu, Ml, Ll8,
Lplcardlal aclng
I. Chamber Ln|argement
k|ght Atr|a| Ln|argement LCG C|ues
1. 1all,peaked wave (>2.3mm) ln ll,lll, avl -
pulmonale
2. 1all lnlLlal upsLroke of ln v1 >0.06sec
3. normal wave wldLh/duraLlon
4. lronLal wave axls >+73
o
3. 8educed LoLal C8S ampllLude ln v1 <0.6mv w/ 3x
more lnc ln v2
Left Atr|a| Ln|argement LCG C|ues
1. noLched or m shaped wave ln l,ll,avL mlLrale,
blphaslc ln v1
2. Small lnlLlal upsLroke of wave ln v1
3. Wlder wave duraLlon ( >0.11sec) ln Lead ll
4. lncreased Morrls and Marcus lndex
3. LefLward shlfL of mean wave axls Lo +43
o
& -30
o
k|ght Ventr|cu|ar nypertrophy: reverses norma| k wave
progress|on |n V1-V6
Soko|ow-Lyon Cr|ter|a
1. 8v1 + Sv3-6 >11mm
2. 8 ln v1 >7mm
3. 8:S raLlo ln v1 >1
4. 8Au >+90
o
8ut|er-Legget
1. (8 ln v1-2 + S ln v6) S ln l/v1 > 7mm
L|pman
1. 8Au
2. PelghL/volLage of C8S ls lncreased
a. PelghL of 8 wave > depLh of S ln v1
b. 8 wave >7mm ln v1, >3mm ln av8
c. S wave ln v1 <2mm
3. negaLlve deflecLlon ls lncreased
a. ueeper S wave ln v3 & v6
4. CnseL of lnLrlnslcold deflecLlon delayed beyond 0.02
sec ln rlghL chesL lead, normal ln lefL
3. Incomplete RBBB ( rSR in V1)
6. SllghLly prolonged C8S >0.10sec
7. S1 segmenL depresslon & 1 wave lnverslon ln v1 & v2
noLe: lnLrlnslcold deflecLlon reflecLs Llme requlred Lo
depolarlze Lhe venLrlcle from endo Lo eplcardlum,
measured from beglnnlng of C8S Lo peak of 8 wave
Left Ventr|cu|ar nypertrophy: exaggerates k wave progress|on |n
V1-V6, k waves ta||er, S waves deeper
Soko|ow-Lyon Cr|ter|a
1. Sv1 + 8v3-6 >33mm
2. 8 ln avL > 12mm, avl >20mm
3. 8 ln l + S ln lll >23mm
4. S ln v1 >24mm
Corne|| Vo|tage Cr|ter|a
1. M: S ln v3 + 8 ln avL >28mm
2. l: S ln v3 + 8 ln avL >20mm
L|pman
1. LAu
2. PelghL/volLage of C8S lncreased ln l,avL,v3,v6, depLh
lncreased ln v1 & v2
a. 8 wave >26mm ln v3 or v6, >11mm ln avL
b. PelghL of 8 wave ln v3 or v6 + S wave depLh ln
v1 >33mm
c. S wave deeper ln v1 and v2
3. CnseL of lnLrlnslcold deflecLlon delayed beyond
0.04sec ln lefL chesL leads, normal ln rlghL
4. rolonged C8S >0.09 Lo 0.12sec
3. S1 segmenL depresslon & 1 wave lnverslon ln
l,avL,v3,v6
Lstes Cr|ter|a ( at |east S po|nts)
1. 3 polnLs volLage, S1 segmenL, 1 wave changes, LAP
LxcepLlon: 1 polnL lf paLlenL Lakes dlglLalls
2. 2 polnLs LAu
3. 1 polnL wlde C8S, delayed lnLrlnslcold deflecLlon
S. Murmurs- types and grad|ng
Murmurs can be classlfled by seven dlfferenL characLerlsLlcs:
Llmlng, shape, locaLlon, radlaLlon, lnLenslLy, plLch and quallLy.
1|m|ng refers Lo wheLher Lhe murmur ls
a sysLollc or dlasLollc murmur.
Shape refers Lo Lhe lnLenslLy over Llme, murmurs can
be crescendo, decrescendo or crescendo-decrescendo.
Locat|on refers Lo where Lhe hearL murmur ls
usually ausculLaLed besL. 1here are slx places on Lhe
anLerlor chesL Lo llsLen for hearL murmurs, each of Lhe
locaLlons roughly corresponds Lo a speclflc parL of Lhe
hearL. 1he flrsL flve of Lhe slx locaLlons are ad[acenL Lo
LhesLernum. 1he slx locaLlons are:
Lhe 2nd rlghL lnLercosLal space
Lhe 2nd Lo 3Lh lefL lnLercosLal spaces
Lhe 3Lh lefL mld-clavlcular lnLercosLal space.
kad|at|on refers Lo where Lhe sound of Lhe murmur
radlaLes. 1he general rule of Lhumb ls LhaL Lhe sound
radlaLes ln Lhe dlrecLlon of Lhe blood flow.
Intens|ty refers Lo Lhe loudness of Lhe murmur, and ls
graded on a scale from 0-6/6.
|tch can be low, medlum or hlgh and ls deLermlned by
wheLher lL can be ausculLaLed besL wlLh Lhe bell or
dlaphragm of a sLeLhoscope.
ua||ty refers Lo unusual characLerlsLlcs of a murmur,
such as b|ow|ng, harsh, rumb||ng or mus|ca|.
1he use of Lwo slmple mnemonlcs may help dlfferenLlaLe
sysLollc and dlasLollc murmurs, ASS and Alu. 3ulmonary
and $orLlc 2Lenoses are 2ysLollc whlle /ulmonary
and $orLlc (nsufflclencles (regurglLaLlon) are )lasLollc. MlLral
and Lrlcuspld defecLs are opposlLe.
Grad|ng Descr|pt|on
Grade 1 very falnL
Grade 2 SofL
Grade 3 Peard all over Lhe precordlum
Grade 4 Loud, wlLh palpable Lhrlll
Grade S very loud, wlLh Lhrlll. May be heard wlLh
sLeLhoscope parLly off chesL
Grade 6 very loud, wlLh Lhrlll. May be heard wlLh
sLeLhoscope enLlrely off chesL
6. Ieta| c|rcu|at|on
1hroughouL Lhe feLal sLage of developmenL, Lhe maLernal
blood supplles Lhe feLus wlLh C
2
and nuLrlenLs and carrles
away lLs wasLes.
1hese subsLances dlffuse beLween Lhe maLernal and feLal
blood Lhrough Lhe placenLal membrane.
1hey are carrled Lo and from Lhe feLal body by Lhe umblllcal
blood vessels.
1he concenLraLlon of hemoglobln ln feLal blood ls abouL 30
greaLer Lhan ln maLernal blood.
leLal hemoglobln ls sllghLly dlfferenL chemlcally and has a
greaLer afflnlLy for C
2
Lhan maLernal hemoglobln.
AL a parLlcular oxygen parLlal pressure, feLal hemoglobln can
carry 20-30 more C
2
Lhan maLernal hemoglobln.
ln Lhe feLal clrculaLory sysLem, Lhe umblllcal veln LransporLs
blood rlch ln C
2
and nuLrlenLs from Lhe placenLa Lo Lhe feLal
body.
1he umblllcal veln enLers Lhe body Lhrough Lhe umblllcal
rlng and Lravels along Lhe anLerlor abdomlnal wall Lo
Lhe llver.
! AbouL 1/2 Lhe blood lL carrles passes lnLo Lhe llver.
! 1he oLher 1/2 of Lhe blood enLers a vessel called
Lhe ducLus venosus whlch bypasses Lhe llver.
1he ducLus venosus Lravels a shorL dlsLance and [olns
Lhe lnferlor vena cava.
! 1here, Lhe oxygenaLed blood from Lhe placenLa ls
mlxed wlLh Lhe deoxygenaLed blood from Lhe lower
parLs of Lhe body.
! 1hls mlxLure conLlnues Lhrough Lhe vena cava Lo
Lhe rlghL aLrlum.
ln Lhe adulL hearL, blood flows from Lhe rlghL aLrlum Lo
Lhe rlghL venLrlcle Lhen Lhrough Lhe pulmonary arLerles
Lo Lhe lungs.
! ln Lhe feLus however, Lhe lungs are nonfuncLlonal
and Lhe blood largely bypasses Lhem.
As Lhe blood from Lhe lnferlor vena cava enLers Lhe rlghL
aLrlum, a large proporLlon of lL ls shunLed dlrecLly lnLo
Lhe lefL aLrlum Lhrough an openlng called Lhe foramen
ovale.
! A small valve, sepLum prlmum ls locaLed on Lhe lefL
slde of Lhe aLrlal sepLum overlles Lhe foramen
ovale and helps prevenL blood from movlng ln Lhe
reverse dlrecLlon.
1he resL of Lhe feLal blood enLerlng Lhe rlghL aLrlum,
lncludlng a large proporLlon of Lhe deoxygenaLed blood
enLerlng from Lhe superlor vena cavapasses lnLo Lhe rlghL
venLrlcle and ouL Lhrough Lhe pulmonary Lrunk.
! Cnly a small volume of blood enLers Lhe pulmonary
clrculL, because Lhe lungs are collapsed, and Lhelr
blood vessels have a hlgh reslsLance Lo flow.
Lnough blood reaches Lhe lung Llssue Lo
susLaln Lhem.
MosL of Lhe blood ln Lhe pulmonary Lrunk bypasses Lhe
lungs by enLerlng a feLal vessel called Lhe ducLus
arLerlosus whlch connecLs Lhe pulmonary Lrunk Lo
Lhe descendlng porLlon of Lhe aorLlc arch.
! As a resulL of Lhls connecLlon, Lhe blood wlLh a
relaLlvely low C
2
concenLraLlon whlch ls reLurnlng Lo
Lhe hearL Lhrough Lhe superlor vena cava, bypasses
Lhe lungs.
! AL Lhe same Llme, Lhe blood ls prevenLed from
enLerlng Lhe porLlon of Lhe aorLa LhaL provldes
branches leadlng Lo Lhe braln.
1he more hlghly oxygenaLed blood LhaL enLers Lhe lefL
aLrlum Lhrough Lhe foramen ovale ls mlxed wlLh a small
amounL of deoxygenaLed blood reLurnlng from
Lhe pulmonary velns.
! 1hls mlxLure moves lnLo Lhe lefL venLrlcle and ls
pumped lnLo Lhe aorLa.
Some of lL reaches Lhe myocardlum Lhrough
Lhe coronary arLerles and some reaches Lhe
braln Lhrough Lhe caroLld arLerles.
1he blood carrled by Lhe descendlng aorLa ls parLlally
oxygenaLed and parLlally deoxygenaLed.
! Some of lL ls carrles lnLo Lhe branches of Lhe aorLa
LhaL lead Lo varlous parLs of Lhe lower reglons of Lhe
body.
! 1he resL passes lnLo Lhe umblllcal arLerles, whlch
branch from Lhe lnLernal lllac arLerles and lead Lo
Lhe placenLa.
1here Lhe blood ls reoxygenaLed.
7. Shock types and parameters
Card|ogen|c Shock
blood flow decreased due Lo an lnLrlnslc defecL ln cardlac
funcLlon elLher Lhe hearL muscle, or Lhe valves are
dysfuncLlonal
classlcal example ls acuLe anLerlor myocardlal lnfarcLlon,
when Lhe amounL of damaged lschaemlc muscle may be so
greaL LhaL Lhe hearL cannoL pump anymore. 1he decreased
conLracLlllLy causes a decrease ln sLroke volume
Lyplcal haemodynamlc plcLure:
! decreased cardlac ouLpuL and blood pressure
! hlgh lefL venLrlcular fllllng pressures (backward
fallure)
! lncreased sysLemlc vascular reslsLance (from
vasoconsLrlcLlon, whlch ls a sympaLheLlc compensaLory
response Lo Lhe low blood pressure)
! lncreased hearL raLe (sympaLheLlc compensaLory
response Lo Lhe low blood pressure)
! oLher feaLures of cardlogenlc shock such as Lhe cool
perlpherles, decreased urlne ouLpuL and sweaLlng can
also be explalned by Lhe sympaLheLlc compensaLory
response.
nypovo|em|c shock
resulL of lnLravascular blood volume depleLlon
common causes:
! haemorrhage
! vomlLlng
! dlarrhoea
! dehydraLlon
! Lhlrd-space losses durlng ma[or operaLlons
prlmary abnormallLy ls a decrease ln preload. 1he
decreased preload causes a decrease ln sLroke volume.
Lyplcal haemodynamlc plcLure:
! decreased cardlac ouLpuL and blood pressure
! low lefL venLrlcular fllllng pressures (because Lhe
venLrlcle ls empLy)
! lncreased Sv8 (from vasoconsLrlcLlon, whlch ls a
sympaLheLlc compensaLory response Lo Lhe low blood
pressure)
! lncreased hearL raLe (sympaLheLlc compensaLory
response Lo Lhe low blood pressure)
CLher feaLures of hypovolaemlc shock are slmllar Lo
Lhose seen ln cardlogenlc shock and lnclude cool perlpherles,
decreased urlne ouLpuL and sweaLlng LhaL can also be
explalned by Lhe sympaLheLlc compensaLory response.
D|str|but|ve Shock
occurs when Lhe perlpheral vascular dllaLaLlon causes a
fall ln Sv8
mosL common causes:
! sepLlc shock
! anaphylacLlc shock
! acuLe adrenal lnsufflclency
! neurogenlc shock.
cardlac ouLpuL ls ofLen lncreased buL Lhe perfuslon of
many vlLal organs ls compromlsed because Lhe blood
pressure is too low and the body loses its ability to distribute
blood properly
hemodynamlc proflle ls usually characLerlsed by:
! normal or lncreased cardlac ouLpuL wlLh a low Sv8
! low Lo normal lefL venLrlcular fllllng pressures
! low blood pressure
cllnlcal feaLures lnclude:
! warm perlpherles
! boundlng pulses
! Llssue dysfuncLlon desplLe Lhls:
menLal sLaLus changes
ollgurla
lacLlc acldosls.
Cbstruct|ve Shock
Cardlac Lamponade
exLracardlac obsLrucLlve shock
mechanlcal obsLrucLlon Lo cardlac fllllng
pressures of Lhe rlghL cardlac chambers, Lhe pulmonary
arLery, and Lhe lefL cardlac chambers equlllbraLe ln dlasLole
always conslder cardlac Lamponade when Lhe Cv ls hlgh
and 8 low.
pulsus paradoxus
! exaggeraLlon of normal physlology ln whlch Lhere ls
a decrease of >10 mm Pg ln sysLollc blood pressure
durlng lnsplraLlon
! lmporLanL cllnlcal flndlng ln paLlenLs wlLh suspecLed
cardlac Lamponade
r|nc|p|es of management
look for reverslble causes such as acuLe valvular
lnsufflclency, drug overdose, or Lamponade
ma[or goal of managemenL ls Lo reLurn Llssue oxygen
dellvery Lo normal. 1he LreaLmenL prlorlLy ls Lherefore Lo
lncrease cardlac ouLpuL and blood pressure. CpLlmlslng Lhe
oxygen conLenL of blood can also help Lo lmprove Llssue
oxygen dellvery. 1he goal of lmprovlng cardlac ouLpuL and
blood pressure ls usually accompllshed wlLh some
comblnaLlon of ad[usLlng preload, lncreaslng cardlac
conLracLlllLy and opLlmlslng Sv8. Lnsurlng boLh good
oxygenaLlon and haemoglobln conLenL opLlmlses Lhe oxygen
conLenL of Lhe blood
occaslonally, hearL raLe abnormallLles, such as
bradycardla, or LachyarrhyLhmlas such as venLrlcular
Lachycardla, may cause or conLrlbuLe Lo hypoLenslon and
musL be LreaLed.
Acute Card|ogen|c Shock
prlmary goal ls Lo lmprove myocardlal muscle funcLlon
elevaLed Sv8 may also lmpalr cardlac ouLpuL because lL
lncreases afLerload. CfLen ln acuLe cardlogenlc shock, Lhe Sv8
ls secondarlly elevaLed (parL of Lhe barorecepLor response Lo
shock) Lo malnLaln vascular perfuslon pressure
lnoLropes, such as dobuLamlne, are lndlcaLed Lo lncrease
myocardlal conLracLlllLy ln Lhe presence of normal or sllghLly
decreased blood pressure and may have a secondary
beneflclal effecL of decreaslng Sv8 and lmprovlng afLerload.
n8 drlvlng pressure for coronary arLery perfuslon ls
aorLlc dlasLollc pressure (Lhls ls because coronary arLery
perfuslon occurs prlmarlly durlng dlasLole). A low aorLlc
dlasLollc pressure ls common ln severe shock seen ln lCu and
may be genLly lncreased wlLh vasopressors (agenLs LhaL cause
vasoconsLrlcLlon and Lherefore lncrease Sv8). Powever,
because of Lhe lncrease ln afLerload, an agenL LhaL also
lncreases cardlac muscle performance musL also be used, and
lnlLlal Lherapy wlLh a slngle agenL LhaL has boLh lnoLroplc and
vasopressor effecLs (l.e. noreplnephrlne or hlgh-dose
dopamlne) ls lndlcaLed
lf hypoLenslon ls noL responslve Lo lnlLlal Lherapy,
consulLaLlon should be obLalned for conslderaLlon of a
cardlac asslsL devlce such as lnLra-aorLlc balloon
counLerpulsaLlon.
nypovo|em|c Shock
reLurn lnLravascular volume Lo normal
lnlLlal resusclLaLlon:
! collold or crysLallold flulds are effecLlve
cholce of fluld should be based on Lhe fluld
Lype LhaL has been losL. lor example, blood
should replace blood and crysLallold should be
used for vomlLlng and dehydraLlon
because of Lhe lnherenL compllcaLlons of
blood Lransfuslon, mlld Lo moderaLe blood loss
(less Lhan one llLer ln an adulL), should be
replaced by collold (1-1.3 Llmes volume of blood
losL) or crysLallold (crysLallold 2.3-3 Llmes
volume of blood losL)
crysLallold of cholce ls normal sallne or
lactated Ringers solution because its osmolaliLy
ls slmllar Lo LhaL of Lhe lnLravascular volume. ln
large-volume resusclLaLlon, however, excesslve
normal sallne lnfuslon may produce
hyperchloremlc meLabollc acldosls. Collold
soluLlons (3 albumln and heLasLarch) offer Lhe
mosL efflclenL lnLravascular volume expanslon,
buL are expenslve and no ouLcome beneflL has
been shown. uexLrose 3 ln waLer does noL
offer slgnlflcanL expanslon of lnLravascular
volume because lL ls qulckly dlsLrlbuLed
LhroughouL body fluld comparLmenLs.
! endpolnLs of Lherapy are Lo re-esLabllsh normal
blood pressure, pulse, and organ perfuslon.
D|str|but|ve Shock
vasodllaLlon, resulLlng ln a very low Sv8, and dlffuse
caplllary leak are Lhe ma[or feaLures
because of caplllary leakage, hypovolaemla conLrlbuLes
slgnlflcanLly Lo Lhe shock before resusclLaLlon and fluld
requlremenLs may be very large
end polnLs of fluld resusclLaLlon are Lhe same as for
hypovolaemlc shock aL Lhls sLage
lf Lhe paLlenL remalns hypoLenslve desplLe adequaLe fluld
resusclLaLlon (hlgh Cv, pulmonary arLery occluslon pressure,
or pulmonary oedema) lnoLropes and/or vasopressors are
necessary
anaphylacLlc shock ls LreaLed wlLh subcuLaneous
eplnephrlne (0.3-1mg) and volume resusclLaLlon. ln
clrcumsLances of very low blood pressure and poor perlpheral
perfuslon, LlLraLed lnLravenous eplnephrlne (23-30g per
bolus) ls lndlcaLed
acuLe adrenal lnsufflclency ls LreaLed wlLh volume
Lherapy, lnLravenous corLlcosLerolds, and vasopressors.
sepLlc shock
! comblnaLlon of lnoLroplc and vasopressor effecL ls
opLlmal. uopamlne (3 mg/kg/mln and lncreased lf
necessary Lo 13-20mg/kg/mln) or adrenallne
(0.03 mg/kg/mln and lncreased lf necessary Lo
2 mg/kg/mln) provlde boLh vasopressor and lnoLroplc
supporL
! lf mg/kg/mln and lncreased lf necessary Lo
2 mg/kg/mln). 1he addlLlon of dobuLamlne (3-
10 mg/kg/mln) may be beneflclal lf noradrenallne ls used
Cbstruct|ve Shock
rellef of Lhe obsLrucLlon ls llfe savlng
! lf cardlac Lamponade ls presenL, urgenL
perlcardlocenLesls ls essenLlal
! Lenslon pneumoLhorax musL be LreaLed prompLly
wlLh needle LhoracosLomy
! masslve pulmonary embollsm requlres urgenL
Lhrombolysls or surglcal removal
keeplng preload normal ls lmporLanL ln paLlenLs wlLh all
forms of obsLrucLlve shock. lluld resusclLaLlon may lmprove
the patients cardiac output and hypotension temporarily and
buy Llme for deflnlLlve lnLervenLlon.
8. Layers- per|card|ocentes|s
(see lnLegumenLary #6)
9. DV1 treatment
ueep veln Lhrombosls (DV1) ls Lhe formaLlon of a blood
cloL ("Lhrombus") ln a deep veln. ueep veln Lhrombosls
commonly affecLs Lhe leg velns (such as Lhe femoral veln or
Lhe popllLeal veln) or Lhe deep velns of Lhe pelvls.
Cccaslonally Lhe velns of Lhe arm are affecLed (such as
ln ageL-SchrLLer dlsease). A uv1 can occur
wlLhouL sympLoms, buL ln many cases Lhe affecLed exLremlLy
wlll be palnful, swollen, red, and warm, and Lhe superflclal
velns may be engorged. 1he mosL serlous compllcaLlon of a
uv1 ls LhaL Lhe cloL could dlslodge and Lravel Lo Lhe lungs,
whlch ls called a pulmonary embollsm.
Accordlng Lo vlrchow's Lrlad, venous Lhrombosls occurs vla
Lhree mechanlsms: decreased flow raLe of Lhe blood, damage
Lo Lhe blood vessel wall and an lncreased Lendency of Lhe
blood Lo cloL (hypercoagulablllLy). Several medlcal condlLlons
can lead Lo uv1, such as compresslon of Lhe velns, physlcal
Lrauma, cancer, lnfecLlons, cerLaln lnflammaLory dlseases and
speclflc condlLlons such as sLroke, hearL fallure or nephroLlc
syndrome. 1here are several facLors whlch can lncrease a
person's rlsk for uv1, lncludlng surgery, hosplLallzaLlon,
lmmoblllzaLlon (such as when orLhopedlc casLs are used, or
durlng long-haul fllghLs, leadlng Lo Lraveler's
Lhrombosls),smoklng, obeslLy, age, cerLaln drugs (such
as esLrogen, or eryLhropoleLln) and lnborn Lendencles Lo form
cloLs known as Lhrombophllla (for example, ln carrlers
of facLor v Lelden). Women have an lncreased rlsk
durlng pregnancy, lf Lhey are on oral conLracepLlves, and ln
Lhe posLnaLal perlod, due Lo lncreased esLrogen levels.
1he mosL commonly used LesLs for Lhe dlagnosls of uv1 are
a blood LesL called u-dlmers and doppler ulLrasound of Lhe
affecLed velns. SomeLlmes, furLher LesLlng ls requlred Lo flnd
Lhe cause of Lhe uv1. ln speclflc cases, an aLLempL can be
made Lo break down Lhe cloL (uslng LhrombolyLlc agenLs). 1o
prevenL furLher accrual and formaLlon of new cloLs wlLh a rlsk
of pulmonary embollsm, anLlcoagulaLlon (blood Lhlnners) ls
advlsed (lf noL posslble, an lnferlor vena cava fllLer may be
used). revenLlon of uv1 ls advlsed ln many medlcal and
surglcal lnpaLlenLs uslng anLlcoagulanLs, graduaLed
compresslon sLocklngs (also known as Lhromboembollc
deLerrenL sLocklngs) or lnLermlLLenL pneumaLlc
compresslon (lC) devlces.
Ant|coagu|at|on
AnLlcoagulanL medlclnes prevenL a blood cloL from geLLlng
blgger. 1hey can also help sLop parL of Lhe blood cloL from
breaklng off and becomlng lodged ln anoLher parL of your
bloodsLream (an embollsm).
AlLhough Lhey are ofLen referred Lo as "blood-Lhlnnlng"
medlclnes, anLlcoagulanLs do noL acLually Lhln Lhe blood.
1hey alLer chemlcals wlLhln lL, whlch prevenLs cloLs formlng
so easlly.
1wo dlfferenL Lypes of anLlcoagulanLs are used Lo LreaL uv1:
heparln
warfarln
Peparln ls usually prescrlbed flrsL, because lL works
lmmedlaLely Lo prevenL furLher cloLLlng. AfLer Lhls lnlLlal
LreaLmenL you may also need Lo Lake warfarln Lo prevenL
anoLher blood cloL formlng.
nepar|n
Peparln ls avallable ln Lwo dlfferenL forms:
sLandard (unfracLloned) heparln
low molecular welghL heparln (LMWP)
SLandard (unfracLloned) heparln can be glven as:
an |ntravenous |n[ect|on - an ln[ecLlon sLralghL
lnLo one of your velns
an |ntravenous |nfus|on - when a conLlnuous drlp
of heparln ls fed Lhrough a narrow Lube lnLo a
veln ln your arm (Lhls musL be done ln hosplLal)
a subcutaneous |n[ect|on - an ln[ecLlon under
your skln
LMWP ls usually glven as a subcuLaneous ln[ecLlon.
A dose of sLandard heparln can work dlfferenLly from person
Lo person, so Lhe dosage musL be carefully monlLored and
ad[usLed where necessary. ?ou may need Lo sLay ln hosplLal
for flve Lo 10 days and have frequenL blood LesLs Lo ensure
you recelve Lhe rlghL dose.
LMWP works dlfferenLly from sLandard heparln. lL conLalns
small molecules, whlch means lLs effecLs are more rellable
and you wlll noL have Lo sLay ln hosplLal and be monlLored.
8oLh sLandard and LMWP can cause slde effecLs, lncludlng:
a skln rash and oLher allerglc reacLlons
bleedlng
weakenlng of Lhe bones (lf Laken for a long Llme)
ln rare cases, heparln can also cause an exLreme reacLlon LhaL
makes exlsLlng blood cloLs worse and causes new cloLs Lo
develop. 1hls reacLlon, and weakenlng of your bones, ls less
llkely Lo occur when Laklng LMWP.
ln mosL cases, you wlll be glven LMWP because lL ls easler Lo
use and causes fewer slde effecLs.
Warfar|n
Warfarln ls Laken as a LableL. ?ou may need Lo Lake lL afLer an
lnlLlal heparln LreaLmenL Lo prevenL furLher blood cloLs
occurrlng. ?our docLor may recommend LhaL you Lake
warfarln for Lhree Lo slx monLhs. ln some cases, warfarln may
need Lo be Laken for longer, even for llfe.
As wlLh sLandard heparln, Lhe effecLs of warfarln vary from
person Lo person, and you wlll need Lo be closely monlLored
wlLh frequenL blood LesLs Lo ensure you are Laklng Lhe rlghL
dosage.
When you flrsL sLarL Laklng warfarln, you may need Lo have
Lwo Lo Lhree blood LesLs a week unLll your regular dose ls
declded. AfLer Lhls, you should only need Lo have a blood LesL
every four weeks aL an anLlcoagulanL ouLpaLlenL cllnlc.
Warfarln can be affecLed by your dleL, any oLher medlclnes
LhaL you are Laklng, and by how well your llver ls worklng. lf
you are Laklng warfarln, you should:
keep your dleL conslsLenL
llmlL Lhe amounL of alcohol LhaL you drlnk
(no more Lhan Lhree Lo four unlLs a day for
men and Lwo Lo Lhree unlLs a day for
women)
Lake your dose of warfarln aL Lhe same Llme
every day
noL sLarL Lo Lake any oLher medlclne
wlLhouL checklng wlLh your C, pharmaclsL
or anLlcoagulanL speclallsL
noL Lake herbal medlclnes
Warfarln ls noL recommended for pregnanL women. 1hey are
glven heparln ln[ecLlons for Lhe full lengLh of LreaLmenL.
Compress|on stock|ngs
Compresslon sLocklngs help prevenL calf paln and swelllng
and lower Lhe rlsk of ulcers developlng afLer havlng a uv1.
1hey can also help prevenL posL-LhromboLlc syndrome
damage Lo Lhe Llssue of your calf caused by Lhe lncrease ln
blood pressure LhaL occurs when a veln ls blocked (by a cloL)
and blood ls dlverLed Lo Lhe ouLer velns.
AfLer havlng a uv1, sLocklngs should be worn every day for aL
leasL Lwo years because sympLoms of posL-LhromboLlc
syndrome may develop several monLhs, or even years, afLer
havlng uv1.
Compresslon sLocklngs should be flLLed professlonally. 1hey
need Lo be worn all day, buL can be Laken off before golng Lo
bed or ln Lhe evenlng whlle you resL wlLh your leg ralsed.
ka|s|ng your |eg
As well as wearlng compresslon sLocklngs, you mlghL be
advlsed Lo ralse your leg whenever you are resLlng. 1hls helps
Lo relleve Lhe pressure ln Lhe velns of Lhe calf and sLops blood
and fluld poollng ln Lhe calf lLself.
When ralslng your leg, make sure LhaL your fooL ls hlgher Lhan
your hlp. 1hls wlll help Lhe reLurnlng blood flow from your
calf. uLLlng a cushlon underneaLh your leg whlle you
are lylng down should help ralse your leg above Lhe level of
your hlp.
?ou can also sllghLly ralse Lhe end of your bed Lo ensure LhaL
your fooL and calf are sllghLly hlgher Lhan your hlp.
10. CnI cr|ter|a
neart fa||ure (nI) ofLen called congest|ve heart fa||ure
(CnI) ls generally deflned as Lhe lnablllLy of Lhe hearL Lo
supply sufflclenL blood flow Lo meeL Lhe needs of Lhe body.
PearL fallure can cause a number of sympLoms
lncludlng shorLness of breaLh, leg swelllng, andexerclse
lnLolerance. 1he condlLlon ls dlagnosed
wlLh echocardlography and blood LesLs. 1reaLmenL commonly
conslsLs of llfesLyle measures (such as smoklng cessaLlon,
llghL exerclse lncludlng breaLhlng proLocols, decreased salL
lnLake and oLher dleLary changes) and medlcaLlons, and
someLlmes devlces or even surgery.
Common causes of hearL fallure lnclude myocardlal
lnfarcLlon and oLher forms of lschemlc hearL
dlsease, hyperLenslon, valvular hearL dlsease,
and cardlomyopaLhy. 1he Lerm "hearL fallure" ls someLlmes
lncorrecLly used Lo descrlbe oLher cardlac-relaLed lllnesses,
such as myocardlal lnfarcLlon (hearL aLLack) or cardlac arresL,
whlch can cause hearL fallure buL are noL equlvalenL Lo hearL
fallure.
ulagnosls of CPl requlres Lhe slmulLaneous presence of aL
leasL 2 ma[or crlLerla or 1 ma[or crlLerlon ln con[uncLlon wlLh
2 mlnor crlLerla.
Ma[or crlLerla:
aroxysmal nocLurnal dyspnea
neck veln dlsLenLlon
8ales
8adlographlc cardlomegaly (lncreaslng hearL slze
on chesL radlography)
AcuLe pulmonary edema
S3 gallop
lncreased cenLral venous pressure (>16 cm P2C
aL rlghL aLrlum)
PepaLo[ugular reflux
WelghL loss >4.3 kg ln 3 days ln response Lo
LreaLmenL
Mlnor crlLerla:
8llaLeral ankle edema
nocLurnal cough
uyspnea on ordlnary exerLlon
PepaLomegaly
leural effuslon
uecrease ln vlLal capaclLy by one Lhlrd from
maxlmum recorded
1achycardla (hearL raLe>120 beaLs/mln.)
1he lramlngham PearL SLudy crlLerla are 100 senslLlve and
78 speclflc for ldenLlfylng persons wlLh deflnlLe congesLlve
hearL fallure.
11. Iones cr|ter|a
kev|sed Iones Cr|ter|a for Acute kheumat|c Iever (AkI)
A flrm dlagnosls requlres LhaL Lwo ma[or or one ma[or and
Lwo mlnor crlLerla are saLlsfled, ln addlLlon Lo evldence of
recenL sLrepLococcal lnfecLlon.
Ma[or Cr|ter|a
1. CardlLls: All layers of cardlac Llssue are affecLed
(perlcardlum, eplcardlum, myocardlum, endocardlum)
1he paLlenL may have a new or changlng murmur, wlLh
mlLral regurglLaLlon belng Lhe mosL common followed by
aorLlc lnsufflclency.
2. olyarLhrlLls: MlgraLlng arLhrlLls LhaL Lyplcally affecLs Lhe
knees, ankles, elbows and wrlsLs. 1he [olnLs are very
palnful and sympLoms are very responslve Lo anLl-
lnflammaLory medlclnes.
3. Chorea: Also known as Syndenhams chorea, or "SL.
vlLus dance". 1here are abrupL, purposeless movemenLs.
1hls may be Lhe only manlfesLaLlon of A8l and ls lLs
presence ls dlagnosLlc. May also lnclude emoLlonal
dlsLurbances and lnapproprlaLe behavlor.
4. LryLhema marglnaLum: A non-prurlLlc rash LhaL
commonly affecLs Lhe Lrunk and proxlmal exLremlLles,
buL spares Lhe face. 1he rash Lyplcally mlgraLes from
cenLral areas Lo perlphery, and has well-deflned borders.
3. SubcuLaneous nodules: usually locaLed over bones or
Lendons, Lhese nodules are palnless and flrm.
M|nor Cr|ter|a:
1. lever
2. ArLhralgla
3. revlous rheumaLlc fever or rheumaLlc hearL dlsease
4. AcuLe phase reacLanLs: LeukocyLosls, elevaLed
erlLrosedlmenLaLlon raLe (LS8) and C-reacLlve proLeln
(C8)
3. rolonged -8 lnLerval on elecLrocardlogram (LCC)
Lv|dence of preced|ng streptococca| |nfect|on: Any one of
Lhe followlng ls consldered adequaLe evldence of lnfecLlon:
lncreased anLlsLrepLolysln C or oLher sLrepLococcal
anLlbodles
oslLlve LhroaL culLure for Croup A beLa-hemolyLlc
sLrepLococcl
oslLlve rapld dlrecL Croup A sLrep carbohydraLe anLlgen
LesL
12. Advantages of enoxapar|n vs. hepar|n
Lnoxapar|n nepar|n
Lhree Lo flve hours Lo achleve
maxlmum effecLlveness
reaches lLs maxlmum
effecLlveness wlLhln Lwo Lo four
hours afLer Lhe drug ls Laken
someLlmes glven wlLh warfarln
for Lhe LreaLmenL of blood cloLs
cannoL dlssolve cloLs LhaL have
already formed
someLlmes used wlLh ASl8ln
Lo prevenL hearL damage from
anglna or hearL aLLacks
ofLen glven wlLh blood
Lransfuslons.
Peparln and lLs derlvaLlve, low-molecular-welghL heparln
(LMWP), are Lhe anLlcoagulanLs of cholce when a rapld
anLlcoagulanL effecL ls requlred, because Lhelr onseL of acLlon
ls lmmedlaLe when admlnlsLered by lv ln[ecLlon. 8oLh Lypes
of heparlns are admlnlsLered ln lower doses for prlmary
prophylaxls Lhan for LreaLmenL of venous Lhrombosls or acuLe
myocardlal lschemla. Peparln has pharmacoklneLlc
llmlLaLlons noL shared by LMWPs. 8ased on Lhese
pharmacoklneLlc llmlLaLlons, heparln Lherapy ls usually
resLrlcLed Lo Lhe hosplLal seLLlng, where lLs effecL can be
monlLored and lLs dosage ad[usLed frequenLly. ln conLrasL,
LMWP preparaLlons can be admlnlsLered ln elLher Lhe ln-
hosplLal or ouL-of-hosplLal seLLlng because Lhey can be
admlnlsLered subcuLaneously (sc) wlLhouL Lhe need for
laboraLory monlLorlng. When long-Lerm anLlcoagulanL
Lherapy ls lndlcaLed, heparln or LMWP admlnlsLraLlon ls
usually followed by LreaLmenL wlLh oral anLlcoagulanLs.
Powever, long-Lerm ouL-of-hosplLal LreaLmenL wlLh heparln
or LMWP ls used when anLlcoagulanL Lherapy ls lndlcaLed ln
pregnancy and ln paLlenLs who develop recurrenL venous
Lhromboembollsm whlle LreaLed wlLh approprlaLe doses of
oral anLlcoagulanLs.
Peparln ls effecLlve and lndlcaLed for Lhe prevenLlon of
venous Lhromboembollsm, for Lhe LreaLmenL of venous
Lhrombosls and pulmonary embollsm (L), for Lhe early
LreaLmenL of paLlenLs wlLh uA and acuLe myocardlal
lnfarcLlon (Ml), for paLlenLs who undergo cardlac surgery
uslng cardlac bypass, vascular surgery, and coronary
angloplasLy, ln paLlenLs wlLh coronary sLenLs, and ln selecLed
paLlenLs wlLh dlssemlnaLed lnLravascular coagulaLlon.
LMWPs are effecLlve and lndlcaLed for Lhe prevenLlon of
venous Lhromboembollsm, for Lhe LreaLmenL of venous
Lhrombosls, for Lhe LreaLmenL of acuLe L, and for Lhe early
LreaLmenL of paLlenLs wlLh uA.
13. Warfar|n]hepar|n overdose treatment
Peparln Warfarln
SLrucLure Large anlonlc
polymer, acldlc
Small llpld-soluble
molecule
8ouLe of
admlnlsLraLlon
arenLeral (lv, SC) Cral
SlLe of acLlon 8lood Llver
CnseL of
acLlon
8apld (seconds) Slow, llmlLed oL
hal-llves of normal
cloLLlng facLors
MCA AcLlvaLes
anLlLhrombln lll
lmpalrs synLhesls
of vlL k dependenL
cloLLlng facLors ll,
vll, lx, x (vlL k
anLagonlsL)
uuraLlon of
acLlon
AcuLe (hours) Chronlc (weeks or
monLhs)
lnhlblLs
coagulaLlon ln
vlLro
?es no
1reaLmenL of
acuLe
overdose
roLamlne sulfaLe lv vlLamln k and
ll
MonlLorlng a11 (lnLrlnslc) 1 (exLrlnslc)
kesp|ratory
1. hys|o|ogy of breath|ng
8reath|ng cyc|e
(1) AL resL (before lnsplraLlon beglns)
a. Alveolar pressure equals aLmospherlc pressure.
l. 8ecause lung pressures are expressed relaLlve Lo
aLmospherlc pressure, alveolar pressure ls sald Lo
be zero.
ll. lnLrapleural pressure ls negaLlve.
1he opposlng forces of Lhe lungs Lrylng Lo
collapse and Lhe chesL wall Lrylng Lo expand
creaLe a negaLlve pressure ln Lhe
lnLrapleural space beLween Lhem.
lnLrapleural pressure can be measured by a
balloon caLheLer ln Lhe esophagus.
lll. Lung volume ls Lhe l8C.
(2) uurlng lnsplraLlon
a. 1he lnsplraLory muscles conLracL and cause Lhe
volume of Lhe Lhorax Lo lncrease.
l. As lung volume lncreases, alveolar pressure
decreases Lo less Lhan aLmospherlc pressure (l.e.,
becomes negaLlve).
ll. 1he pressure gradlenL beLween Lhe aLmosphere
and Lhe alveoll now causes alr Lo flow lnLo Lhe
lungs, alrflow wlll conLlnue unLll Lhe pressure
gradlenL dlsslpaLes.
b. lnLrapleural pressure becomes more negaLlve.
l. 8ecause lung volume lncreases durlng lnsplraLlon,
Lhe elasLlc recoll sLrengLh of Lhe lungs also
lncreases. As a resulL, lnLrapleural pressure
becomes even more negaLlve Lhan lL was aL resL.
ll. Changes ln lnLrapleural pressure durlng lnsplraLlon
are used Lo measure Lhe dynamlc compllance of
Lhe lungs.
c. Lung volume lncreases by one 1v.
l. AL Lhe peak of lnsplraLlon, lung volume ls Lhe l8C
plus one 1v.
(3) uurlng explraLlon
a. Alveolar pressure becomes greaLer Lhan aLmospherlc
pressure.
l. 1he alveolar pressure becomes greaLer (l.e.,
becomes poslLlve) because alveolar gas ls
compressed by Lhe elasLlc forces of Lhe lung.
ll. 1hus, alveolar pressure ls now hlgher Lhan
aLmospherlc pressure, Lhe pressure gradlenL ls
reversed, and alr flows ouL of Lhe lungs.
b. lnLrapleural pressure reLurns Lo lLs resLlng value
durlng a normal (passlve) explraLlon.
l. Powever, durlng a forced explraLlon, lnLrapleural
pressure acLually becomes poslLlve. 1hls poslLlve
lnLrapleural pressure compresses Lhe alrways and
makes explraLlon more dlfflculL.
ll. ln chronlc obsLrucLlve pulmonary dlsease (CCu),
ln whlch alrway reslsLance lslncreased, paLlenLs
learn to expire slowly with pursed llps to
prevenL Lhe alrway collapse LhaL may occur wlLh a
forced explraLlon.
c. Lung volume reLurns Lo l8C.
2. Cough and sneeze ref|ex
1he funcLlon of boLh Lhe cough reflex and Lhe sneeze reflex ls
Lo dlslodge forelgn maLLer or lrrlLaLlng maLerlal from
resplraLory passages. 1he bronchl and Lhe Lrachea conLaln
sensory recepLors LhaL are senslLlve Lo forelgn parLlcles and
lrrlLaLlng subsLances. 1he cough reflex ls lnlLlaLed wlLh Lhe
sensory recepLors deLecL Lhese subsLances and lnlLlaLe acLlon
poLenLlals LhaL pass along Lhe vagus nerves Lo Lhe medulla
oblongaLa, where Lhe cough reflex ls Lrlggered.
1he movemenLs resulLlng ln a cough occur as follows: abouL
2.3 llLLers (L) of alr are lnsplred, Lhe eplgloLLls closes, and Lhe
vesLlbular folds and vocal cords close LlghLly Lo Lrap Lhe
lnsplred alr ln Lhe lung, Lhe abdomlnal muscles conLracL Lo
force Lhe abdomlnal conLenLs up agalnsL Lhe dlaphragm, and
Lhe muscles of explraLlon conLracL forcefully. As a
consequence, Lhe pressure ln Lhe lungs lncrease Lo abouL 100
mm Pg. 1hen Lhe vesLlbular folds, Lhe vocal cords, and Lhe
eplgloLLls open suddenly, and Lhe alr rushes from Lhe lungs aL
a hlgh veloclLy, carrylng forelgn parLlcles wlLh lL.
1he sneeze reflex ls slmllar Lo Lhe cough reflex, buL lL dlffers
ln several ways. 1he source of lrrlLaLlon LhaL lnlLlaLes Lhe
sneeze reflex ls ln Lhe nasal passages lnsLead of ln Lhe Lrachea
and bronchl, and Lhe acLlon poLenLlals are conducLed along
Lhe Lrlgemlnal nerves Lo Lhe medulla, where Lhe reflex ls
Lrlggered. uurlng Lhe sneeze reflex Lhe uvula and Lhe sofL
palaLe are depressed so Lhe alr ls dlrecLed prlmarlly Lhrough
Lhe nasal passages, alLhough a conslderable amounL passes
Lhrough Lhe oral cavlLy. 1he rapldly flowlng alr dlslodges
parLlculaLe maLLer from Lhe nasal passages and propels lL a
conslderable dlsLance from Lhe nose.
1he mechanlsm of a cough ls as follows:
ulaphragm (phrenlc nerve) and exLernal lnLercosLal
muscles (segmenLal lnLercosLal nerves) conLracL, creaLlng
a negaLlve pressure around Lhe lung.
Alr rushes lnLo Lhe lungs ln order Lo equallse Lhe
pressure.
1he gloLLls closes (recurrenL laryngeal nerve) and Lhe
vocal cords conLracL Lo shuL Lhe larynx.
1he abdomlnal muscles conLracL Lo accenLuaLe Lhe
acLlon of Lhe relaxlng dlaphragm, slmulLaneously, Lhe
oLher explraLory muscles conLracL. 1hese acLlons
lncrease Lhe pressure of alr wlLhln Lhe lungs.
1he vocal cords relax and Lhe gloLLls opens, releaslng alr
aL over 100 mph.
1he bronchl and non-carLllaglnous porLlons of Lhe
Lrachea collapse Lo form sllLs Lhrough whlch Lhe alr ls
forced, whlch clears ouL any lrrlLanLs aLLached Lo Lhe
resplLory llnlng.
SLlmulaLlon of Lhe aurlcular branch of Lhe vagus nerve
supplylng Lhe ear may also ellclL a cough. 1hls ls known as
Arnold's reflex. 8esplraLory muscle weakness, LracheosLomy,
or vocal cord paLhology (lncludlng paralysls or anesLhesla)
may prevenL effecLlve clearlng of Lhe alrways.
1he reflex ls lmpalred ln Lhe person whose abdomlnals and
resplraLory muscles are weak. 1hls problem can be caused by
dlsease condlLlon LhaL lead Lo muscle weakness or paralysls,
by prolonged lnacLlvlLy, or as ouLcome of surgery lnvolvlng
Lhese muscles. 8ed resL lnLerferes wlLh Lhe expanslon of Lhe
chesL and llmlLs Lhe amounL of alr LhaL can be Laken lnLo Lhe
lungs ln preparaLlon for coughlng, maklng Lhe cough weak
and lneffecLlve. 1hls reflex may also be lmpalred by damage
Lo Lhe lnLernal branch of Lhe superlor laryngeal nerve.
1he sneeze reflex can be Lrlggered by even mlld sLlmulaLlon
of Lhe Lhe nasal llnlng. When sLlmulaLed, Lhe recepLors ln Lhe
llnlng send lmpulses vla Lhe flfLh cranlal nerve (Cn v /
Lrlgemlnal nerve) Lo sneezlng cenLer ln Lhe medulla. 1hls
Lrlggers Lhe sneeze reflex whlch ls slmllar Lo Lhe cough reflex,
wlLh Lhe dlfference belng LhaL alr ls forced ouL malnly Lhrough
Lhe nose by depresslng Lhe uvula.
8apld lnsplraLlon fllls Lhe lung wlLh exLra alr. 1he eplgloLLls
and Lhe vocal cords close LlghLly Lo bulld up pressure ln Lhe
lungs. 1he explraLory muscles of resplraLlon as well as
accessory resplraLory muscles conLracL forcefully. 1hls furLher
lncreases Lhe pressure ln Lhe lungs. Cnce a sufflclenLly hlgh
pressure ls reached, Lhe vocal cords relax, Lhe eplgloLLls
opens and Lhe alr rushes ouL rapldly.
uue Lo Lhe speed of Lhe movlng alr, Lhe Lermlnal parLs of Lhe
alrway lnvaglnaLes Lhereby creaLlng sllLswhlch furLher
lncreases Lhe pressure of Lhe explred alr. 1he depressed uvula
ln a sneeze reflex pushes Lhe alr ouL Lhough Lhe nose. 1hls
enLlre process happens wlLhln seconds. !usL as wlLh a cough,
Lhe speed of Lhe alr rushlng ouL Lhrough Lhe nose can be
close Lo 100mph.
Common sLlmulaLlon and LlghLly shuLLlng Lhe eyes
whlle sneezlng, may cause Lhe lacrlmal glands (Lear
glands) Lo empLy lLs conLenLs Lhereby resulLlng ln sllghLly
waLery eyes wlLh sneezlng. 1he lrrlLaLlon of Lhe nasal
passages Lrlggers Lhe lnflammaLory response whlch causes
mucus hypersecreLlon. 1hls excess mucus ls also forced ouL
durlng a sneeze ln an aerosol fashlon.
3. Musc|es of resp|rat|on
Muscles of lnsplraLlon
a. ulaphragm
l. Lhe mosL lmporLanL muscle for lnsplraLlon.
ll. When Lhe dlaphragm conLracLs, Lhe abdomlnal
conLenLs are pushed downward, and Lhe rlbs are
llfLed upward and ouLward, lncreaslng Lhe volume
of Lhe Lhoraclc cavlLy.
b. lnLercosLals and accessory muscles
l. noL used for lnsplraLlon durlng normal quleL
breaLhlng.
ll. are used durlng exerclse and ln resplraLory
dlsLress.
Muscles of explraLlon
a. LxplraLlon ls normally passlve.
b. 8ecause Lhe lungchesL wall sysLem ls elasLlc, lL
reLurns Lo lLs resLlng poslLlon afLer lnsplraLlon.
c. LxplraLory muscles are used durlng exerclse or when
alrway reslsLance ls lncreased because of dlsease
l. Abdomlnal muscles
1. compress Lhe abdomlnal cavlLy, push Lhe
dlaphragm up, and push alr ouL of Lhe
lungs.
ll. lnLernal lnLercosLal muscles pull Lhe rlbs
downward and lnward
Você também pode gostar
- CLINICAL CHEMISTRY: Passbooks Study GuideNo EverandCLINICAL CHEMISTRY: Passbooks Study GuideAinda não há avaliações
- Legal Medicine Summary by Olarte PDFDocumento22 páginasLegal Medicine Summary by Olarte PDFucbscholarship office100% (2)
- Neurologic Differential Diagnosis - A Case-Based Approach CNVTD PDFDocumento1.196 páginasNeurologic Differential Diagnosis - A Case-Based Approach CNVTD PDFIoana Moraru100% (1)
- Chapter 42 - Sepsis, Septic Shock, and Multiple Organ FailureDocumento15 páginasChapter 42 - Sepsis, Septic Shock, and Multiple Organ FailureWorrawalun FuktongAinda não há avaliações
- Haem. Notes (MBCHB) ProperDocumento162 páginasHaem. Notes (MBCHB) ProperKelvinTMaikanaAinda não há avaliações
- Blood Coagulation StudiesDocumento14 páginasBlood Coagulation Studiesjlb0711Ainda não há avaliações
- Kidney Function TestDocumento19 páginasKidney Function Testbeena gracelyn sarahAinda não há avaliações
- Spinal Cord Anatomy MCQ'S: A) Biceps ReflexDocumento4 páginasSpinal Cord Anatomy MCQ'S: A) Biceps ReflexTahir Aziz100% (2)
- Oncology Revision: Paul BaillieDocumento299 páginasOncology Revision: Paul BaillieMourian AmanAinda não há avaliações
- Clinical Chemistry EnzymeDocumento8 páginasClinical Chemistry EnzymeFrances del RosarioAinda não há avaliações
- Examination of UrineDocumento7 páginasExamination of UrineDaniel LamasonAinda não há avaliações
- Clinical Chemistry (Lecture) - PrelimsDocumento12 páginasClinical Chemistry (Lecture) - Prelimsisprikitik3100% (1)
- Defining The Practice of Medical Technology or Clinical Laboratory Science ProfessionDocumento27 páginasDefining The Practice of Medical Technology or Clinical Laboratory Science ProfessionKianna TicsayAinda não há avaliações
- Electrocardiogram (Ecg or Ekg) : - 2 Components of ELECTRODESDocumento4 páginasElectrocardiogram (Ecg or Ekg) : - 2 Components of ELECTRODESDhanNie CenitaAinda não há avaliações
- Non Protein CompoundsDocumento64 páginasNon Protein CompoundsAbigail Mayled LausAinda não há avaliações
- Hematology NotesDocumento4 páginasHematology NotesHannah Grace CorveraAinda não há avaliações
- Spinal Cord AnatomyDocumento20 páginasSpinal Cord AnatomyrooparawatAinda não há avaliações
- BLOOD PresentationDocumento33 páginasBLOOD PresentationLezlie Jane SahaliAinda não há avaliações
- Anatomy and Physiology, Heart, BP and Hematology Labs MoodleDocumento70 páginasAnatomy and Physiology, Heart, BP and Hematology Labs MoodleLeena LapenaAinda não há avaliações
- Neuro Assessment ReviwerDocumento51 páginasNeuro Assessment ReviwerKim RamosAinda não há avaliações
- Blood Grouping ReagentsDocumento7 páginasBlood Grouping ReagentsDominic EmerencianaAinda não há avaliações
- Introduction To OrthopaedicsDocumento42 páginasIntroduction To Orthopaedicsgus_lions100% (1)
- Transfusion Reaction and Coombs Test: Moderator:-Dr Sanjay Agrwal Presenter: - DR Pratima Singh PG Jr-1Documento33 páginasTransfusion Reaction and Coombs Test: Moderator:-Dr Sanjay Agrwal Presenter: - DR Pratima Singh PG Jr-1UmikaguptaAinda não há avaliações
- Asthma and CopdDocumento44 páginasAsthma and CopdBeer Dilacshe100% (1)
- NO Hazard Slight Moderate Serious Extreme: Hazard Hazard Hazard HazardDocumento74 páginasNO Hazard Slight Moderate Serious Extreme: Hazard Hazard Hazard HazardCristy Jean100% (1)
- Unit-Two Biological Bases of BehaviorDocumento27 páginasUnit-Two Biological Bases of Behaviorरोशन सिग्देलAinda não há avaliações
- Clinical KardexDocumento2 páginasClinical KardexJackie Frey100% (2)
- Hemodynamic Disturbances: Dr. Dhamyaa Al-RahalDocumento74 páginasHemodynamic Disturbances: Dr. Dhamyaa Al-RahalAmmar Bany AtaAinda não há avaliações
- ImmunityDocumento70 páginasImmunityisprikitik30% (2)
- Microanatomy pt1Documento27 páginasMicroanatomy pt1poopziAinda não há avaliações
- Chapter 14 Neurologic Disorders Study Guide Outline #2Documento12 páginasChapter 14 Neurologic Disorders Study Guide Outline #2Del Delgado100% (1)
- Saumya Gupta Moderator: Dr. Vishal GuptaDocumento41 páginasSaumya Gupta Moderator: Dr. Vishal Guptaimranqazi11Ainda não há avaliações
- 18 - Flow Cytometry and Introduction To Molecular PathologyDocumento11 páginas18 - Flow Cytometry and Introduction To Molecular Pathologyhamadadodo7Ainda não há avaliações
- Combined Hormone Pill, Patch, Ring Progestin Only Mini Pill, Depo-Provera, IUDDocumento1 páginaCombined Hormone Pill, Patch, Ring Progestin Only Mini Pill, Depo-Provera, IUDnkuligowskiAinda não há avaliações
- Pleural CollectionsDocumento30 páginasPleural CollectionsRitam JoarderAinda não há avaliações
- Synovial Fluid and Fecal Analysis .Group 5Documento39 páginasSynovial Fluid and Fecal Analysis .Group 5John Alfrey Dondiego PuebloAinda não há avaliações
- Hematology PreliminariesDocumento7 páginasHematology PreliminariesRomie SolacitoAinda não há avaliações
- Classification of The Epilepsies: Purpose: For Clinical DiagnosisDocumento25 páginasClassification of The Epilepsies: Purpose: For Clinical Diagnosisayu rifqiAinda não há avaliações
- Anatomy and Physiology Musculoskeletal System Chap 6 - 2401Documento18 páginasAnatomy and Physiology Musculoskeletal System Chap 6 - 2401slyfoxkittyAinda não há avaliações
- Review SlidesDocumento91 páginasReview SlidesomyomarAinda não há avaliações
- Blood TransfusonDocumento22 páginasBlood TransfusonArmandoAinda não há avaliações
- Lab Values and Vital SignsDocumento4 páginasLab Values and Vital SignsWole Olaluwoye100% (1)
- UrinalysisDocumento9 páginasUrinalysisSukma EffendyAinda não há avaliações
- Clearance and GFR: Major DR Arabinda Mohan Bhattarai Lecturer (Biochemistry), NAIHSDocumento25 páginasClearance and GFR: Major DR Arabinda Mohan Bhattarai Lecturer (Biochemistry), NAIHSChandan SahAinda não há avaliações
- Dracunculus MedinensisDocumento1 páginaDracunculus MedinensisEm KayAinda não há avaliações
- Trace Elements and Porphyrins - JBDocumento7 páginasTrace Elements and Porphyrins - JBVinAinda não há avaliações
- Clin Path Trans 3.05 Urinalysis (2b)Documento6 páginasClin Path Trans 3.05 Urinalysis (2b)Reymart FernandezAinda não há avaliações
- Blood Exercises (PHYANA LAB)Documento53 páginasBlood Exercises (PHYANA LAB)Juan CarlosAinda não há avaliações
- ElecrolytesDocumento4 páginasElecrolytesKrizzia Allyssa CotingjoAinda não há avaliações
- Cardiac Function Tests: Example: Normal Formula LDH 1 2 0.5 LDH 2 4Documento1 páginaCardiac Function Tests: Example: Normal Formula LDH 1 2 0.5 LDH 2 4Ritz CelsoAinda não há avaliações
- At HemoglobinDocumento2 páginasAt HemoglobinzulfiAinda não há avaliações
- Red Blood Cells "Best Module Ever"Documento4 páginasRed Blood Cells "Best Module Ever"Jose Emmanuel Dolor100% (1)
- 4 - HemoglobinopathiesDocumento19 páginas4 - HemoglobinopathiesHamzehAinda não há avaliações
- 4 Blood ProductsDocumento11 páginas4 Blood ProductsGampa VijaykumarAinda não há avaliações
- Safety of High Alert MedicationDocumento48 páginasSafety of High Alert Medicationrini setyawatiAinda não há avaliações
- Cell Inclusions: John SantangeloDocumento45 páginasCell Inclusions: John Santangelosaint5470Ainda não há avaliações
- Blood Tubes and Labeling GuidelinesDocumento2 páginasBlood Tubes and Labeling GuidelinesbluetealAinda não há avaliações
- Hemolytic DiseaseDocumento10 páginasHemolytic DiseaseChino Paolo SamsonAinda não há avaliações
- SGOT ASAT Kit Reitman Frankel MethodDocumento3 páginasSGOT ASAT Kit Reitman Frankel MethodShribagla MukhiAinda não há avaliações
- DR - Kim File 3Documento70 páginasDR - Kim File 3Tanveer HamidAinda não há avaliações
- Study Guide Hematologic AssessmentDocumento5 páginasStudy Guide Hematologic AssessmentNancy LemusAinda não há avaliações
- Sources of Errors in Clinical ChemistryDocumento9 páginasSources of Errors in Clinical Chemistrykalantan23Ainda não há avaliações
- Urine AnalysisDocumento63 páginasUrine AnalysisVench DemicaisAinda não há avaliações
- Leukemia - Pathophysiology of White Cells DisordersDocumento10 páginasLeukemia - Pathophysiology of White Cells DisordersJacecosmozAinda não há avaliações
- OncologyDocumento5 páginasOncologymitzi019Ainda não há avaliações
- WBC ReviewDocumento6 páginasWBC Reviewsmoore1234Ainda não há avaliações
- (F) Chapter 11 - Principles of Antimicrobial Action and ResistanceDocumento6 páginas(F) Chapter 11 - Principles of Antimicrobial Action and ResistanceGerald John PazAinda não há avaliações
- Collection TubeDocumento6 páginasCollection TubeChristiane ReaAinda não há avaliações
- Clinical Chemistry IDocumento8 páginasClinical Chemistry IMariel AbatayoAinda não há avaliações
- Evaluation - For External Trainings 06222017Documento1 páginaEvaluation - For External Trainings 06222017isprikitik3Ainda não há avaliações
- Drugs Mechanism of Action Indication Contraindication Adverse EffectsDocumento2 páginasDrugs Mechanism of Action Indication Contraindication Adverse Effectsisprikitik3Ainda não há avaliações
- Ao Final ProgramDocumento16 páginasAo Final Programisprikitik3Ainda não há avaliações
- Biochemistry 1.6 - ABO Blood Typing and Crossmatching (A1 Group 6)Documento68 páginasBiochemistry 1.6 - ABO Blood Typing and Crossmatching (A1 Group 6)isprikitik3Ainda não há avaliações
- God's Creation: Christianity Is An Abrahamic, Monotheistic Religion Based On The Life and OralDocumento2 páginasGod's Creation: Christianity Is An Abrahamic, Monotheistic Religion Based On The Life and Oralisprikitik3Ainda não há avaliações
- Recommendation LetterDocumento1 páginaRecommendation Letterisprikitik3Ainda não há avaliações
- Crown Lengthening of ToothDocumento4 páginasCrown Lengthening of Toothisprikitik3Ainda não há avaliações
- Request LetterDocumento1 páginaRequest Letterisprikitik3Ainda não há avaliações
- Individual Reflections Format (CPH)Documento2 páginasIndividual Reflections Format (CPH)isprikitik3Ainda não há avaliações
- MycologyDocumento3 páginasMycologyisprikitik3Ainda não há avaliações
- Must Knows IIDocumento3 páginasMust Knows IIisprikitik3Ainda não há avaliações
- Carbohydrates 2Documento37 páginasCarbohydrates 2isprikitik3Ainda não há avaliações
- Human Anatomy Lab Manual 1612818025. - PrintDocumento219 páginasHuman Anatomy Lab Manual 1612818025. - Printmishraadityaraj516Ainda não há avaliações
- Nervous System Part 1Documento11 páginasNervous System Part 1Mariel AbatayoAinda não há avaliações
- SHENIBLOG-Class 10 Biology Focus Area Covered Notes (Eng Med) All Chapters 2022Documento16 páginasSHENIBLOG-Class 10 Biology Focus Area Covered Notes (Eng Med) All Chapters 2022kailaskrishnaushusAinda não há avaliações
- Physio Uhs Solved Past Papers 2nd Year Mbbs WWW Edu Apnafort ComDocumento130 páginasPhysio Uhs Solved Past Papers 2nd Year Mbbs WWW Edu Apnafort ComHamza AhmedAinda não há avaliações
- Pinal Stenosis TreatmentDocumento10 páginasPinal Stenosis Treatmentravideva84Ainda não há avaliações
- Anatomy Practical OSPEDocumento33 páginasAnatomy Practical OSPEAbdi Ñãśìr Møhàmèď ŚàĺàhAinda não há avaliações
- University of Cambridge International Examinations International General Certificate of Secondary EducationDocumento20 páginasUniversity of Cambridge International Examinations International General Certificate of Secondary EducationShivraj NaikAinda não há avaliações
- Nervous Tissue List of TermsDocumento7 páginasNervous Tissue List of TermsMARKUS GERARD REYESAinda não há avaliações
- Medical NeurobiologyDocumento682 páginasMedical NeurobiologyMaría CristinaAinda não há avaliações
- Nursing Care Plan Orthopedic Philipine CenterDocumento4 páginasNursing Care Plan Orthopedic Philipine CenterAnonymous NZTQVgjaAinda não há avaliações
- BioRIDPaper PDFDocumento6 páginasBioRIDPaper PDFCristi AntonAinda não há avaliações
- Chart Showing The Classification of Human Nervous SystemDocumento6 páginasChart Showing The Classification of Human Nervous Systemamala raviAinda não há avaliações
- Development of The Nervous System Spinal CordDocumento41 páginasDevelopment of The Nervous System Spinal CordAleksandarTrenovskiAinda não há avaliações
- Question Week 5Documento9 páginasQuestion Week 5I'zzat AndikaAinda não há avaliações
- Review of The Nervous SystemDocumento38 páginasReview of The Nervous SystemNan'EsiPessehAinda não há avaliações
- 2ND Period 1 PDFDocumento2 páginas2ND Period 1 PDFRëönärüdö KmpöAinda não há avaliações
- Efficacy of Muscle Energy Technique Versus MyofascialDocumento7 páginasEfficacy of Muscle Energy Technique Versus Myofascialmuhammad yaminAinda não há avaliações
- Embriologi, Neuroanatomi, Neurofisiologi Medulla SpinalisDocumento60 páginasEmbriologi, Neuroanatomi, Neurofisiologi Medulla SpinalisNadia Vinka LisdiantiAinda não há avaliações
- The Spinal Cord and Spinal NervesDocumento33 páginasThe Spinal Cord and Spinal NervesRushaida AminullaAinda não há avaliações
- Human Physiology From Cells To Systems 4Th Ed Edition Sherwood Full ChapterDocumento67 páginasHuman Physiology From Cells To Systems 4Th Ed Edition Sherwood Full Chapteraudra.rossetti281100% (6)
- Biology Nervous SystemDocumento5 páginasBiology Nervous SystemFatima PueblaAinda não há avaliações
- Nervous System OverviewDocumento5 páginasNervous System Overviewapi-306398192Ainda não há avaliações