Você também pode gostar
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Parathyroid Glands: Presented By: Dr. Mohammed Alshehri Pgy2Documento28 páginasParathyroid Glands: Presented By: Dr. Mohammed Alshehri Pgy2Omar Alruwaili100% (1)
- Patho AsthmaDocumento1 páginaPatho AsthmaAyel JimenezAinda não há avaliações
- 07 - Sudden Plays A Hand (1950)Documento206 páginas07 - Sudden Plays A Hand (1950)ShaziaAshrafAinda não há avaliações
- 01 - Sudden - Outlawed (1935)Documento223 páginas01 - Sudden - Outlawed (1935)ShaziaAshrafAinda não há avaliações
- 02 - Sudden (1933)Documento339 páginas02 - Sudden (1933)ShaziaAshrafAinda não há avaliações
- History and Admiralty Jurisdiction of The High Court in IndiaDocumento9 páginasHistory and Admiralty Jurisdiction of The High Court in IndiaShaziaAshrafAinda não há avaliações
- ITLOS - Admiralty JurisdictionDocumento13 páginasITLOS - Admiralty JurisdictionShaziaAshrafAinda não há avaliações
- The Immunity of State Owned Vessels From Maritime ArrestsDocumento7 páginasThe Immunity of State Owned Vessels From Maritime ArrestsShaziaAshrafAinda não há avaliações
- Compensation Claims Under WorkmenDocumento10 páginasCompensation Claims Under WorkmenBijay Krishna DasAinda não há avaliações
- Role of Non-Governmental Organizations in Environment Conservation - The Indian ScenarioDocumento18 páginasRole of Non-Governmental Organizations in Environment Conservation - The Indian ScenarioShaziaAshrafAinda não há avaliações
- Deletion Od Article 32 Is UnconstituionalDocumento2 páginasDeletion Od Article 32 Is UnconstituionalShaziaAshrafAinda não há avaliações
- Combination Hyperbaric Oxygen and Temozolomide Therapy in c6 Rat Glioma ModelDocumento5 páginasCombination Hyperbaric Oxygen and Temozolomide Therapy in c6 Rat Glioma ModelDICKY PANDUWINATAAinda não há avaliações
- Land of NodDocumento7 páginasLand of NodMaltesers1976Ainda não há avaliações
- Department of Obstetrics and Gynecology FinalDocumento42 páginasDepartment of Obstetrics and Gynecology Finalkremlin23455Ainda não há avaliações
- Paedia - Dr. RehabDocumento173 páginasPaedia - Dr. RehabMohammed Saad NabhanAinda não há avaliações
- Nursing Care Plan Placenta PreviaDocumento2 páginasNursing Care Plan Placenta PreviaApril Ann HortilanoAinda não há avaliações
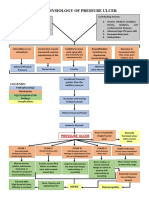
- Pathophysiology of Pressure UlcerDocumento1 páginaPathophysiology of Pressure UlcerSTORAGE FILEAinda não há avaliações
- Proton Pump Inhibitors, Adverse Events and Increased Risk of MortalityDocumento36 páginasProton Pump Inhibitors, Adverse Events and Increased Risk of MortalityMohammad Mahmudur RahmanAinda não há avaliações
- Annals of Thyroid ResearchDocumento2 páginasAnnals of Thyroid ResearchAustin Publishing GroupAinda não há avaliações
- Aches and Pains in The ElderlyDocumento34 páginasAches and Pains in The ElderlyAna CampeanuAinda não há avaliações
- What Is An Obstetric Fistula?Documento5 páginasWhat Is An Obstetric Fistula?abyAinda não há avaliações
- NCP PryllDocumento6 páginasNCP PryllpjcolitaAinda não há avaliações
- JACC Volume 78, Issue 11 SeptemberDocumento122 páginasJACC Volume 78, Issue 11 SeptemberFareesha KhanAinda não há avaliações
- Ã'Tia' Fiakdkdhl Úohd, H - FLD U 07: D.S. Senanayake College - Colombo 07Documento12 páginasÃ'Tia' Fiakdkdhl Úohd, H - FLD U 07: D.S. Senanayake College - Colombo 07joker boyAinda não há avaliações
- Acetylcholine Esterase AntibodyDocumento2 páginasAcetylcholine Esterase AntibodySrinivasanAinda não há avaliações
- Treatment of Portal HypertensionDocumento10 páginasTreatment of Portal HypertensionLourianne NcAinda não há avaliações
- Child Abuse Nursing Care PlansDocumento7 páginasChild Abuse Nursing Care PlansMAHESH KOUJALAGIAinda não há avaliações
- Syphilis Symptoms, Causes, and DiagnosisDocumento3 páginasSyphilis Symptoms, Causes, and DiagnosisIndra FahleviAinda não há avaliações
- Thyroid Hormone Profile in Chronic Kidney DiseaseDocumento6 páginasThyroid Hormone Profile in Chronic Kidney DiseaserefaAinda não há avaliações
- Annotated-Research 20paperDocumento7 páginasAnnotated-Research 20paperapi-667261947Ainda não há avaliações
- NCM 104 RLE Module 3 FinalsDocumento22 páginasNCM 104 RLE Module 3 FinalsAlexander DontonAinda não há avaliações
- Colon Large Intestine: ColorectalDocumento3 páginasColon Large Intestine: ColorectalAlina AldeaAinda não há avaliações
- Acute Suppurative Parotitis: Related SummariesDocumento7 páginasAcute Suppurative Parotitis: Related SummariesFarida Dwi IrnawatiAinda não há avaliações
- Rickettsia eDocumento10 páginasRickettsia eDeep Iyaz100% (1)
- Lapp Jan2020Documento88 páginasLapp Jan2020Siti RojanahAinda não há avaliações
- C-Reactive Protein in Serum by NephelometryDocumento12 páginasC-Reactive Protein in Serum by NephelometryTrajceAinda não há avaliações
- Midterm Activity ScitechDocumento3 páginasMidterm Activity ScitechKean KaiAinda não há avaliações
- Drug Study FINALDocumento32 páginasDrug Study FINALhomeworkping1Ainda não há avaliações
- Pathophys RespDocumento38 páginasPathophys RespSabrina LavegaAinda não há avaliações