Você também pode gostar
- Facs ProtocolDocumento7 páginasFacs ProtocolmisterxAinda não há avaliações
- Whole Cell ExtractDocumento1 páginaWhole Cell Extractbiotech_vidhyaAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
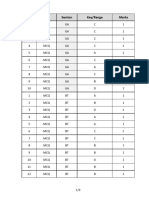
- Q.No. Type Section Key/Range MarksDocumento3 páginasQ.No. Type Section Key/Range Marksbiotech_vidhyaAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- BT 2019Documento13 páginasBT 2019biotech_vidhyaAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- TNPSC Group 1 Prelim Book List PDFDocumento2 páginasTNPSC Group 1 Prelim Book List PDFbiotech_vidhyaAinda não há avaliações
- Polymerasen GuideDocumento16 páginasPolymerasen Guidebiotech_vidhyaAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Stripping For ReprobingDocumento2 páginasStripping For ReprobingStella SalvatoreAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Stripping For ReprobingDocumento2 páginasStripping For ReprobingStella SalvatoreAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Troubleshooting SDS-PAGE 1Documento3 páginasTroubleshooting SDS-PAGE 1biotech_vidhyaAinda não há avaliações
- Polymerase Chain Reaction (PCR)Documento3 páginasPolymerase Chain Reaction (PCR)biotech_vidhyaAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Brad FordDocumento12 páginasBrad FordQi ChaoAinda não há avaliações
- TNPSC Group 1 Prelim Book List PDFDocumento2 páginasTNPSC Group 1 Prelim Book List PDFbiotech_vidhyaAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- SDS PageDocumento2 páginasSDS Pagebiotech_vidhyaAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Components Reaction MixtureDocumento3 páginasComponents Reaction Mixturebiotech_vidhyaAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- Buffer Preparation Guide for DNA/Protein Work (Shi LabDocumento6 páginasBuffer Preparation Guide for DNA/Protein Work (Shi Labbiotech_vidhyaAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Buffer Preparation Guide for DNA/Protein Work (Shi LabDocumento6 páginasBuffer Preparation Guide for DNA/Protein Work (Shi Labbiotech_vidhyaAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Qpaper PondyDocumento21 páginasQpaper Pondybiotech_vidhyaAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- Nuclear ExtractsDocumento2 páginasNuclear Extractsbiotech_vidhyaAinda não há avaliações
- TDC 41597 A (Mechanical Engg.) - 2012Documento20 páginasTDC 41597 A (Mechanical Engg.) - 2012biotech_vidhyaAinda não há avaliações
- Img Word-To PDFDocumento3 páginasImg Word-To PDFbiotech_vidhyaAinda não há avaliações
- Ies 17 Set A Me Q ADocumento67 páginasIes 17 Set A Me Q Abiotech_vidhyaAinda não há avaliações
- TNPSC Group 1 Prelim Book List PDFDocumento2 páginasTNPSC Group 1 Prelim Book List PDFbiotech_vidhyaAinda não há avaliações
- ESE 2017 Mechanical Engineering Prelims Exam Detailed SolutionDocumento52 páginasESE 2017 Mechanical Engineering Prelims Exam Detailed SolutionpataAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Mechanical Engineering Code No. 14: Combined Competitive (Preliminary) Examination, 2010Documento20 páginasMechanical Engineering Code No. 14: Combined Competitive (Preliminary) Examination, 2010biotech_vidhyaAinda não há avaliações
- Befcv List PDFDocumento22 páginasBefcv List PDFbiotech_vidhyaAinda não há avaliações
- A.E. (Mechanical Engineering I) 2007Documento24 páginasA.E. (Mechanical Engineering I) 2007Mukesh KumarAinda não há avaliações
- Qpaper PondyDocumento21 páginasQpaper Pondybiotech_vidhyaAinda não há avaliações
- 1 TolerancesDocumento1 página1 Tolerancesbiotech_vidhyaAinda não há avaliações
- Recruitment RulesDocumento5 páginasRecruitment Rulesbiotech_vidhyaAinda não há avaliações
- Part and Mold Design GuideDocumento170 páginasPart and Mold Design GuideminhtintinAinda não há avaliações
- CBSE Class 4 Social Studies Worksheet - Means of TransportDocumento4 páginasCBSE Class 4 Social Studies Worksheet - Means of TransportNancy Amelia RosaAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Bleeding DisorderDocumento3 páginasBleeding DisorderyanzwinerAinda não há avaliações
- Publications On Multimorbidity 01 PDFDocumento146 páginasPublications On Multimorbidity 01 PDFWalter MendozaAinda não há avaliações
- 3D CD Technique Completes Dentures in 3 Days for ElderlyDocumento5 páginas3D CD Technique Completes Dentures in 3 Days for ElderlyMaulida Dara HarjantiAinda não há avaliações
- Merck Veterinary ManualDocumento264 páginasMerck Veterinary Manualschmooshie91% (11)
- ProjectDocumento64 páginasProjectPradip DindaAinda não há avaliações
- Retinopathy of Prematurity Handout FormatDocumento31 páginasRetinopathy of Prematurity Handout FormatkaznielsAinda não há avaliações
- Scott-Sinema Medicare Advantage LetterDocumento2 páginasScott-Sinema Medicare Advantage LetterRachel CohrsAinda não há avaliações
- UTI in PregnancyDocumento47 páginasUTI in PregnancyAli MahmoudAinda não há avaliações
- Good Medical Practice Nov12 - 2019Documento13 páginasGood Medical Practice Nov12 - 2019Fransiscus RivaldyAinda não há avaliações
- Health Information SystemDocumento14 páginasHealth Information SystemRoberto MendozaAinda não há avaliações
- Brazilian Sanitary Guide For Cruise ShipsDocumento82 páginasBrazilian Sanitary Guide For Cruise ShipsStanislav KozhuharovAinda não há avaliações
- Interpretation: L63 - Ankit Jain Sagar Cc-3 I/F HDFC Bank Parkota Ward Goughat SAGAR-470002 M.PDocumento2 páginasInterpretation: L63 - Ankit Jain Sagar Cc-3 I/F HDFC Bank Parkota Ward Goughat SAGAR-470002 M.PAviral SinghAinda não há avaliações
- The Lancet, 2018Documento70 páginasThe Lancet, 2018dessyAinda não há avaliações
- Froelich Syndrome and HomoeopathyDocumento13 páginasFroelich Syndrome and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- LECTURE 4 Introduction To MicrobiologyDocumento36 páginasLECTURE 4 Introduction To MicrobiologyArcee Feb Dela PazAinda não há avaliações
- Gross Pathology SpringerDocumento2 páginasGross Pathology SpringerThalia ChristabelAinda não há avaliações
- Cdi Reviewer MidtermDocumento8 páginasCdi Reviewer MidtermKIMBERLY MARGARETTE REDAinda não há avaliações
- Pulmonary Embolism: Presented By: Miss. M.K.Kaku Nursing TutorDocumento9 páginasPulmonary Embolism: Presented By: Miss. M.K.Kaku Nursing TutorKaku ManishaAinda não há avaliações
- Dr. Khalid - S Explanation of 1700 MCQ1Documento683 páginasDr. Khalid - S Explanation of 1700 MCQ1heba100% (1)
- Form 3 - Patient Care Report (PCR) FormDocumento2 páginasForm 3 - Patient Care Report (PCR) FormMdrrmo Pamplona Camarines SurAinda não há avaliações
- Database Management SystemDocumento12 páginasDatabase Management Systemaklesh parteAinda não há avaliações
- TubercolosisDocumento8 páginasTubercolosisNitesh Bhura100% (1)
- MCQ Exam 2Documento13 páginasMCQ Exam 2Anwaar YousafAinda não há avaliações
- Daftar Max - Min Obat / Barang di ApotekDocumento38 páginasDaftar Max - Min Obat / Barang di ApotekMeta JuliaAinda não há avaliações
- Herbalage Products KnowledgeDocumento25 páginasHerbalage Products Knowledgemail9246Ainda não há avaliações
- Test Bank of Neurocognitive DisordersDocumento27 páginasTest Bank of Neurocognitive DisordersmAinda não há avaliações
- Đề Cương Môn Tiếng Anh Chuyên Ngành Ngành: DượcDocumento11 páginasĐề Cương Môn Tiếng Anh Chuyên Ngành Ngành: DượcNguyễn Thị Hương75% (8)
- Work in Team EnvironmentDocumento50 páginasWork in Team EnvironmentMercy Dadulla - ElvinaAinda não há avaliações
- Endophthalmitis 1Documento42 páginasEndophthalmitis 1Nasrin sultana rmcAinda não há avaliações
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNo EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNota: 4 de 5 estrelas4/5 (402)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingNo EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingNota: 5 de 5 estrelas5/5 (4)
- The Age of Magical Overthinking: Notes on Modern IrrationalityNo EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityNota: 4 de 5 estrelas4/5 (13)
- The Happiness Trap: How to Stop Struggling and Start LivingNo EverandThe Happiness Trap: How to Stop Struggling and Start LivingNota: 4 de 5 estrelas4/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeAinda não há avaliações
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNo EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNota: 3.5 de 5 estrelas3.5/5 (3)