Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Leaf Structure WorksheetDocumento1 páginaLeaf Structure Worksheetapi-309893409100% (1)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Sample SOP For Biotechnology in CanadaDocumento3 páginasSample SOP For Biotechnology in CanadaAlbert MarreddyAinda não há avaliações
- Virtual Lab Report: Name of The SimulationDocumento12 páginasVirtual Lab Report: Name of The SimulationBruce PanAinda não há avaliações
- Lesson Plan - DNA Replication (REVISED)Documento6 páginasLesson Plan - DNA Replication (REVISED)Keziah ValenzuelaAinda não há avaliações
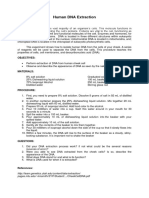
- Human DNA ExtractionDocumento1 páginaHuman DNA ExtractionJosaphat M. AnteAinda não há avaliações
- Class 3rdDocumento16 páginasClass 3rdJude Chisom Jnr NwaugoAinda não há avaliações
- Igments IN Lants: Betalains: What Are Betalains?Documento1 páginaIgments IN Lants: Betalains: What Are Betalains?inka harrisAinda não há avaliações
- Inserto HPV IngDocumento48 páginasInserto HPV IngMelissa MenesesAinda não há avaliações
- Supplementary Materials for Human OTULIN haploinsufficiency impairs cell-intrinsic immunity to staphylococcal α-toxinDocumento47 páginasSupplementary Materials for Human OTULIN haploinsufficiency impairs cell-intrinsic immunity to staphylococcal α-toxinElif Tugce AydinAinda não há avaliações
- Cell Membrane Function and StructureDocumento6 páginasCell Membrane Function and Structurecris ibarraAinda não há avaliações
- Thesis StatementDocumento3 páginasThesis StatementMichelle Kate TorresAinda não há avaliações
- Cell DivisionDocumento17 páginasCell DivisionRaj AgrawalAinda não há avaliações
- Gene Therapy, Cell TherapyDocumento3 páginasGene Therapy, Cell TherapyMayuri DuttaAinda não há avaliações
- Project 1 Day 1Documento339 páginasProject 1 Day 1Mohamed NagyAinda não há avaliações
- Dna Computers Seminar ReportDocumento14 páginasDna Computers Seminar ReportSarika Sharma100% (2)
- Drugs Acting On The Blood and The BloodDocumento26 páginasDrugs Acting On The Blood and The BloodHealthy7Ainda não há avaliações
- Yeast Protocols.-springer-Verlag New York (2020)Documento259 páginasYeast Protocols.-springer-Verlag New York (2020)Andrés Nicolás Beltrán SeguraAinda não há avaliações
- Mubarek Aplied Neuroscience PPT Lecture NoteDocumento50 páginasMubarek Aplied Neuroscience PPT Lecture NoteAklile TsegaAinda não há avaliações
- AminofostineDocumento5 páginasAminofostinePedro JuarezAinda não há avaliações
- Redox Regulation, Thioredoxins, and Glutaredoxins (Review 2023)Documento15 páginasRedox Regulation, Thioredoxins, and Glutaredoxins (Review 2023)Hatem BoubakriAinda não há avaliações
- 4 - Transformasi GenetikDocumento42 páginas4 - Transformasi GenetikJatuna AyundaAinda não há avaliações
- Clinical EnzymologyDocumento23 páginasClinical EnzymologyKishore KaranAinda não há avaliações
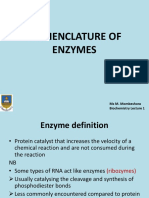
- Biochem 1 - NOMENCLATURE OF ENZYMESDocumento51 páginasBiochem 1 - NOMENCLATURE OF ENZYMESNyasha Peter ManamikeAinda não há avaliações
- Specialized Products From Amino Acids - Part 2Documento16 páginasSpecialized Products From Amino Acids - Part 2Leon WarrenAinda não há avaliações
- Thermochemistry Heteroatomic CompoundsDocumento7 páginasThermochemistry Heteroatomic CompoundsAnisatya AmaliahAinda não há avaliações
- Pharmaceutical Biochemistry Lecture No 1 General Introduction To Pharmacy and Pharmaceutical Biochemistry PharmacyDocumento2 páginasPharmaceutical Biochemistry Lecture No 1 General Introduction To Pharmacy and Pharmaceutical Biochemistry PharmacyAkash Syed100% (1)
- 20.320 Exam 2 Review Problem Solutions April 20, 2006 1. No InhibitionDocumento3 páginas20.320 Exam 2 Review Problem Solutions April 20, 2006 1. No InhibitionMovie Scene BankAinda não há avaliações
- ch26 Test 4Documento6 páginasch26 Test 4Cloris WongAinda não há avaliações
- Being Asked in Each of The Boxes. (Note: You Can Insert A Textbox Where You Can Insert Your Answer.)Documento4 páginasBeing Asked in Each of The Boxes. (Note: You Can Insert A Textbox Where You Can Insert Your Answer.)Reign PedrosaAinda não há avaliações
- HND Sector 2 Vol3-1Documento530 páginasHND Sector 2 Vol3-1mbabit leslieAinda não há avaliações