Você também pode gostar
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsAinda não há avaliações
- ICU Scoring Systems A Complete Guide - 2020 EditionNo EverandICU Scoring Systems A Complete Guide - 2020 EditionAinda não há avaliações
- Hypoglycemia PresentationDocumento45 páginasHypoglycemia Presentationask1400100% (1)
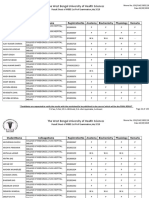
- The West Bengal University of Health SciencesDocumento9 páginasThe West Bengal University of Health Sciencesbhaskar rayAinda não há avaliações
- Neurologic Assessment RationaleDocumento16 páginasNeurologic Assessment RationaleflorenzoAinda não há avaliações
- Data Collection Form - Pressure InjuryDocumento3 páginasData Collection Form - Pressure InjuryErwin Dela GanaAinda não há avaliações
- Kidney TransplantDocumento11 páginasKidney TransplantPrincess Xzmae RamirezAinda não há avaliações
- Lab 9++10 Pathological UrinlysisDocumento38 páginasLab 9++10 Pathological UrinlysisSai SreedharAinda não há avaliações
- Routine Laboratory Evaluation of CoagulationDocumento7 páginasRoutine Laboratory Evaluation of CoagulationGilo IlaganAinda não há avaliações
- I.V. FluidsDocumento33 páginasI.V. FluidsVineel Bezawada100% (1)
- UTIDocumento17 páginasUTIBongkotchakorn Mind PhonchaiAinda não há avaliações
- Introduction To HematologyDocumento61 páginasIntroduction To HematologyThis is PonyAinda não há avaliações
- Physiology of DiabetesDocumento52 páginasPhysiology of DiabetesPhysiology by Dr RaghuveerAinda não há avaliações
- 041 - Endocrinology Physiology) Antidiuretic Hormone (ADH)Documento3 páginas041 - Endocrinology Physiology) Antidiuretic Hormone (ADH)یوسف رمضان100% (1)
- Gastric and Duodenal UlcerDocumento56 páginasGastric and Duodenal UlcerMatthew MckenzieAinda não há avaliações
- Cpap and Bipap: "A CPAP A Day Helps Keep The ET Tube Away!"Documento15 páginasCpap and Bipap: "A CPAP A Day Helps Keep The ET Tube Away!"Muhammad Tayyab MadniAinda não há avaliações
- Introduction To Clinical PathologyDocumento20 páginasIntroduction To Clinical PathologySwagath NAinda não há avaliações
- The Result of Any Laboratory Test Is Only As Good As The Sample Received in The LaboratoryDocumento16 páginasThe Result of Any Laboratory Test Is Only As Good As The Sample Received in The LaboratoryZeeshan YousufAinda não há avaliações
- Management of Arterial LineDocumento16 páginasManagement of Arterial LineFarcasanu Liana GeorgianaAinda não há avaliações
- Hemodialysis PPT School ProjectDocumento66 páginasHemodialysis PPT School ProjectBasharat KarimAinda não há avaliações
- Fluid Resuscitation and Organ Perfusion EvaluationDocumento66 páginasFluid Resuscitation and Organ Perfusion EvaluationDewiRatnasariAinda não há avaliações
- Theory UrinalysisDocumento23 páginasTheory UrinalysisAnggi Dyah AristiAinda não há avaliações
- Isotonic Saline (0.9%Nacl-Normal Saline) IndicationDocumento3 páginasIsotonic Saline (0.9%Nacl-Normal Saline) IndicationJared AllenAinda não há avaliações
- Diabetes MellitusDocumento110 páginasDiabetes MellitusToluwani Lade-ige100% (1)
- Preoperative EvaluationDocumento47 páginasPreoperative EvaluationCzerwin Juales100% (2)
- RenoVascular HypertensionDocumento34 páginasRenoVascular HypertensionAbira KhanAinda não há avaliações
- Point of Care TestingDocumento16 páginasPoint of Care TestingCookie MonsterAinda não há avaliações
- Report2014 PDFDocumento332 páginasReport2014 PDFShareDialysis100% (1)
- Lab InvestigationsDocumento25 páginasLab Investigationsbadar_aq100% (1)
- Metheny - Fluid and Electrolyte Balance 4th EdDocumento227 páginasMetheny - Fluid and Electrolyte Balance 4th Edfirst aid kit100% (1)
- Liver Function TestsDocumento16 páginasLiver Function TestsAnjali Devi100% (1)
- Approach To Septic ShockDocumento16 páginasApproach To Septic ShockRaja EllysyaAinda não há avaliações
- Massive Blood TransfusionDocumento17 páginasMassive Blood TransfusionevanAinda não há avaliações
- Interpretation of CBCDocumento35 páginasInterpretation of CBCnth1992Ainda não há avaliações
- Prospectus of Paramedical College in Delhi - IPHIDocumento16 páginasProspectus of Paramedical College in Delhi - IPHIParamedical CollegeinDelhiAinda não há avaliações
- Urine AnalysisDocumento53 páginasUrine AnalysisMaath KhalidAinda não há avaliações
- Diabetic Foot Case PresentationDocumento58 páginasDiabetic Foot Case PresentationZH. omg sarAinda não há avaliações
- UrinalysisDocumento32 páginasUrinalysiskholoud220Ainda não há avaliações
- SaO2 Versus SpO2Documento9 páginasSaO2 Versus SpO2jidongjc100% (1)
- Interpretation of Laboratory TestsDocumento21 páginasInterpretation of Laboratory TestsYadile D BenoitAinda não há avaliações
- Cardiac (Heart) FailureDocumento27 páginasCardiac (Heart) FailureSanthoshi Sadhanaa SankarAinda não há avaliações
- N A B H PDFDocumento92 páginasN A B H PDFtapan_tsgAinda não há avaliações
- Regional AnesthesiaDocumento54 páginasRegional AnesthesiaIdza Fariha AfriAinda não há avaliações
- Acidification of UrineDocumento30 páginasAcidification of UrineNanditha SureshAinda não há avaliações
- CPG Management of Dyslipidaemia 2017 (5th Edition)Documento107 páginasCPG Management of Dyslipidaemia 2017 (5th Edition)Ikram RauhiAinda não há avaliações
- Principles of Liver TransplantationDocumento22 páginasPrinciples of Liver TransplantationRajarshi KumarAinda não há avaliações
- Corrosive PoisoningDocumento4 páginasCorrosive PoisoningaBay AesculapianoAinda não há avaliações
- ICU One Pager EVD V11Documento1 páginaICU One Pager EVD V11Mohamed Mahmoud100% (1)
- Thromboembolic Disease PDFDocumento5 páginasThromboembolic Disease PDFBáĦẳá Y. Ẳl-mársǾúmiAinda não há avaliações
- Medical InvestigationsDocumento7 páginasMedical InvestigationsmedpgnotesAinda não há avaliações
- Pathology Bleeding DisordersDocumento67 páginasPathology Bleeding DisordersMarcelliaAinda não há avaliações
- Peripheral Smear ExaminationDocumento75 páginasPeripheral Smear ExaminationMoorthi100% (1)
- Febrile Neutropenia: Nontapak ThiangpakDocumento53 páginasFebrile Neutropenia: Nontapak ThiangpakRapid MedicineAinda não há avaliações
- Acute Gastroenteritis (AGE)Documento37 páginasAcute Gastroenteritis (AGE)Sari HariyaniAinda não há avaliações
- Medicine IMM SyllabusDocumento53 páginasMedicine IMM SyllabusAamir HamaadAinda não há avaliações
- Platelet ConcentratesDocumento2 páginasPlatelet ConcentratesARIF AHAMMEDAinda não há avaliações
- NKTI Lepto Handbook Second EditionDocumento40 páginasNKTI Lepto Handbook Second EditionJulie Ann BibalAinda não há avaliações
- Acid-Base Disorder 27 July 2017 PDFDocumento48 páginasAcid-Base Disorder 27 July 2017 PDFPauline ChanAinda não há avaliações
- Transportation and Stabilitation in Critically Ill Patient - 2015Documento36 páginasTransportation and Stabilitation in Critically Ill Patient - 2015Gustav Valentino100% (1)
- Fluid ManagementDocumento59 páginasFluid ManagementAj Primaditya WardhanaAinda não há avaliações
- Acetaminphen Overdose Treatment InfoDocumento19 páginasAcetaminphen Overdose Treatment InfoadadanAinda não há avaliações
- Hurst Review Services - Live Review ScheduleDocumento2 páginasHurst Review Services - Live Review Scheduleadadan100% (1)
- Crash Assessment For Field Triage: "Rules and Exceptions"Documento99 páginasCrash Assessment For Field Triage: "Rules and Exceptions"adadanAinda não há avaliações
- Acc 3121Documento8 páginasAcc 3121adadanAinda não há avaliações
- PublicHealthEmerging IssuesDocumento13 páginasPublicHealthEmerging IssuesadadanAinda não há avaliações
- Web QsenDocumento2 páginasWeb QsenadadanAinda não há avaliações
- Shaken Baby Syndrome (SBS)Documento18 páginasShaken Baby Syndrome (SBS)adadanAinda não há avaliações
- Nursing Report Sheet TemplateDocumento1 páginaNursing Report Sheet TemplateadadanAinda não há avaliações
- Clinical Pathway Acute Psych BehavioralDocumento3 páginasClinical Pathway Acute Psych Behavioraladadan100% (2)
- Exceptional Dentistry: Beverly Rose D.M.D.Documento1 páginaExceptional Dentistry: Beverly Rose D.M.D.adadanAinda não há avaliações
- HemorrhoidsDocumento2 páginasHemorrhoidsadadanAinda não há avaliações
- Na Clinical Skills ChecklistDocumento11 páginasNa Clinical Skills ChecklistadadanAinda não há avaliações
- The Postpartum Period and The Healthy Newborn: This Course Expires On November 30, 2015Documento30 páginasThe Postpartum Period and The Healthy Newborn: This Course Expires On November 30, 2015adadanAinda não há avaliações
- 36 36 Fr-CA 0 Phase II Trial of Encapsulated Ginger As A Treatment For Chemotherapy Induced Nausea and VomitingDocumento10 páginas36 36 Fr-CA 0 Phase II Trial of Encapsulated Ginger As A Treatment For Chemotherapy Induced Nausea and VomitingadadanAinda não há avaliações
- Connections: Nursing Practice ApplicationDocumento3 páginasConnections: Nursing Practice ApplicationadadanAinda não há avaliações
- Summary Clinical Skills TimingDocumento1 páginaSummary Clinical Skills TimingadadanAinda não há avaliações
- Calculation of Fluid Needs in SurgeryDocumento1 páginaCalculation of Fluid Needs in SurgeryadadanAinda não há avaliações
- Body Mass Index Percentiles For Boys and Girls From 5-17 YearsDocumento1 páginaBody Mass Index Percentiles For Boys and Girls From 5-17 YearsadadanAinda não há avaliações
- ICT ContactCenterServices 9 Q1 LAS3 FINALDocumento10 páginasICT ContactCenterServices 9 Q1 LAS3 FINALRomnia Grace DivinagraciaAinda não há avaliações
- 6 Adjective ClauseDocumento16 páginas6 Adjective ClauseMaharRkpAinda não há avaliações
- Ens TecDocumento28 páginasEns TecBorja CanalsAinda não há avaliações
- LIST OF REGISTERED DRUGS As of December 2012: DR No Generic Brand Strength Form CompanyDocumento2 páginasLIST OF REGISTERED DRUGS As of December 2012: DR No Generic Brand Strength Form CompanyBenjamin TantiansuAinda não há avaliações
- Diablo LED Wall LightDocumento2 páginasDiablo LED Wall LightSohit SachdevaAinda não há avaliações
- VSR 411 QB AnaesthesiaDocumento7 páginasVSR 411 QB Anaesthesiavishnu dathAinda não há avaliações
- 134.4902.06 - DM4170 - DatasheetDocumento7 páginas134.4902.06 - DM4170 - DatasheetVinicius MollAinda não há avaliações
- Variant Perception - Recessions and ShocksDocumento15 páginasVariant Perception - Recessions and ShocksVariant Perception Research80% (5)
- Cooking VocabularyDocumento2 páginasCooking VocabularyDANIELAAinda não há avaliações
- Radiesthesia and The Major ArcanaDocumento72 páginasRadiesthesia and The Major ArcanaStere Stere67% (3)
- Esomeprazol Vs RabeprazolDocumento7 páginasEsomeprazol Vs RabeprazolpabloAinda não há avaliações
- Questions To Client On SAP HCMDocumento19 páginasQuestions To Client On SAP HCMeurofighterAinda não há avaliações
- Pelatihan Olahan Pangan Ukm LamselDocumento6 páginasPelatihan Olahan Pangan Ukm LamselCalista manda WidyapalastriAinda não há avaliações
- Cardiovascular Pharmacology: DR Muhamad Ali Sheikh Abdul Kader MD (Usm) MRCP (Uk) Cardiologist, Penang HospitalDocumento63 páginasCardiovascular Pharmacology: DR Muhamad Ali Sheikh Abdul Kader MD (Usm) MRCP (Uk) Cardiologist, Penang HospitalCvt RasulAinda não há avaliações
- Antiarrhythmic DrugsDocumento56 páginasAntiarrhythmic DrugsHassan MohammadAinda não há avaliações
- LR-360KAS-BROCHURE-LNG Sampling SystemsDocumento4 páginasLR-360KAS-BROCHURE-LNG Sampling SystemsIdehen KelvinAinda não há avaliações
- Gpat Reference NotesDocumento9 páginasGpat Reference NotesPreethi KiranAinda não há avaliações
- PLAB 2 VISA Guidelines by Omar AlamDocumento18 páginasPLAB 2 VISA Guidelines by Omar Alamrafew19Ainda não há avaliações
- Business-Plan (John Lloyd A Perido Grade 12-Arc)Documento4 páginasBusiness-Plan (John Lloyd A Perido Grade 12-Arc)Jaypher PeridoAinda não há avaliações
- Service Manual - DM0412SDocumento11 páginasService Manual - DM0412SStefan Jovanovic100% (1)
- Stepanenko DermatologyDocumento556 páginasStepanenko DermatologySanskar DeyAinda não há avaliações
- Powermatic 58480438-Millrite-Mvn-Manual PDFDocumento54 páginasPowermatic 58480438-Millrite-Mvn-Manual PDFJason Willis75% (4)
- UNICEF Annual Report - Water 2018Documento20 páginasUNICEF Annual Report - Water 2018Ross WeistrofferAinda não há avaliações
- The List InditexDocumento126 páginasThe List InditexRezoanul Haque100% (2)
- Task 2: Health Services Survey: School Community 1. What Are The Health Services Provided?Documento1 páginaTask 2: Health Services Survey: School Community 1. What Are The Health Services Provided?Bernadeth BaiganAinda não há avaliações
- Soduim Prescription in The Prevention of Intradialytic HypotensionDocumento10 páginasSoduim Prescription in The Prevention of Intradialytic HypotensionTalala tililiAinda não há avaliações
- The Man Booker PrizeDocumento2 páginasThe Man Booker PrizeChu Hòa Bình100% (1)
- Public Health Interventions: Applications For Public Health Nursing PracticeDocumento249 páginasPublic Health Interventions: Applications For Public Health Nursing PracticeJemimah AdaclogAinda não há avaliações
- COLLOIDAL GOLD RECIPE - CitrateDocumento9 páginasCOLLOIDAL GOLD RECIPE - CitrateDevon Narok100% (4)
- The Ethics of CloningDocumento5 páginasThe Ethics of CloningUpai MbembAinda não há avaliações