Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- ATLS Post TestDocumento1 páginaATLS Post Testanon_57896987836% (56)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
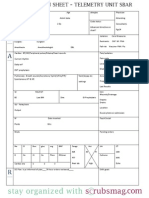
- Nurse Brain Sheet Telemetry Unit SBARDocumento1 páginaNurse Brain Sheet Telemetry Unit SBARvsosa624Ainda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Epidemiology Triangle of MalariaDocumento3 páginasEpidemiology Triangle of MalariaArslan Bashir100% (8)
- NCLEX Random FactsDocumento34 páginasNCLEX Random FactsLegnaMary100% (8)
- Drugs NclexDocumento30 páginasDrugs Nclexawuahboh100% (1)
- King Rush MoreDocumento1 páginaKing Rush MoreawuahbohAinda não há avaliações
- Article For JournalDocumento6 páginasArticle For JournalawuahbohAinda não há avaliações
- Oop Say You Know MeDocumento1 páginaOop Say You Know MeawuahbohAinda não há avaliações
- The BSN Job Search: Interview Preparation: Telling Your StoryDocumento25 páginasThe BSN Job Search: Interview Preparation: Telling Your StoryawuahbohAinda não há avaliações
- HandOff SampleToolsDocumento9 páginasHandOff SampleToolsOllie EvansAinda não há avaliações
- Massachusetts Department of Public HealthDocumento24 páginasMassachusetts Department of Public HealthawuahbohAinda não há avaliações
- Middle Age Adult Health History Assignment Guidelines N315 Fall 2013Documento23 páginasMiddle Age Adult Health History Assignment Guidelines N315 Fall 2013awuahbohAinda não há avaliações
- Pharm NclexDocumento9 páginasPharm NclexawuahbohAinda não há avaliações
- Article For CET CHFDocumento5 páginasArticle For CET CHFawuahbohAinda não há avaliações
- PolypharmacyDocumento24 páginasPolypharmacySurina Zaman HuriAinda não há avaliações
- Probability of A or B and A and B-1Documento2 páginasProbability of A or B and A and B-1awuahbohAinda não há avaliações
- EBP Article 1Documento11 páginasEBP Article 1awuahbohAinda não há avaliações
- Random FactsDocumento338 páginasRandom Factscyram81100% (1)
- STDA VaricealDocumento8 páginasSTDA VaricealDeisy de JesusAinda não há avaliações
- Therapeutic CommunicationDocumento1 páginaTherapeutic CommunicationawuahbohAinda não há avaliações
- EBP Article 3Documento6 páginasEBP Article 3awuahbohAinda não há avaliações
- Critical Thinking StrategiesDocumento3 páginasCritical Thinking StrategiesawuahbohAinda não há avaliações
- Tips On Answering NclexDocumento4 páginasTips On Answering NclexawuahbohAinda não há avaliações
- ENT Throat and EsophagusDocumento41 páginasENT Throat and EsophagusMUHAMMAD HASAN NAGRAAinda não há avaliações
- Debate 3 Youth Incarceration in Adult PrisonsDocumento6 páginasDebate 3 Youth Incarceration in Adult PrisonsawuahbohAinda não há avaliações
- Patient Report FormDocumento1 páginaPatient Report FormawuahbohAinda não há avaliações
- Does Prospective Payment Increase Hospital (In) Efficiency? Evidence From The Swiss Hospital SectorDocumento24 páginasDoes Prospective Payment Increase Hospital (In) Efficiency? Evidence From The Swiss Hospital SectorawuahbohAinda não há avaliações
- Article For CET CHFDocumento5 páginasArticle For CET CHFawuahbohAinda não há avaliações
- Article For JournalDocumento6 páginasArticle For JournalawuahbohAinda não há avaliações
- Article For Journal 4-18-14Documento8 páginasArticle For Journal 4-18-14awuahbohAinda não há avaliações
- Med Surg BurnsDocumento8 páginasMed Surg BurnsawuahbohAinda não há avaliações
- Article For Jouranal 2 (498P)Documento5 páginasArticle For Jouranal 2 (498P)awuahbohAinda não há avaliações
- Lecture - Maternal Health Concerns (Part 1)Documento1 páginaLecture - Maternal Health Concerns (Part 1)Rovilyn DizonAinda não há avaliações
- A03 - Sangita Singh - FPSC Naini 641A, Chak Raghunath, Mirzapur Road, ALLAHABAD, UP 211008Documento2 páginasA03 - Sangita Singh - FPSC Naini 641A, Chak Raghunath, Mirzapur Road, ALLAHABAD, UP 211008mohd arkamAinda não há avaliações
- Birla Institute of Technology & Science, Pilani Work Integrated Learning Programmes DigitalDocumento10 páginasBirla Institute of Technology & Science, Pilani Work Integrated Learning Programmes DigitalAAKAinda não há avaliações
- Pokemon 5th Edition - Gen I, II, & IIIDocumento265 páginasPokemon 5th Edition - Gen I, II, & IIIJames TonkinAinda não há avaliações
- Ethics Case StudyDocumento4 páginasEthics Case StudycasscactusAinda não há avaliações
- Title: Anthrax: Subtitles Are FollowingDocumento14 páginasTitle: Anthrax: Subtitles Are FollowingSyed ShahZaib ShahAinda não há avaliações
- How To Dominate The Ventilator: Spinning DialsDocumento5 páginasHow To Dominate The Ventilator: Spinning DialsIgnacia Cid PintoAinda não há avaliações
- ĐỀ THI THỬ 2021 - THPT QUẢNG XƯƠNG - THANH HOÁDocumento11 páginasĐỀ THI THỬ 2021 - THPT QUẢNG XƯƠNG - THANH HOÁNguyen NhanAinda não há avaliações
- Explant Sterilization TechniqueDocumento4 páginasExplant Sterilization TechniqueHaripriya88% (8)
- Motility and Fertility CorrelationDocumento14 páginasMotility and Fertility CorrelationvetlakshmiAinda não há avaliações
- Surgical DressingDocumento7 páginasSurgical DressingGabz GabbyAinda não há avaliações
- Criteria-Based Return To SprintingDocumento7 páginasCriteria-Based Return To SprintingJorge Aguirre GonzalezAinda não há avaliações
- Airway Publish Irfan AltafDocumento3 páginasAirway Publish Irfan AltafTAUSEEFA JANAinda não há avaliações
- Loads of Continuous Mechanics For Uprighting The Second Molar On The Second Molar and PremolarDocumento8 páginasLoads of Continuous Mechanics For Uprighting The Second Molar On The Second Molar and PremolarAlvaro ChacónAinda não há avaliações
- Goodman, Ashley SignedDocumento1 páginaGoodman, Ashley SignedAshley GoodmanAinda não há avaliações
- Ieltsfever Academic Reading Practcie Test 50 PDFDocumento11 páginasIeltsfever Academic Reading Practcie Test 50 PDFLOAinda não há avaliações
- Philadelphia Adventist ChurchDocumento2 páginasPhiladelphia Adventist ChurchMETALAinda não há avaliações
- Itm Dosage FormsDocumento15 páginasItm Dosage FormsArun Singh N JAinda não há avaliações
- Viva Q-Ans Class XiiDocumento10 páginasViva Q-Ans Class Xiipavani pavakiAinda não há avaliações
- Psychology Project CbseDocumento17 páginasPsychology Project CbseJiya GeorgeAinda não há avaliações
- The Power of ConflictDocumento4 páginasThe Power of Conflictapi-459276089Ainda não há avaliações
- Kel 3 A Midwifery Model of Care ForDocumento13 páginasKel 3 A Midwifery Model of Care ForWawa KurniaAinda não há avaliações
- Daily Lesson Log Week 2Documento7 páginasDaily Lesson Log Week 2Jolie Ann De GuzmanAinda não há avaliações
- Communicable Disease QuizDocumento2 páginasCommunicable Disease QuizPlacida Mequiabas National High SchoolAinda não há avaliações
- Resume Fall 2022 PDFDocumento2 páginasResume Fall 2022 PDFapi-663012445Ainda não há avaliações
- Master Summary of Parenting - I Read 16 Parenting Books To Create This Master SummaryDocumento16 páginasMaster Summary of Parenting - I Read 16 Parenting Books To Create This Master SummarySaurabh Jain CAAinda não há avaliações
- Testicular Cancer (Teratoma Testis)Documento7 páginasTesticular Cancer (Teratoma Testis)Witha Lestari AdethiaAinda não há avaliações
- Good Morning Class! February 10, 2021: Tle-CarpentryDocumento57 páginasGood Morning Class! February 10, 2021: Tle-CarpentryGlenn Fortades SalandananAinda não há avaliações