Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Vet CareplanexampleDocumento6 páginasVet CareplanexampleAnonymous eJZ5HcAinda não há avaliações
- Transformation of Modern Library in To Green Library For Sustaining FutureDocumento7 páginasTransformation of Modern Library in To Green Library For Sustaining FutureHardik AnandAinda não há avaliações
- E2788-11 Standard Specification For Use of Expanded Shale, Clay and Slate (ESCS) As A Mineral Component in The Growing Media and The Drainage Layer For Vegetative (Green) Roof SystemsDocumento3 páginasE2788-11 Standard Specification For Use of Expanded Shale, Clay and Slate (ESCS) As A Mineral Component in The Growing Media and The Drainage Layer For Vegetative (Green) Roof SystemsSatya kaliprasad vangaraAinda não há avaliações
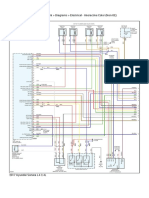
- 2017 Hyundai Sonata L4-2.4L Engine Controls (Powertrain Management) - ALLDATA RepairDocumento6 páginas2017 Hyundai Sonata L4-2.4L Engine Controls (Powertrain Management) - ALLDATA RepairChino PlagaAinda não há avaliações
- r315 Quick Start PDFDocumento80 páginasr315 Quick Start PDFfdsfasdsfadsAinda não há avaliações
- Kasuti of KarnatakaDocumento2 páginasKasuti of KarnatakarhlkAinda não há avaliações
- HSE Plan For RSPL ProjectDocumento10 páginasHSE Plan For RSPL ProjectSaibabu SiripurapuAinda não há avaliações
- Classification of Tooth StainingDocumento4 páginasClassification of Tooth StainingYAMUNA M.D.S. PAEDODONTICS & PREVENTIVE DENTISTRYAinda não há avaliações
- Water Treatment Lecture 4Documento34 páginasWater Treatment Lecture 4pramudita nadiahAinda não há avaliações
- Mikrotik Kung Fu Kitab 2Documento68 páginasMikrotik Kung Fu Kitab 2aditya ferdiansyahAinda não há avaliações
- Mice and Men Naturalism Web SiteDocumento10 páginasMice and Men Naturalism Web SitedrooolAinda não há avaliações
- E2870-13 Standard Test Method For Evaluating RelativDocumento6 páginasE2870-13 Standard Test Method For Evaluating RelativA MusaverAinda não há avaliações
- 6.m.tech-Ece-Vlsi, Vlsi Systems, Vlsi System Design (Vlsi, Vlsis, Vlsisd) r17 Course Structure & SyllabiDocumento35 páginas6.m.tech-Ece-Vlsi, Vlsi Systems, Vlsi System Design (Vlsi, Vlsis, Vlsisd) r17 Course Structure & SyllabiravibabukancharlaAinda não há avaliações
- 1-Theory of Metal Cutting PDFDocumento144 páginas1-Theory of Metal Cutting PDFNithinArvindAinda não há avaliações
- BMC IV - Module 02 Finishes 200912Documento56 páginasBMC IV - Module 02 Finishes 200912Fidha SulfiAinda não há avaliações
- NSO SPRDocumento9 páginasNSO SPRADITYA SINGHAinda não há avaliações
- Trucks Fin Eu PCDocumento117 páginasTrucks Fin Eu PCjeanpienaarAinda não há avaliações
- Energy and FluctuationDocumento10 páginasEnergy and Fluctuationwalid Ait MazouzAinda não há avaliações
- Norma ASTM C171Documento2 páginasNorma ASTM C171Jony Gutiérrez100% (1)
- Power System Analysis and Design EE-461: Tassawar Kazmi Lecturer, EE Department, Seecs, NustDocumento10 páginasPower System Analysis and Design EE-461: Tassawar Kazmi Lecturer, EE Department, Seecs, NustShahab SaqibAinda não há avaliações
- Labangon Elementary School Diagbostic Test in Epp/Tle 6 Directions: Multiple Choice. Choose The Correct The Letter of The Correct AnswerDocumento4 páginasLabangon Elementary School Diagbostic Test in Epp/Tle 6 Directions: Multiple Choice. Choose The Correct The Letter of The Correct AnswerJulianFlorenzFalconeAinda não há avaliações
- Examination Speaking Assignments Term III - 2021Documento2 páginasExamination Speaking Assignments Term III - 2021Khrystyna ShkilniukAinda não há avaliações
- Ufm Interpretation SynopsisDocumento1 páginaUfm Interpretation SynopsispipegamoAinda não há avaliações
- Ford6000cd Rear ConnectorDocumento2 páginasFord6000cd Rear ConnectorAnonymous WcYW9AeAinda não há avaliações
- 11 Physical Fitness Assessment 1Documento40 páginas11 Physical Fitness Assessment 1Danilo Sare IIIAinda não há avaliações
- 100% Chemical-Free Solution For Organic Farming: Where Health Is A HabitDocumento2 páginas100% Chemical-Free Solution For Organic Farming: Where Health Is A Habitamit4118Ainda não há avaliações
- NL0520 NEPAL SagarmathaDocumento12 páginasNL0520 NEPAL SagarmathaPrashantpal RaiAinda não há avaliações
- 1414-Electric Room 1 Calculation Report Rev.02Documento28 páginas1414-Electric Room 1 Calculation Report Rev.02zakariaelrayesusaAinda não há avaliações
- Glass Standards PDFDocumento4 páginasGlass Standards PDFCristian TofanAinda não há avaliações
- IBH Link UA Manual PDFDocumento302 páginasIBH Link UA Manual PDFjavixl1Ainda não há avaliações