Você também pode gostar
- Addison Disease: Diagnosis and Initial ManagementDocumento5 páginasAddison Disease: Diagnosis and Initial ManagementI Gede SubagiaAinda não há avaliações
- Adrenal InsufficiencyDocumento11 páginasAdrenal InsufficiencyAustine OsaweAinda não há avaliações
- Jurnal Krisis AdrenalDocumento4 páginasJurnal Krisis AdrenalMelda IndrawatiAinda não há avaliações
- Causes of Diffuse Hyperpigmentation EndocrinopathiesDocumento9 páginasCauses of Diffuse Hyperpigmentation EndocrinopathiesAbdul QuyyumAinda não há avaliações
- MRCPass Notes For MRCP 1 - EnDOCRINOLOGYDocumento12 páginasMRCPass Notes For MRCP 1 - EnDOCRINOLOGYsabdali100% (1)
- Your Online Nursing Notes : Addison'S Disease Basic InfoDocumento4 páginasYour Online Nursing Notes : Addison'S Disease Basic InfoseigelysticAinda não há avaliações
- Addison's DseDocumento9 páginasAddison's DseKath RubioAinda não há avaliações
- Adrenocortical DisordersDocumento73 páginasAdrenocortical DisordersReunita ConstantiaAinda não há avaliações
- Adrenal Insufficiency: DR - Abbas Mansour Senior Consultant Internal MedicineDocumento24 páginasAdrenal Insufficiency: DR - Abbas Mansour Senior Consultant Internal Medicineraed faisalAinda não há avaliações
- Adrenal Diseases: Types Aetiology Diagnosis Complications TreatmentDocumento29 páginasAdrenal Diseases: Types Aetiology Diagnosis Complications Treatmentgani7222Ainda não há avaliações
- Wernicke Encephalopathy: EtiologyDocumento6 páginasWernicke Encephalopathy: EtiologyDrhikmatullah SheraniAinda não há avaliações
- Adrenal Gland DisordersDocumento31 páginasAdrenal Gland DisordersThe AbyssinicansAinda não há avaliações
- Insuficiencia AdrenalDocumento5 páginasInsuficiencia AdrenalLuciana RafaelAinda não há avaliações
- Endocrinology NotesDocumento12 páginasEndocrinology Notesrandiey john abelleraAinda não há avaliações
- Adrenal Gland: Adrenal Insufficiency, Addison Disease, Cushing SyndromeDocumento46 páginasAdrenal Gland: Adrenal Insufficiency, Addison Disease, Cushing Syndromeyuyu tuptupAinda não há avaliações
- Addisons DiseaseDocumento12 páginasAddisons DiseaseChinju CyrilAinda não há avaliações
- AddisonsdiseaseDocumento5 páginasAddisonsdiseasenessimmounir1173Ainda não há avaliações
- 6 Mary Lou Sole, Deborah Goldenberg Klein, Marthe J. Moseley - EndokrinDocumento56 páginas6 Mary Lou Sole, Deborah Goldenberg Klein, Marthe J. Moseley - EndokrinyaminmuhAinda não há avaliações
- Thyroid Disorder NCPDocumento9 páginasThyroid Disorder NCPKen RegalaAinda não há avaliações
- Adrenal Crisis: Risk FactorsDocumento25 páginasAdrenal Crisis: Risk Factorspwinzizitah063Ainda não há avaliações
- Adrenal Insufficiency in The Intensive Care Unit: Samir El Ansary Icu Professor Ain Shams CairoDocumento49 páginasAdrenal Insufficiency in The Intensive Care Unit: Samir El Ansary Icu Professor Ain Shams CairoGebby MamuayaAinda não há avaliações
- Adrenal CrisisDocumento4 páginasAdrenal CrisisRichie Marie BajaAinda não há avaliações
- Cushings, Addisons and Acromegaly: DR J Storrow FY2Documento38 páginasCushings, Addisons and Acromegaly: DR J Storrow FY2abdalkhalidAinda não há avaliações
- ENDO - Adrenal CrisisDocumento8 páginasENDO - Adrenal CrisisHajime NakaegawaAinda não há avaliações
- Tanpa JudulDocumento14 páginasTanpa JudulAsrapia HubaisyingAinda não há avaliações
- Endocrinology Course Content: Semester (5) Clinical Pharmacy CourseDocumento91 páginasEndocrinology Course Content: Semester (5) Clinical Pharmacy CourseSadigMukhAinda não há avaliações
- Subclinical Hyperthyroidism Case ReportDocumento26 páginasSubclinical Hyperthyroidism Case ReportkapanjddokterAinda não há avaliações
- 22 MetabolicEncephalopathies FinalDocumento19 páginas22 MetabolicEncephalopathies FinalShravan BimanapalliAinda não há avaliações
- Autoimmune Polyglandular Syndrome ReviewDocumento3 páginasAutoimmune Polyglandular Syndrome ReviewIan AlvaradoAinda não há avaliações
- Adrenal Crisis FinalDocumento10 páginasAdrenal Crisis FinalAmanda Scarlet100% (1)
- REPORTDocumento13 páginasREPORTEarlou MagbanuaAinda não há avaliações
- Addison's DiseaseDocumento3 páginasAddison's Diseaseavinash dhameriyaAinda não há avaliações
- Endocrinology Teaching CasesDocumento47 páginasEndocrinology Teaching CasesBinta BaptisteAinda não há avaliações
- EndokrinDocumento27 páginasEndokrinSarah Putri AbellysaAinda não há avaliações
- Canine Hypoadrenocorticism Overvew Diagnosis and Treatment LolattiDocumento6 páginasCanine Hypoadrenocorticism Overvew Diagnosis and Treatment LolattiAna Clara SevasteAinda não há avaliações
- 20 Endocrine Disease and AnaesthesiaDocumento0 página20 Endocrine Disease and AnaesthesiajuniorebindaAinda não há avaliações
- 2 Bvab048.1976Documento1 página2 Bvab048.1976Anca LunguAinda não há avaliações
- Case Study: MYXEDEMATOUS COMADocumento5 páginasCase Study: MYXEDEMATOUS COMAjisooAinda não há avaliações
- Adrenal Senior 1Documento12 páginasAdrenal Senior 1mohammad saifuddinAinda não há avaliações
- Stunted Growth: Addison DiseaseDocumento32 páginasStunted Growth: Addison DiseaseAshim AbhiAinda não há avaliações
- ENDOCRINE DISORDERS (Autosaved)Documento81 páginasENDOCRINE DISORDERS (Autosaved)Princewill SeiyefaAinda não há avaliações
- Adrenal and Pitutary Disoreders Adigrat LecDocumento144 páginasAdrenal and Pitutary Disoreders Adigrat Lecbereket gashuAinda não há avaliações
- Addison's Disease:: Clinical IntelligenceDocumento3 páginasAddison's Disease:: Clinical Intelligencemira tianiAinda não há avaliações
- Adrenal InsufficiencyDocumento2 páginasAdrenal InsufficiencyTracy NwanneAinda não há avaliações
- Flashcards - QuizletDocumento7 páginasFlashcards - QuizletNEsreAinda não há avaliações
- Addison DiseaseDocumento23 páginasAddison DiseaseKompari EvansAinda não há avaliações
- Pituitary &thyroid NotesDocumento7 páginasPituitary &thyroid NotesAli salimAinda não há avaliações
- Addison's DiseaseDocumento15 páginasAddison's DiseaseRonald A. Ogania50% (4)
- NCMB316 Rle 2-10-7addison's DiseaseDocumento4 páginasNCMB316 Rle 2-10-7addison's DiseaseMaica LectanaAinda não há avaliações
- Parathyroid DisordersDocumento44 páginasParathyroid DisordersBIAN ALKHAZMARIAinda não há avaliações
- Research Paper On Addisons DiseaseDocumento8 páginasResearch Paper On Addisons Diseasetug0l0byh1g2100% (1)
- Geriatric Anesthesia & Analgesia: ComplicationsDocumento4 páginasGeriatric Anesthesia & Analgesia: ComplicationsWilly Victorio CisnerosAinda não há avaliações
- adrenal presentation - صیادیDocumento39 páginasadrenal presentation - صیادیRazyAinda não há avaliações
- Summary of Medical EmergenciesDocumento24 páginasSummary of Medical Emergenciesbasharswork99Ainda não há avaliações
- Addisonian Crisis: Manish K Medical Officer IgmhDocumento47 páginasAddisonian Crisis: Manish K Medical Officer IgmhNaaz Delhiwale100% (1)
- Reye'S Syndrome: Mrs. Smitha.M Associate Professor Vijaya College of Nursing KottarakkaraDocumento7 páginasReye'S Syndrome: Mrs. Smitha.M Associate Professor Vijaya College of Nursing KottarakkarakrishnasreeAinda não há avaliações
- Endocrine DiseasesDocumento64 páginasEndocrine DiseasesshobanaaaradhanaAinda não há avaliações
- Thyrotoxicosis Ischaemic Heart Disease Hypertension Alcohol Excess Lone Atrial FibrillationDocumento5 páginasThyrotoxicosis Ischaemic Heart Disease Hypertension Alcohol Excess Lone Atrial FibrillationZhao Xuan TanAinda não há avaliações
- 351 UN 1824 Sodium Hydroxide SolutionDocumento8 páginas351 UN 1824 Sodium Hydroxide SolutionCharls DeimoyAinda não há avaliações
- Celltac MEK 6500Documento3 páginasCelltac MEK 6500RiduanAinda não há avaliações
- Presentasi Evaluasi Manajemen Risiko - YLYDocumento16 páginasPresentasi Evaluasi Manajemen Risiko - YLYOPERASIONALAinda não há avaliações
- Withania DSC PDFDocumento6 páginasWithania DSC PDFEfsha KhanAinda não há avaliações
- Qualitative Tests Organic NotesDocumento5 páginasQualitative Tests Organic NotesAdorned. pearlAinda não há avaliações
- Ams - 4640-C63000 Aluminium Nickel MNDocumento3 páginasAms - 4640-C63000 Aluminium Nickel MNOrnella MancinelliAinda não há avaliações
- Sociology/Marriage PresentationDocumento31 páginasSociology/Marriage PresentationDoofSadAinda não há avaliações
- PMEGP Revised Projects (Mfg. & Service) Vol 1Documento260 páginasPMEGP Revised Projects (Mfg. & Service) Vol 1Santosh BasnetAinda não há avaliações
- (ISPS Book Series) Yrjö O. Alanen, Manuel González de Chávez, Ann-Louise S. Silver, Brian Martindale - Psychotherapeutic Approaches To Schizophrenic Psychoses - Past, Present and Future-Routledge (20Documento419 páginas(ISPS Book Series) Yrjö O. Alanen, Manuel González de Chávez, Ann-Louise S. Silver, Brian Martindale - Psychotherapeutic Approaches To Schizophrenic Psychoses - Past, Present and Future-Routledge (20Manuel100% (1)
- Women and International Human Rights Law PDFDocumento67 páginasWomen and International Human Rights Law PDFakilasriAinda não há avaliações
- GeoSS Event Seminar 12 July 2012 - SlidesDocumento15 páginasGeoSS Event Seminar 12 July 2012 - SlidesNurmanda RamadhaniAinda não há avaliações
- 2008 03 20 BDocumento8 páginas2008 03 20 BSouthern Maryland OnlineAinda não há avaliações
- Additional Activity 3 InsciDocumento3 páginasAdditional Activity 3 InsciZophia Bianca BaguioAinda não há avaliações
- Shoulder Joint Position Sense Improves With ElevationDocumento10 páginasShoulder Joint Position Sense Improves With ElevationpredragbozicAinda não há avaliações
- HDFC Life Insurance (HDFCLIFE) : 2. P/E 58 3. Book Value (RS) 23.57Documento5 páginasHDFC Life Insurance (HDFCLIFE) : 2. P/E 58 3. Book Value (RS) 23.57Srini VasanAinda não há avaliações
- Defects Lamellar TearingDocumento6 páginasDefects Lamellar Tearingguru_terexAinda não há avaliações
- Cataloge ICARDocumento66 páginasCataloge ICARAgoess Oetomo100% (1)
- Vocab PDFDocumento29 páginasVocab PDFShahab SaqibAinda não há avaliações
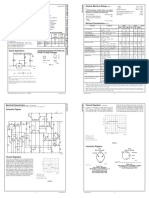
- LM 337Documento4 páginasLM 337matias robertAinda não há avaliações
- NASA ISS Expedition 2 Press KitDocumento27 páginasNASA ISS Expedition 2 Press KitOrion2015Ainda não há avaliações
- Ethnomedicinal Plants For Indigestion in Uthiramerur Taluk Kancheepuram District Tamilnadu IndiaDocumento8 páginasEthnomedicinal Plants For Indigestion in Uthiramerur Taluk Kancheepuram District Tamilnadu IndiaGladys DjeugaAinda não há avaliações
- Pescatarian Mediterranean Diet Cookbook 2 - Adele TylerDocumento98 páginasPescatarian Mediterranean Diet Cookbook 2 - Adele Tylerrabino_rojoAinda não há avaliações
- Allison Weech Final ResumeDocumento1 páginaAllison Weech Final Resumeapi-506177291Ainda não há avaliações
- Indirect Current Control of LCL Based Shunt Active Power FilterDocumento10 páginasIndirect Current Control of LCL Based Shunt Active Power FilterArsham5033Ainda não há avaliações
- Cisco - Level 45Documento1 páginaCisco - Level 45vithash shanAinda não há avaliações
- Leave of Absence Form (Rev. 02 072017)Documento1 páginaLeave of Absence Form (Rev. 02 072017)KIMBERLY BALISACANAinda não há avaliações
- Material: Safety Data SheetDocumento3 páginasMaterial: Safety Data SheetMichael JoudalAinda não há avaliações
- 1 Stra Bill FinalDocumento41 páginas1 Stra Bill FinalRajesh JhaAinda não há avaliações
- R. Nishanth K. VigneswaranDocumento20 páginasR. Nishanth K. VigneswaranAbishaTeslinAinda não há avaliações
- Ergo 1 - Workshop 3Documento3 páginasErgo 1 - Workshop 3Mugar GeillaAinda não há avaliações