Você também pode gostar
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Morse Potential CurveDocumento9 páginasMorse Potential Curvejagabandhu_patraAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Internet Bill FormatDocumento1 páginaInternet Bill FormatGopal Singh100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Tachycardia Algorithm 2021Documento1 páginaTachycardia Algorithm 2021Ravin DebieAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Estate TaxDocumento10 páginasEstate TaxCharrie Grace PabloAinda não há avaliações
- Assignment 3Documento2 páginasAssignment 3Debopam RayAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Paramount Healthcare Management Private Limited: First Reminder Letter Without PrejudiceDocumento1 páginaParamount Healthcare Management Private Limited: First Reminder Letter Without PrejudiceSwapnil TiwariAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Ideal Gas Law Lesson Plan FinalDocumento5 páginasIdeal Gas Law Lesson Plan FinalLonel SisonAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Mark Magazine#65Documento196 páginasMark Magazine#65AndrewKanischevAinda não há avaliações
- Villamaria JR Vs CADocumento2 páginasVillamaria JR Vs CAClarissa SawaliAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
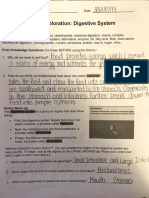
- Student Exploration: Digestive System: Food Inio Simple Nutrien/oDocumento9 páginasStudent Exploration: Digestive System: Food Inio Simple Nutrien/oAshantiAinda não há avaliações
- IPM GuidelinesDocumento6 páginasIPM GuidelinesHittesh SolankiAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Ac221 and Ac211 CourseoutlineDocumento10 páginasAc221 and Ac211 CourseoutlineLouis Maps MapangaAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- A SURVEY OF ENVIRONMENTAL REQUIREMENTS FOR THE MIDGE (Diptera: Tendipedidae)Documento15 páginasA SURVEY OF ENVIRONMENTAL REQUIREMENTS FOR THE MIDGE (Diptera: Tendipedidae)Batuhan ElçinAinda não há avaliações
- LG Sigma+EscalatorDocumento4 páginasLG Sigma+Escalator강민호Ainda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Research On Export Trade in BangladeshDocumento7 páginasResearch On Export Trade in BangladeshFarjana AnwarAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Christena Nippert-Eng - Watching Closely - A Guide To Ethnographic Observation-Oxford University Press (2015)Documento293 páginasChristena Nippert-Eng - Watching Closely - A Guide To Ethnographic Observation-Oxford University Press (2015)Emiliano CalabazaAinda não há avaliações
- Life in The Ancient WorldDocumento48 páginasLife in The Ancient Worldjmagil6092100% (1)
- Personal Finance Kapoor 11th Edition Solutions ManualDocumento26 páginasPersonal Finance Kapoor 11th Edition Solutions Manualsiennamurielhlhk100% (28)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Journal of Atmospheric Science Research - Vol.5, Iss.4 October 2022Documento54 páginasJournal of Atmospheric Science Research - Vol.5, Iss.4 October 2022Bilingual PublishingAinda não há avaliações
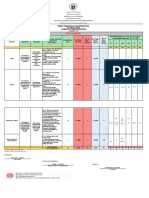
- Revised Final Quarter 1 Tos-Rbt-Sy-2022-2023 Tle-Cookery 10Documento6 páginasRevised Final Quarter 1 Tos-Rbt-Sy-2022-2023 Tle-Cookery 10May Ann GuintoAinda não há avaliações
- Rubric For Aet570 BenchmarkDocumento4 páginasRubric For Aet570 Benchmarkapi-255765082Ainda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- 100 20210811 ICOPH 2021 Abstract BookDocumento186 páginas100 20210811 ICOPH 2021 Abstract Bookwafiq alibabaAinda não há avaliações
- Hydrogeological Survey and Eia Tor - Karuri BoreholeDocumento3 páginasHydrogeological Survey and Eia Tor - Karuri BoreholeMutonga Kitheko100% (1)
- HemoptysisDocumento30 páginasHemoptysisMarshall ThompsonAinda não há avaliações
- NHM Thane Recruitment 2022 For 280 PostsDocumento9 páginasNHM Thane Recruitment 2022 For 280 PostsDr.kailas Gaikwad , MO UPHC Turbhe NMMCAinda não há avaliações
- DIFFERENTIATING PERFORMANCE TASK FOR DIVERSE LEARNERS (Script)Documento2 páginasDIFFERENTIATING PERFORMANCE TASK FOR DIVERSE LEARNERS (Script)Laurice Carmel AgsoyAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Grade 9 WorkbookDocumento44 páginasGrade 9 WorkbookMaria Russeneth Joy NaloAinda não há avaliações
- Product Specifications Product Specifications: LLPX411F LLPX411F - 00 - V1 V1Documento4 páginasProduct Specifications Product Specifications: LLPX411F LLPX411F - 00 - V1 V1David MooneyAinda não há avaliações
- Object-Oriented Design Patterns in The Kernel, Part 2 (LWN - Net)Documento15 páginasObject-Oriented Design Patterns in The Kernel, Part 2 (LWN - Net)Rishabh MalikAinda não há avaliações
- ThaneDocumento2 páginasThaneAkansha KhaitanAinda não há avaliações