Você também pode gostar
- 20 Pathoma Skin DisordersDocumento10 páginas20 Pathoma Skin Disordersn alawiAinda não há avaliações
- Introduction to Oncology: Retroviruses, Oncogenes, and Cancer DevelopmentDocumento22 páginasIntroduction to Oncology: Retroviruses, Oncogenes, and Cancer DevelopmentkurniawanAinda não há avaliações
- 2011-07-PATHO-Basic Pathology of SkinDocumento17 páginas2011-07-PATHO-Basic Pathology of SkindtimtimanAinda não há avaliações
- Chromosomal Abnormalities Provide Insights into Cancer GeneticsDocumento48 páginasChromosomal Abnormalities Provide Insights into Cancer GeneticsDr.Santosh KumarAinda não há avaliações
- Subfalcine Herniation Damages Cingulate GyrusDocumento34 páginasSubfalcine Herniation Damages Cingulate GyrusLorenzo FrancisAinda não há avaliações
- Psycho Sexual 6ceu CourseDocumento78 páginasPsycho Sexual 6ceu CourseariizianaAinda não há avaliações
- Oral Dermatology: Important Oral Questions & AnswersDocumento29 páginasOral Dermatology: Important Oral Questions & AnswersMedo JTAinda não há avaliações
- Causes and Treatment of Malignant Melanoma: DiscussionDocumento4 páginasCauses and Treatment of Malignant Melanoma: DiscussionAriSeliengAinda não há avaliações
- Clinical Pearls DermatologíamatologyDocumento4 páginasClinical Pearls DermatologíamatologyMaritza24Ainda não há avaliações
- Dermatology Lectures JRRMMCDocumento10 páginasDermatology Lectures JRRMMCGi Em100% (1)
- Obama Mind ControlDocumento68 páginasObama Mind Controlkdnkgljfg67% (3)
- Dr F Bhatti's Guide to Skin Tumours and CancersDocumento39 páginasDr F Bhatti's Guide to Skin Tumours and CancerspfxbkAinda não há avaliações
- Introductory Pharmacology - Cancer ChemotherapyDocumento9 páginasIntroductory Pharmacology - Cancer ChemotherapyTyler Rosolowski100% (2)
- Review of Dermatology Ebook Ebook Alikhan, Ali, Hocker, Thomas L. H Kindle StoreDocumento1 páginaReview of Dermatology Ebook Ebook Alikhan, Ali, Hocker, Thomas L. H Kindle StoreSally dossAinda não há avaliações
- Rational Antibiotic Usage and Antibiotic Policy - Dr. FirmansyahDocumento76 páginasRational Antibiotic Usage and Antibiotic Policy - Dr. Firmansyahjay neefAinda não há avaliações
- Question 1 of 13 on pityriasis rosea diagnosisDocumento23 páginasQuestion 1 of 13 on pityriasis rosea diagnosisjonyAinda não há avaliações
- Lesson Plan in English 8 Q2 Module 1Documento8 páginasLesson Plan in English 8 Q2 Module 1Nicky SanchezAinda não há avaliações
- Merkel Cell CarcinomaDocumento15 páginasMerkel Cell CarcinomaJhonnathan Rodriguez100% (1)
- History Taking in JaundiceDocumento2 páginasHistory Taking in Jaundiceshanyiar100% (5)
- MELANOMA: Risk Factors, Diagnosis, Staging and TreatmentDocumento25 páginasMELANOMA: Risk Factors, Diagnosis, Staging and TreatmentFazaKhilwanAmnaAinda não há avaliações
- Cell Cycle ChemotherapyDocumento5 páginasCell Cycle ChemotherapyVictoria Alessandra BrownAinda não há avaliações
- Review Article Immunotherapy in The Treatment of Metastatic Melanoma: Current Knowledge and Future DirectionsDocumento16 páginasReview Article Immunotherapy in The Treatment of Metastatic Melanoma: Current Knowledge and Future DirectionsSeprianto RuslanAinda não há avaliações
- Overview of CancerDocumento31 páginasOverview of Cancersamarth kaulAinda não há avaliações
- Review Mechanisms of Caspase Activation and Inhibition During ApoptosisDocumento12 páginasReview Mechanisms of Caspase Activation and Inhibition During ApoptosisFery WirawanAinda não há avaliações
- The Biology of Apoptosis: Fouad Boulos, MD August 2010Documento4 páginasThe Biology of Apoptosis: Fouad Boulos, MD August 2010ans11Ainda não há avaliações
- Concurrent ChemoRadiotherapyDocumento51 páginasConcurrent ChemoRadiotherapyJalal EltabibAinda não há avaliações
- Multiple MyelomaDocumento17 páginasMultiple MyelomaAhmed AbouelwafaAinda não há avaliações
- Adjuvant breast cancer therapy agentsDocumento3 páginasAdjuvant breast cancer therapy agentsGem BulaongAinda não há avaliações
- Cancer ChemotherapyDocumento86 páginasCancer ChemotherapyFrancheska MicuAinda não há avaliações
- BIO 2 MergedDocumento132 páginasBIO 2 Mergedsubham ghoshAinda não há avaliações
- Oncology Questions by DR - OkashaDocumento31 páginasOncology Questions by DR - Okashamohammed okashaAinda não há avaliações
- ABT-199, A Potent and Selective BCL-2 Inhibitor, Achieves Antitumor Activity While Sparing PlateletsDocumento9 páginasABT-199, A Potent and Selective BCL-2 Inhibitor, Achieves Antitumor Activity While Sparing PlateletsSanziana CristeaAinda não há avaliações
- Crispr TechniqueDocumento16 páginasCrispr TechniqueAmmar Abbas100% (1)
- Skin Cancer in HKDocumento6 páginasSkin Cancer in HKChiu ChunAinda não há avaliações
- Apoptosis and CaspasesDocumento19 páginasApoptosis and CaspasesKunhutty Vasudevan AnubhamaAinda não há avaliações
- Maternal and Child PreboardDocumento17 páginasMaternal and Child PreboardMichelle GambolAinda não há avaliações
- Summary of Diseases Exam 1Documento9 páginasSummary of Diseases Exam 1smn416Ainda não há avaliações
- Anatomy and Pathology of Testicular Tumors - UpToDateDocumento26 páginasAnatomy and Pathology of Testicular Tumors - UpToDateBhargav YagnikAinda não há avaliações
- Molecular Carcinogenesis Endometrium PDFDocumento7 páginasMolecular Carcinogenesis Endometrium PDFMelati HasnailAinda não há avaliações
- Malignant Melanoma Research PaperDocumento10 páginasMalignant Melanoma Research Paperapi-272931142Ainda não há avaliações
- Diagnosis and Treatment of MelanomaDocumento14 páginasDiagnosis and Treatment of MelanomaAnonymous Af24L7Ainda não há avaliações
- Drug Toxicity in Pregnancy and LactationDocumento3 páginasDrug Toxicity in Pregnancy and LactationPardeep SonyAinda não há avaliações
- Drugs in LactationDocumento36 páginasDrugs in Lactationcorzpun168678100% (1)
- Drug Use During Pregnancy and LactationDocumento45 páginasDrug Use During Pregnancy and LactationSayli GoreAinda não há avaliações
- Advances in Malignant Melanoma - Clinical and Research PerspectivesDocumento264 páginasAdvances in Malignant Melanoma - Clinical and Research PerspectivesInternational Medical PublisherAinda não há avaliações
- NemaoDocumento94 páginasNemaoRoxenette Gil Bernales PangilinanAinda não há avaliações
- Guidelines For The Management of Nappy RashDocumento13 páginasGuidelines For The Management of Nappy RashOva PradiptaAinda não há avaliações
- MEN1 PPDocumento15 páginasMEN1 PPAaron D. PhoenixAinda não há avaliações
- Bookshelf NBK481860Documento192 páginasBookshelf NBK481860kukyAinda não há avaliações
- Principles of Diuretic Therapy: Dr. Rania Magadmi, MBBS, PHDDocumento24 páginasPrinciples of Diuretic Therapy: Dr. Rania Magadmi, MBBS, PHDمشاعرمبعثرةAinda não há avaliações
- Protozoan Parasites Causing Malaria, Sleeping Sickness, Leishmaniasis and MoreDocumento32 páginasProtozoan Parasites Causing Malaria, Sleeping Sickness, Leishmaniasis and MoreFort SalvadorAinda não há avaliações
- Tissue Engineering SummaryDocumento28 páginasTissue Engineering SummaryDwisetyaSafirnaWidyaratihAinda não há avaliações
- NEUROPATHOLOGY REPORTDocumento28 páginasNEUROPATHOLOGY REPORTAnggi WahyuAinda não há avaliações
- Nematode Infections 2019 Student PDFDocumento272 páginasNematode Infections 2019 Student PDFCharlene SuliganAinda não há avaliações
- Microb Seminar Group 3 (LATEST)Documento21 páginasMicrob Seminar Group 3 (LATEST)HasifAinda não há avaliações
- Histamine 5-ht Angiotensin Kinin Endothelins Eicosanoids Interleukins TNF Interferones Growth FCDocumento57 páginasHistamine 5-ht Angiotensin Kinin Endothelins Eicosanoids Interleukins TNF Interferones Growth FCFaisal 'arifAinda não há avaliações
- Germ Cell TumoursDocumento32 páginasGerm Cell Tumoursapi-3705046Ainda não há avaliações
- Tumor Necrosis FactorDocumento77 páginasTumor Necrosis FactorRahul SinghAinda não há avaliações
- Medicine2 - Complications of Cancer Treatment 2007Documento76 páginasMedicine2 - Complications of Cancer Treatment 2007api-3762917Ainda não há avaliações
- Multidrug Resistance EssayDocumento15 páginasMultidrug Resistance EssayShainaz Mahmood Shams AddeenAinda não há avaliações
- EAU ESUR ESTRO SIOG Guidelines On Prostate Cancer Large Text V2Documento145 páginasEAU ESUR ESTRO SIOG Guidelines On Prostate Cancer Large Text V2DellaAinda não há avaliações
- Systemic Lupus Erythematosus Lecture Salah Abdel BakyDocumento8 páginasSystemic Lupus Erythematosus Lecture Salah Abdel Bakyahmed gabrAinda não há avaliações
- Receptors: Types Structure FunctionsDocumento44 páginasReceptors: Types Structure Functionsmaham1085Ainda não há avaliações
- Technology in Practical Dermatology: Non-Invasive Imaging, Lasers and Ulcer ManagementNo EverandTechnology in Practical Dermatology: Non-Invasive Imaging, Lasers and Ulcer ManagementMichele FimianiAinda não há avaliações
- Ray Model of LightDocumento2 páginasRay Model of LightMatthew NgAinda não há avaliações
- Human Digestive System Sls WorksheetDocumento2 páginasHuman Digestive System Sls WorksheetMatthew NgAinda não há avaliações
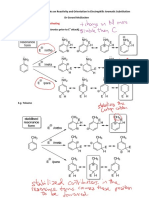
- The Effect of Substituents on Reactivity and Orientation in EASDocumento5 páginasThe Effect of Substituents on Reactivity and Orientation in EASMatthew Ng100% (1)
- Identification of Lactate Dehydrogenase Isoenzymes by Rapid KineticsDocumento5 páginasIdentification of Lactate Dehydrogenase Isoenzymes by Rapid KineticsMatthew NgAinda não há avaliações
- Born Is The Light of The WorldDocumento1 páginaBorn Is The Light of The WorldMatthew NgAinda não há avaliações
- A Positive Screen For Cloning PCR ProductsDocumento2 páginasA Positive Screen For Cloning PCR ProductsMatthew NgAinda não há avaliações
- FCPS Ii Major Tentative Schedule 2a Feb 2024Documento1 páginaFCPS Ii Major Tentative Schedule 2a Feb 2024haseeb ur rehmanAinda não há avaliações
- EMQ and SAQ Revision QuestionsDocumento12 páginasEMQ and SAQ Revision QuestionsSanathRaoAinda não há avaliações
- Closing The Gap 2012Documento127 páginasClosing The Gap 2012ABC News OnlineAinda não há avaliações
- Jan Marc Bulatao 10-Einstein BiologyDocumento3 páginasJan Marc Bulatao 10-Einstein BiologyNomer SenadorAinda não há avaliações
- CLASS 1 - Image - Roles Revised June 260Documento48 páginasCLASS 1 - Image - Roles Revised June 260Marie-Lynne L'orAinda não há avaliações
- ICU protocol 2015 قصر العيني by mansdocsDocumento227 páginasICU protocol 2015 قصر العيني by mansdocsWalaa YousefAinda não há avaliações
- MRI Monitoring System Provides Safety and MobilityDocumento4 páginasMRI Monitoring System Provides Safety and MobilityAchiyat WinataAinda não há avaliações
- Supine Cervical Traction After Anterior Cervical Diskectomy and FusionDocumento4 páginasSupine Cervical Traction After Anterior Cervical Diskectomy and FusionOscar NgAinda não há avaliações
- Food and Exercise LogDocumento24 páginasFood and Exercise LogmhetfieldAinda não há avaliações
- Maths On The Move' - Effectiveness of Physically-Active Lessons For Learning Maths and Increasing Physical Activity in Primary School StudentsDocumento22 páginasMaths On The Move' - Effectiveness of Physically-Active Lessons For Learning Maths and Increasing Physical Activity in Primary School Studentsiisu-cmse libraryAinda não há avaliações
- Human Osteology at Wharram PercyDocumento2 páginasHuman Osteology at Wharram PercyMichael Lovejoy100% (1)
- Crabtales 061Documento20 páginasCrabtales 061Crab TalesAinda não há avaliações
- Acupuncture Has Been Used For Thousands of YearsDocumento13 páginasAcupuncture Has Been Used For Thousands of Yearsoluwasegun DavidAinda não há avaliações
- Statement On Controlled Organ Donation After Circulatory DeathDocumento10 páginasStatement On Controlled Organ Donation After Circulatory DeathHeidi ReyesAinda não há avaliações
- Demand and ElasticityDocumento5 páginasDemand and ElasticityCorey Crismon100% (1)
- GupisoneDocumento7 páginasGupisoneahibba.03862Ainda não há avaliações
- Fphar 12 768268Documento25 páginasFphar 12 768268Araceli Anaya AlvaradoAinda não há avaliações
- Route of Administration PDFDocumento45 páginasRoute of Administration PDFBurhan MubasharAinda não há avaliações
- Ergogenic Aids 1Documento24 páginasErgogenic Aids 1unattractiveyouAinda não há avaliações
- Records of Patient Medical CheckupsDocumento237 páginasRecords of Patient Medical CheckupsPanca WirawanAinda não há avaliações
- Medical Marijuana Dispensary ApplicationsDocumento7 páginasMedical Marijuana Dispensary Applicationsvcarey7524Ainda não há avaliações
- The Abc of Handover: E.D. Registrar A: Areas AllocationDocumento1 páginaThe Abc of Handover: E.D. Registrar A: Areas AllocationDiahNiatiAinda não há avaliações
- Candida Albicans and IridologyDocumento8 páginasCandida Albicans and IridologyFRANCISCO JAVIER GALEANOAinda não há avaliações
- 11 16 16Documento22 páginas11 16 16WoodsAinda não há avaliações