Você também pode gostar
- Pharmacology Drug Chart: Drug Name Receptor Therapeutic Uses Adverse EffectsDocumento18 páginasPharmacology Drug Chart: Drug Name Receptor Therapeutic Uses Adverse EffectsPadmavathy Naidu Chokkapu100% (2)
- 100 Essential Drugs1Documento8 páginas100 Essential Drugs1Sudip DevadasAinda não há avaliações
- Critical Care Drug Reference SheetDocumento12 páginasCritical Care Drug Reference SheetYanina CoxAinda não há avaliações
- Diabetes MedicationDocumento3 páginasDiabetes MedicationRuben Gutierrez-ArizacaAinda não há avaliações
- Lab Values Chart GuideDocumento5 páginasLab Values Chart GuideVanessaMUeller100% (3)
- Antibiotics ChartDocumento10 páginasAntibiotics Chartadom09Ainda não há avaliações
- AntimicrobialsDocumento1 páginaAntimicrobialsRomaine Barrett100% (1)
- Common infections and recommended antibioticsDocumento3 páginasCommon infections and recommended antibioticsNicole BerryAinda não há avaliações
- Bumetanide Torsemide: Desmopressin - V2Documento1 páginaBumetanide Torsemide: Desmopressin - V2med testAinda não há avaliações
- Local Anesthetics - Blockers K+ Channel Blockers Ca2+ Channel BlockersDocumento4 páginasLocal Anesthetics - Blockers K+ Channel Blockers Ca2+ Channel Blockersmed testAinda não há avaliações
- Labs Electrolyte ChartDocumento1 páginaLabs Electrolyte ChartmdcmepAinda não há avaliações
- Common MedicationsDocumento4 páginasCommon MedicationsFatima CarricoAinda não há avaliações
- Test InformationDocumento5 páginasTest InformationCatalina BorquezAinda não há avaliações
- Common Medications UsedDocumento3 páginasCommon Medications UsedRay Michael CasupananAinda não há avaliações
- Ninja - Anti-HTN PDFDocumento6 páginasNinja - Anti-HTN PDFErica Hyeyeon Lee100% (2)
- Cardiac Meds CompleteDocumento3 páginasCardiac Meds CompleteDanielle100% (2)
- Antibiotics Chart 1Documento7 páginasAntibiotics Chart 1Vee MendAinda não há avaliações
- Sphere: These DiarrheaDocumento3 páginasSphere: These Diarrheamed testAinda não há avaliações
- Approximate Equivalents:: 0.100 Gmn. 1.00 GMDocumento8 páginasApproximate Equivalents:: 0.100 Gmn. 1.00 GMakane ryuAinda não há avaliações
- Drug Names - Stems, Prefixes, Roots and Suffixes - NCLEX MasteryDocumento5 páginasDrug Names - Stems, Prefixes, Roots and Suffixes - NCLEX MasteryMarcel YoungAinda não há avaliações
- Antibiotics Chart 2Documento10 páginasAntibiotics Chart 2Vee MendAinda não há avaliações
- Urinary Tract and Bladder DrugsDocumento2 páginasUrinary Tract and Bladder Drugslhayes1234100% (2)
- NSAIDS and SteroidsDocumento2 páginasNSAIDS and Steroidsmed testAinda não há avaliações
- Diabetes Medications Chart PDFDocumento1 páginaDiabetes Medications Chart PDFRachel Lalaine Marie SialanaAinda não há avaliações
- Git Drugs TablesDocumento3 páginasGit Drugs TablesSulochan Ssplendid Splinterr Lohani100% (1)
- Respiratory and Cardiovascular DrugsDocumento21 páginasRespiratory and Cardiovascular DrugsCandace Flowers100% (3)
- Pharmacology of Cardiac Diseases MINEDocumento3 páginasPharmacology of Cardiac Diseases MINEMitu Miressa تAinda não há avaliações
- Antibiotic TableDocumento7 páginasAntibiotic TablenkuligowskiAinda não há avaliações
- Diabetes DrugsDocumento1 páginaDiabetes Drugsmed testAinda não há avaliações
- Musculoskeletal PharmacologyDocumento18 páginasMusculoskeletal PharmacologyBLEEMAGE100% (2)
- Drug CardDocumento1 páginaDrug CardPaul AlfonsoAinda não há avaliações
- Heart Rhythms S SDocumento3 páginasHeart Rhythms S SGloryJane100% (1)
- Drug of ChoiceDocumento2 páginasDrug of ChoiceRia Tiglao Fortugaliza100% (1)
- Medications and assessmentsDocumento225 páginasMedications and assessmentsJessica 'Baker' IsaacsAinda não há avaliações
- 0.5. ANS Quicksheet PDFDocumento1 página0.5. ANS Quicksheet PDFErica Hyeyeon LeeAinda não há avaliações
- GI Drugs PDFDocumento6 páginasGI Drugs PDFErica Hyeyeon Lee100% (1)
- Anemia ChartDocumento1 páginaAnemia ChartBetsy Brown ByersmithAinda não há avaliações
- Pain and Inflammation Med ChartsDocumento4 páginasPain and Inflammation Med Chartssurviving nursing school100% (1)
- Comprehensive Nclex Notes Easy To Read PDFDocumento97 páginasComprehensive Nclex Notes Easy To Read PDFKenia GeorgesAinda não há avaliações
- NCLEX Review: Pharmacology Charlene Natale, BSN, RNDocumento43 páginasNCLEX Review: Pharmacology Charlene Natale, BSN, RNMenly Susada100% (1)
- Common Cardiac Related MedicationsDocumento18 páginasCommon Cardiac Related MedicationsTracy100% (2)
- Blood Test Reference GuideDocumento3 páginasBlood Test Reference GuideHAinda não há avaliações
- Lang 10 EditionDocumento235 páginasLang 10 Editionraju niraulaAinda não há avaliações
- Drugs WorksheetDocumento16 páginasDrugs Worksheetninja-2001Ainda não há avaliações
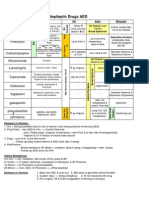
- Antiepileptic Drugs AED: D' DI Disadv SE AdvDocumento1 páginaAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88Ainda não há avaliações
- Introduction to commonly used antibioticsDocumento2 páginasIntroduction to commonly used antibioticsAmir AmirulAinda não há avaliações
- Med Geeks Clinical Lab GuideDocumento17 páginasMed Geeks Clinical Lab GuideHuy Hoang100% (1)
- Antiarrhythmic Medication Chart - EBM Consult v3Documento2 páginasAntiarrhythmic Medication Chart - EBM Consult v3Linlin100% (1)
- Anti Infective Drug ChartDocumento1 páginaAnti Infective Drug ChartJessica100% (1)
- Northern Ireland Management of Infection Guidelines For Primary and Community Care 2016Documento48 páginasNorthern Ireland Management of Infection Guidelines For Primary and Community Care 2016dreneavalentinstefanAinda não há avaliações
- Drugs of ChoiceDocumento3 páginasDrugs of ChoiceReeti R. Bhat100% (1)
- Cell Wall Inhibitors and Protein Synthesis Inhibitors Antibiotics Mechanisms of ActionDocumento3 páginasCell Wall Inhibitors and Protein Synthesis Inhibitors Antibiotics Mechanisms of Actionyanks1120Ainda não há avaliações
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsAinda não há avaliações
- Lab Values: An Easy Guide to Learn Everything You Need to Know About Laboratory Medicine and Its Relevance in Diagnosing DiseaseNo EverandLab Values: An Easy Guide to Learn Everything You Need to Know About Laboratory Medicine and Its Relevance in Diagnosing DiseaseNota: 5 de 5 estrelas5/5 (2)
- Literature ReviewDocumento4 páginasLiterature Reviewapi-549241187Ainda não há avaliações
- Librarianship and Professional Ethics: Understanding Standards for Library ProfessionalsDocumento12 páginasLibrarianship and Professional Ethics: Understanding Standards for Library ProfessionalsHALLAinda não há avaliações
- Think Like An EconomistDocumento34 páginasThink Like An EconomistDiv-yuh BothraAinda não há avaliações
- Are Moral Principles Determined by SocietyDocumento2 páginasAre Moral Principles Determined by SocietyKeye HiterozaAinda não há avaliações
- Bible Study RisksDocumento6 páginasBible Study RisksVincentAinda não há avaliações
- Why Research Is Important in The BusinessDocumento2 páginasWhy Research Is Important in The BusinessBricx BalerosAinda não há avaliações
- Assessment Explanation of The Problem Outcomes Interventions Rationale Evaluation Sto: STO: (Goal Met)Documento3 páginasAssessment Explanation of The Problem Outcomes Interventions Rationale Evaluation Sto: STO: (Goal Met)Arian May MarcosAinda não há avaliações
- ADSL Line Driver Design Guide, Part 2Documento10 páginasADSL Line Driver Design Guide, Part 2domingohAinda não há avaliações
- St. Louis ChemicalDocumento8 páginasSt. Louis ChemicalNaomi Alberg-BlijdAinda não há avaliações
- ARCH1350 Solutions 6705Documento16 páginasARCH1350 Solutions 6705Glecy AdrianoAinda não há avaliações
- We Don't Eat Our: ClassmatesDocumento35 páginasWe Don't Eat Our: ClassmatesChelle Denise Gumban Huyaban85% (20)
- The Republic of LOMAR Sovereignty and International LawDocumento13 páginasThe Republic of LOMAR Sovereignty and International LawRoyalHouseofRA UruguayAinda não há avaliações
- Culture of BMWDocumento6 páginasCulture of BMWhk246100% (1)
- Kurukshetra English August '17Documento60 páginasKurukshetra English August '17amit2688Ainda não há avaliações
- Ashe v. Swenson, 397 U.S. 436 (1970)Documento25 páginasAshe v. Swenson, 397 U.S. 436 (1970)Scribd Government DocsAinda não há avaliações
- Hitachi Datasheet Thin Image SnapshotDocumento2 páginasHitachi Datasheet Thin Image Snapshotemail7urangAinda não há avaliações
- Chapter 5 Quiz Corrections ADocumento4 páginasChapter 5 Quiz Corrections Aapi-244140508Ainda não há avaliações
- Javier Couso, Alexandra Huneeus, Rachel Sieder Cultures of Legality Judicialization and Political Activism in Latin America Cambridge Studies in Law and SocietyDocumento290 páginasJavier Couso, Alexandra Huneeus, Rachel Sieder Cultures of Legality Judicialization and Political Activism in Latin America Cambridge Studies in Law and SocietyLívia de SouzaAinda não há avaliações
- Debt Recovery Management of SBIDocumento128 páginasDebt Recovery Management of SBIpranjalamishra100% (6)
- Ernst & Young: Public Sector Compensation ReviewDocumento88 páginasErnst & Young: Public Sector Compensation ReviewThe Vancouver SunAinda não há avaliações
- Marwar Steel Tubes Pipes StudyDocumento39 páginasMarwar Steel Tubes Pipes Studydeepak kumarAinda não há avaliações
- Sexual Self PDFDocumento23 páginasSexual Self PDFEden Faith Aggalao100% (1)
- Comparative Ethnographies: State and Its MarginsDocumento31 páginasComparative Ethnographies: State and Its MarginsJuan ManuelAinda não há avaliações
- Dwi Athaya Salsabila - Task 4&5Documento4 páginasDwi Athaya Salsabila - Task 4&521Dwi Athaya SalsabilaAinda não há avaliações
- The Art of Woodworking Shaker FurnitureDocumento147 páginasThe Art of Woodworking Shaker Furnituremalefikus100% (2)
- S The Big Five Personality TestDocumento4 páginasS The Big Five Personality TestXiaomi MIX 3Ainda não há avaliações
- Benchmarking The Formation Damage of Drilling FluidsDocumento11 páginasBenchmarking The Formation Damage of Drilling Fluidsmohamadi42Ainda não há avaliações
- Week 1 Amanda CeresaDocumento2 páginasWeek 1 Amanda CeresaAmanda CeresaAinda não há avaliações
- Intrinsic Resistance and Unusual Phenotypes Tables v3.2 20200225Documento12 páginasIntrinsic Resistance and Unusual Phenotypes Tables v3.2 20200225Roy MontoyaAinda não há avaliações
- Christian Appraisal of Feminist Ideologies Among Nigerian Women 2020Documento78 páginasChristian Appraisal of Feminist Ideologies Among Nigerian Women 2020Nwaozuru JOHNMAJOR ChinecheremAinda não há avaliações