Você também pode gostar
- Hilton Head Relocation GuideDocumento50 páginasHilton Head Relocation GuidebernardhhiAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Footloose Playbill FinalDocumento6 páginasFootloose Playbill Finalbernardhhi100% (3)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Julie Toon Pawley ResumeDocumento1 páginaJulie Toon Pawley Resumebernardhhi100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Heroes On Horseback Summer 08 NewsletterDocumento2 páginasHeroes On Horseback Summer 08 NewsletterbernardhhiAinda não há avaliações
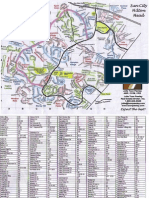
- Sun City Hilton Head Street Map-JTPDocumento2 páginasSun City Hilton Head Street Map-JTPbernardhhi100% (3)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Ladybird Book - The PolicemanDocumento15 páginasLadybird Book - The Policemanbernardhhi91% (11)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- JanFeb 08 WebDocumento16 páginasJanFeb 08 WebbernardhhiAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Heroes On Horseback Participant Registration and Photo Release FormDocumento11 páginasHeroes On Horseback Participant Registration and Photo Release FormbernardhhiAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Spring 2008 Continuing-Registration-FormDocumento1 páginaSpring 2008 Continuing-Registration-FormbernardhhiAinda não há avaliações
- Summer 2008 Continuing-Registration-FormDocumento1 páginaSummer 2008 Continuing-Registration-FormbernardhhiAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- HOH Volunteer FormsDocumento4 páginasHOH Volunteer FormsbernardhhiAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Participant Registration FORMSDocumento6 páginasParticipant Registration FORMSbernardhhi100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Set2 Cases SpeproDocumento58 páginasSet2 Cases SpeproLynetth LclAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Child CustodyDocumento10 páginasChild CustodyZohaib AhmedAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Raja Ram Vs State of HaryanaDocumento15 páginasRaja Ram Vs State of HaryanamohitpalsinghgorayaAinda não há avaliações
- TORT Midterm ExamDocumento6 páginasTORT Midterm ExamJenieAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- IRR RA No. 9048 - EditedDocumento3 páginasIRR RA No. 9048 - EditedEfeiluj CuencaAinda não há avaliações
- 3917en How To Write A DeclarationDocumento19 páginas3917en How To Write A DeclarationPheletso Rigdway100% (1)
- Judge Munro, Horowitz, Krieger, Marilou Giovannucci's Presentations at The 2013 AFCC ConferenceDocumento63 páginasJudge Munro, Horowitz, Krieger, Marilou Giovannucci's Presentations at The 2013 AFCC ConferenceJournalistABC50% (2)
- Abdul Haye AbroDocumento17 páginasAbdul Haye AbrorainaAinda não há avaliações
- Guardianship Workshop Script: Parent of The Child Who Seeks A Court Order For Legal Custody of A Minor ChildDocumento3 páginasGuardianship Workshop Script: Parent of The Child Who Seeks A Court Order For Legal Custody of A Minor ChildKkkkkkkkAinda não há avaliações
- High Court 1991 7Documento3 páginasHigh Court 1991 7suakelloAinda não há avaliações
- 017 - USAID Development Assistance Specialist PDFDocumento7 páginas017 - USAID Development Assistance Specialist PDFAiméOuedraogoAinda não há avaliações
- Child Workers: Ra 7610 As Amended by Ra 7658 and Ra 9231 Arts 137 & 138 Labor CodeDocumento22 páginasChild Workers: Ra 7610 As Amended by Ra 7658 and Ra 9231 Arts 137 & 138 Labor CodeKate GaroAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Form 28 Petition For Temporary Letters of Guardianship of MinorDocumento18 páginasForm 28 Petition For Temporary Letters of Guardianship of MinorSheryar AfridiAinda não há avaliações
- North Carolina Chapter-04 - Bench-Book - 2017-1 PDFDocumento172 páginasNorth Carolina Chapter-04 - Bench-Book - 2017-1 PDFJustice CauseAinda não há avaliações
- ObliCon Week1Documento86 páginasObliCon Week1Que LlyAinda não há avaliações
- In Re Petition For Adoption of Michelle Lim Full TextDocumento3 páginasIn Re Petition For Adoption of Michelle Lim Full TextOfelia RagpaAinda não há avaliações
- Skate Zone WaiverDocumento1 páginaSkate Zone WaiverBrittany SmithAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Assent Morris Et Al 2021Documento17 páginasAssent Morris Et Al 2021Carolina SilveiraAinda não há avaliações
- Parental Authority ReviewerDocumento15 páginasParental Authority Reviewerdoraemon100% (1)
- Bcal-3731 212621 7 Child Information RecordDocumento1 páginaBcal-3731 212621 7 Child Information Recordapi-261936496Ainda não há avaliações
- Guardianship Cases - LOLITA R. ALAMAYRI VS. ROMMEL, ELMER, ERWIN, ROILER and AMANDA, All Surnamed PABALEDocumento19 páginasGuardianship Cases - LOLITA R. ALAMAYRI VS. ROMMEL, ELMER, ERWIN, ROILER and AMANDA, All Surnamed PABALEAnonymous VG51PNxIAyAinda não há avaliações
- Persons With DisabilitiesDocumento15 páginasPersons With DisabilitiesAmber AhluwaliaAinda não há avaliações
- Example Policy and Procedure: Implementation of Advance Care Planning in Residential Aged Care FacilitiesDocumento23 páginasExample Policy and Procedure: Implementation of Advance Care Planning in Residential Aged Care FacilitiesMax RamirezAinda não há avaliações
- Jurisprudence CustodyDocumento10 páginasJurisprudence CustodyChristine Denise AbuelAinda não há avaliações
- Ra 6809Documento3 páginasRa 6809Dairen Canlas50% (2)
- Succession DigestDocumento4 páginasSuccession DigestHenson Montalvo100% (1)
- KHSAA Physical FormDocumento7 páginasKHSAA Physical Formkbarrier214Ainda não há avaliações
- 2) Terry Schiavo CaseDocumento2 páginas2) Terry Schiavo CaseAj Guadalupe de MataAinda não há avaliações
- Rules of Conduct and Distributor PoliciesDocumento71 páginasRules of Conduct and Distributor Policiesrubylyngulmatico0% (1)
- Consolidated Spec Proceedings Notes FinalDocumento55 páginasConsolidated Spec Proceedings Notes FinalsapphirealmondsAinda não há avaliações