Você também pode gostar
- Ear Health 101: The Complete Guide to Understanding Ear InfectionsNo EverandEar Health 101: The Complete Guide to Understanding Ear InfectionsAinda não há avaliações
- Meningitis and Childhood Deafness: A Guide For FamiliesDocumento36 páginasMeningitis and Childhood Deafness: A Guide For FamiliesNguyễn YếnAinda não há avaliações
- Listen: What'S in This Article?Documento6 páginasListen: What'S in This Article?KamlaAinda não há avaliações
- ACPA Booklet Helpwithhearing WebDocumento16 páginasACPA Booklet Helpwithhearing WebAhmed AshfaqAinda não há avaliações
- Descriptions of Hearing LossDocumento8 páginasDescriptions of Hearing LossPesántez Franco GemaAinda não há avaliações
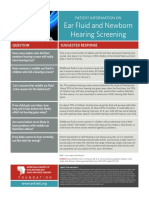
- Ear Fluid and Newborn Hearing Screening: Patient Information OnDocumento1 páginaEar Fluid and Newborn Hearing Screening: Patient Information OnMerlin NoronhaAinda não há avaliações
- Your Guide To Better Hearing. VisitDocumento32 páginasYour Guide To Better Hearing. VisitPhonac Hearing CentreAinda não há avaliações
- 683 2Documento15 páginas683 2M Noaman AkbarAinda não há avaliações
- HearinglossfactsheetDocumento2 páginasHearinglossfactsheetapi-239968581Ainda não há avaliações
- Papers About EarsDocumento24 páginasPapers About EarsFajra FajiraAinda não há avaliações
- Hearing Impairment: HistoryDocumento3 páginasHearing Impairment: HistoryNorence BuenoAinda não há avaliações
- EZRIHDocumento7 páginasEZRIHMuneYakitoriAinda não há avaliações
- HSC 430 Childhood Disease PaperDocumento10 páginasHSC 430 Childhood Disease Paperapi-502687231Ainda não há avaliações
- Medicina: The Importance of Early Genetic Diagnostics of Hearing Loss in ChildrenDocumento13 páginasMedicina: The Importance of Early Genetic Diagnostics of Hearing Loss in ChildrenAsniar RAinda não há avaliações
- Deafness and Hearing LossDocumento6 páginasDeafness and Hearing Lossapi-281466418100% (1)
- TEXTO 7 Ingl I What Is Hearing Loss 2CDocumento4 páginasTEXTO 7 Ingl I What Is Hearing Loss 2Ccande cáceresAinda não há avaliações
- The Importance of Early Intervention of Hearing Impaired ChildrenDocumento4 páginasThe Importance of Early Intervention of Hearing Impaired ChildrenAkhsaful ImamAinda não há avaliações
- Hearing ImpairementDocumento8 páginasHearing ImpairementMARY KENNETH SILVOSAAinda não há avaliações
- Noise Induced Hearing LossDocumento4 páginasNoise Induced Hearing LossrrrawAinda não há avaliações
- 4 Steps To Severe Hearing Loss TreatmentDocumento8 páginas4 Steps To Severe Hearing Loss TreatmentTon SawyerAinda não há avaliações
- An Educator's Guide To Hearing Disability Issues: Gender Bias Accessibility Funding Visual Disability Other DisabilitiesDocumento13 páginasAn Educator's Guide To Hearing Disability Issues: Gender Bias Accessibility Funding Visual Disability Other DisabilitiesMukarram AbdulnabeeAinda não há avaliações
- Earproblemsinchildren WithcleftpalatesDocumento3 páginasEarproblemsinchildren Withcleftpalatesane_dokter1905Ainda não há avaliações
- Lecture 8 Advanced Developmental StudiesDocumento39 páginasLecture 8 Advanced Developmental StudiesDr Muhammad NadeemAinda não há avaliações
- Causes of Hearing LossDocumento2 páginasCauses of Hearing LossTitaniasAppleAinda não há avaliações
- Gatau Ini ApaDocumento6 páginasGatau Ini ApaAlfa KaromahAinda não há avaliações
- Bab I Pendahuluan 1.1 Latar BelakangDocumento4 páginasBab I Pendahuluan 1.1 Latar BelakangdesmawitaAinda não há avaliações
- Hearing Tests For Babies and Young ChildrenDocumento6 páginasHearing Tests For Babies and Young Childrengwenkz011Ainda não há avaliações
- Hearing LossDocumento31 páginasHearing LossDat boi100% (1)
- Hearing Loss in Children - Etiology - UpToDateDocumento39 páginasHearing Loss in Children - Etiology - UpToDateAlexander AdrielAinda não há avaliações
- Mayo Clinic on Better Hearing and Balance: Strategies to Restore Hearing, Manage Dizziness and Much MoreNo EverandMayo Clinic on Better Hearing and Balance: Strategies to Restore Hearing, Manage Dizziness and Much MoreAinda não há avaliações
- Otitis Media With E UsionDocumento10 páginasOtitis Media With E UsionMas KaryonAinda não há avaliações
- Part C.3 and AnsDocumento10 páginasPart C.3 and AnsKhang VõAinda não há avaliações
- Diagnosis and Management of Congenital Sensorineural Hearing LossDocumento10 páginasDiagnosis and Management of Congenital Sensorineural Hearing LossAlifia Nurdani DarmawanAinda não há avaliações
- Tugas Inggris KMB MGG 1-3Documento6 páginasTugas Inggris KMB MGG 1-3Julia Wibawa HaryantoAinda não há avaliações
- Unilateral Hearing LossDocumento16 páginasUnilateral Hearing LossMarília Barbieri PereiraAinda não há avaliações
- Hearing ImpairmentDocumento7 páginasHearing ImpairmentIrene MendozaAinda não há avaliações
- To Study The Incidence of Sensorineural Hearing Loss Post Meningitis in NeonatesDocumento7 páginasTo Study The Incidence of Sensorineural Hearing Loss Post Meningitis in NeonatesIJAR JOURNALAinda não há avaliações
- Hearing A New Voice-Final DraftDocumento12 páginasHearing A New Voice-Final Draftapi-609395904Ainda não há avaliações
- Jurnal Otitis MediaDocumento33 páginasJurnal Otitis MediaFredy RizkiAinda não há avaliações
- whd2016 Brochure en 2Documento16 páginaswhd2016 Brochure en 2api-311125682Ainda não há avaliações
- Tinnitus 2019Documento20 páginasTinnitus 2019Leslie Lindsay AlvarezAinda não há avaliações
- Äc 0 ' C C C +C C C C % C& C C C %C ' C 'CDocumento5 páginasÄc 0 ' C C C +C C C C % C& C C C %C ' C 'CwhoisthatgirlalouAinda não há avaliações
- Childhood Deafness With AllDocumento63 páginasChildhood Deafness With AllMunadiAinda não há avaliações
- Anatomy and Physiology of The EarDocumento6 páginasAnatomy and Physiology of The EarrizzarAinda não há avaliações
- Hearing Loss in Children - Treatment - UpToDateDocumento13 páginasHearing Loss in Children - Treatment - UpToDateAlexander AdrielAinda não há avaliações
- Enlarged Vestibular Aqueducts and Childhood Deafness PDFDocumento20 páginasEnlarged Vestibular Aqueducts and Childhood Deafness PDFNics GanoAinda não há avaliações
- Assessing Ears: Cos, Dimple J. Danao, Vina de Jesus, Manuela Marie BSN1-ADocumento36 páginasAssessing Ears: Cos, Dimple J. Danao, Vina de Jesus, Manuela Marie BSN1-ADimple CosAinda não há avaliações
- What Is An Ear InfectionDocumento3 páginasWhat Is An Ear InfectionGladie Ann Dela RosaAinda não há avaliações
- jpg20005 1215 1215Documento1 páginajpg20005 1215 1215Rahma R SAinda não há avaliações
- Your Baby's Hearing Screening and Next StepsDocumento6 páginasYour Baby's Hearing Screening and Next Stepsrameezchaudhary964Ainda não há avaliações
- m8 KimDocumento3 páginasm8 KimKimberly CarmenAinda não há avaliações
- Causes of Hearing Loss, Deafness, and Tinnitus/Ringing Ears - Information From NOWiHEAR ProfessionalsDocumento6 páginasCauses of Hearing Loss, Deafness, and Tinnitus/Ringing Ears - Information From NOWiHEAR Professionalscheerfulnecessi98Ainda não há avaliações
- Hearing Impairment by Nyanga KeyDocumento4 páginasHearing Impairment by Nyanga KeyMbuyoti KanyataAinda não há avaliações
- MSN 2 Short AnswersDocumento39 páginasMSN 2 Short AnswersTijoAinda não há avaliações
- Otitis MediaDocumento7 páginasOtitis MediaNader Smadi67% (3)
- Anotia/Microtia: Minnesota Department of Health Fact Sheet November 2005Documento3 páginasAnotia/Microtia: Minnesota Department of Health Fact Sheet November 2005Carlos Santiago VivenzaAinda não há avaliações
- Noise and Hearing Loss: A Review: Eneral RticleDocumento8 páginasNoise and Hearing Loss: A Review: Eneral RticleMacarena Ignacia AniñirAinda não há avaliações
- Topnotch Ent Supplement Handout Updated April 2016pdf PDFDocumento15 páginasTopnotch Ent Supplement Handout Updated April 2016pdf PDFKenneth NuñezAinda não há avaliações
- IPT Intro To Dental Anatomy Tooth Dental DentistryDocumento37 páginasIPT Intro To Dental Anatomy Tooth Dental DentistryAnonymous OWjCHMOAinda não há avaliações
- 3rd Year Q.BankDocumento128 páginas3rd Year Q.BankMòháñ DonnAinda não há avaliações
- What To Know About Eyebrow TransplantsDocumento5 páginasWhat To Know About Eyebrow TransplantsOliver Carrasco VilladomaAinda não há avaliações
- Adenoidectomy and Tonsillectomy 2Documento27 páginasAdenoidectomy and Tonsillectomy 2DR AAMAinda não há avaliações
- Head Trauma: Adhitya Rahadi, M.DDocumento50 páginasHead Trauma: Adhitya Rahadi, M.DNatasya Saraswati100% (1)
- 1st Lecture On Physiology of Eye by Dr. RoomiDocumento30 páginas1st Lecture On Physiology of Eye by Dr. RoomiMudassar Roomi100% (1)
- Nursing Health Assessment 3rd Edition Dillon Test BankDocumento6 páginasNursing Health Assessment 3rd Edition Dillon Test BankPrestonTaylorfper100% (42)
- Youssef Yahia 212140098 Orthodontics Dept Copy 221116 075352Documento8 páginasYoussef Yahia 212140098 Orthodontics Dept Copy 221116 075352Karizma TravelAinda não há avaliações
- Maxillary Width and Hard Palate Thickness in Men and Women With Different Vertical and Sagittal Skeletal PatternsDocumento10 páginasMaxillary Width and Hard Palate Thickness in Men and Women With Different Vertical and Sagittal Skeletal PatternsLily CAAinda não há avaliações
- Vertigo and DizzinessDocumento50 páginasVertigo and DizzinessAshraf HusseinAinda não há avaliações
- Find A Criminal (Appearance) by Gorina - TeacherDocumento36 páginasFind A Criminal (Appearance) by Gorina - TeacherMartaAinda não há avaliações
- Inferior Alveolar Nerve BlockDocumento16 páginasInferior Alveolar Nerve BlockhinawittyAinda não há avaliações
- MR Imaging of Olfactory BulbsDocumento3 páginasMR Imaging of Olfactory BulbsMustafa BaranAinda não há avaliações
- Denture Complaint PDFDocumento10 páginasDenture Complaint PDFFaheemuddin MuhammadAinda não há avaliações
- Malocclusion Class IIIDocumento33 páginasMalocclusion Class IIIAyat KewanAinda não há avaliações
- Stadium CA LaringDocumento4 páginasStadium CA LaringmunzirAinda não há avaliações
- Basic Sinus AnatomyDocumento71 páginasBasic Sinus AnatomyTalal AlanzyAinda não há avaliações
- MCQ Nemer 2Documento20 páginasMCQ Nemer 2adham bani younesAinda não há avaliações
- Local Anesthesia Technique HandoutDocumento2 páginasLocal Anesthesia Technique Handoutmirfanulhaq100% (1)
- Treatment Planning of ImplantsDocumento10 páginasTreatment Planning of ImplantsRussia Al ShboulAinda não há avaliações
- HydrocephalusDocumento40 páginasHydrocephalusAstrid Sabirin100% (1)
- Imaging of Cranial Nerves - A Pictorial OverviewDocumento39 páginasImaging of Cranial Nerves - A Pictorial OverviewValeria KuchkaryanAinda não há avaliações
- Dollz Face - OceanSubliminalsDocumento4 páginasDollz Face - OceanSubliminalsboldizsarkopaszAinda não há avaliações
- Retention and RelapseDocumento30 páginasRetention and RelapseDrNamrah DanishAinda não há avaliações
- Unusual Orthodontic Correction of Bilateral Maxillary Canine-First Premolar TranspositionDocumento11 páginasUnusual Orthodontic Correction of Bilateral Maxillary Canine-First Premolar TranspositionAstrid DindaAinda não há avaliações
- Anatomy of BrainstemDocumento66 páginasAnatomy of BrainstemFitria OctavianiAinda não há avaliações
- Have Something Done PRACTICEDocumento3 páginasHave Something Done PRACTICEMaría Vela FontisAinda não há avaliações
- Atlas of Thyroid UltrasonographyDocumento399 páginasAtlas of Thyroid Ultrasonographynino.matasAinda não há avaliações
- Examination of Lacrimal ApparatusDocumento23 páginasExamination of Lacrimal ApparatusDr. T. BalasubramanianAinda não há avaliações