IOSR Journal of Dental and Medical Sciences (IOSR-JDMS)
e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 13, Issue 6 Ver. I (Jun. 2014), PP 100-102
www.iosrjournals.org
www.iosrjournals.org 100 | Page
Lingual lobe of right lung- a rare variation
Mohanty S.R
1
, Yadav B
2
.
Kalinga Institute of Medical Sciences , Bhubaneswar. Smruti Rekha Mohanty , MS
Assistant Professor ,Department of Anatomy , Kalinga Institute of Medical Sciences ,
KIIT University ,Patia , Bhubaneswar-751024.Dist-Khurda ,State-Odisha INDIA
Abstract: Knowledge of variations of lobar pattern of lung is important for identification of broncho-
pulmonary segments. It is of great clinical significance for surgeons and radiologists. Normally the right lung
has two fissures, one oblique and one horizontal and three lobes, upper, middle and lower lobes. Many authors
have described the lobar variations on imaging techniques but a few studies have reported in gross anatomy.
The present case highlights an abnormal lingual lobe of the right lung which was detected incidentally during
the undergraduate dissection. Also it highlights the abnormal pattern of oblique and horizontal fissures.
Keywords: right lung, horizontal fissure, oblique fissure, lingual lobe, variation
I. Introduction
Incomplete fissures of lung are a common observations , but are often misinterpreted on radiographs
and computed scans. Lobar anatomy and broncho-pulmonary segments can be appreciated better with
knowledge of variations. Classically the right lung is divided into three lobes namely upper, middle and lower
by two fissures, an oblique and a horizontal. The oblique fissure runs downwards, thereby meeting the inferior
border of the lung at a distance of approximately 7.5cm behind anterior end (standring). The horizontal fissure,
passes from the anterior margin into the oblique fissure to separate a wedge shaped middle lobe from the upper
lobe. It passes at the level of midaxillary line to the anterior border of the lung at the level of sternal end of 4
th
costal cartilage.
The present case describes a S-shaped oblique fissure and incomplete curved horizontal fissure with
upward convexity and a pyriform shaped lingual lobe in between the two fissures.
II. Case Report
During routine dissection classes of thoracic region for the undergraduate students, an unusual lobar
variation of right lung was observed. The oblique fissure of right lung cut the posterior border of lung,6cms
from the apex of the lung. Another curved fissure commences at a distance of 16.5cms from the posterior
border. The curved fissure divided the oblique fissure into a cranial part and a caudal part. The curvature of the
oblique fissure was convexo-concave. The oblique fissure could be traced upto the lower end of hilum. The
curved fissure was well defined in its proximal part but at a distance of 3.5cms from the anterior border of right
lung it could not be delineated. A lingual lobe was observed between these two fissures. The maximum height
of the lingual lobe was 10.5cms and maximum width was 6.5cms.The distance between the lower end of oblique
fissure and the anterior border of right lung was 5cms.The distance between the anterior end of curved fissure
and the inferior border was 4cms.
III. Discussion
The right lung is divided into superior, middle and inferior lobes by two fissures, an oblique and a
horizontal (1). The oblique fissure separates the inferior lobe from middle and superior lobes and corresponds
closely to the left oblique fissure although it is less vertical, crossing the inferior border of the lung about 7.5cms
behind its anterior end. On the posterior border it is level with the spine of 4th thoracic vertebra or slightly
lower. It descends across the 5th intercostal space and follows the 6th rib to the 6th costochondral junction(2).
The short horizontal fissure separate the superior and middle lobes.It passes from the oblique fissure,
near the mid axillary line, horizontally forwards to the anterior border of the lung, level with the sternal end of
the 4th costal cartilage, then passes backwards to the hilum on the mediastinal surface. The small middle lobe is
thus cuneiform and includes some of the costal surface, the lower part of the anterior border and the anterior part
of the base of the lung (3).
During foetal life as the lung develops, the spaces of fissures that separate individual
bronchopulmonary buds or segments become obliterated except along the oblique and horizontal fissures (4).
Incomplete fissures could be result of abnormal obliterations of these fissures, partially or completely.
Knowledge of variations of incomplete fissures and lobes of lung is important for preoperative
planning strategy for pulmonary lobectomy and segmental resection of lung.(5). Incomplete fissure is also a
Lingual lobe of right lung- a rare variation
www.iosrjournals.org 101 | Page
cause for post operative air leakage (6). Incomplete fissures are also responsible for altering the spread of any
lung disease(7).
Anatomical knowledge of fissures of lung helps in differential diagnosis of chest diseases in case of
extension of fluid into an incomplete major fissure or spread of diseases through different pathways (8).
Incomplete fissures as recorded in the present case are often mistaken for the appearance of pleural effusion. (9).
The incomplete horizontal fissure in the present case also described an abnormal upward convex course and
along with sinuous course of lower part of oblique fissure, also there is variation in the middle lobe with tongue
like projection . The incompleteness, thick sections and orientation of fissures may obscure them during
radiographic procedure and increase clinicians dilemma (10).
It is proven fact that lymphatics of the lung drain centripetally from the pleura towards hilum (11). In
the present case, an abnormal course of horizontal fissure and lower part of oblique fissure would mean an
anomalous or altered course of visceral pleura, thereby changing the course and arrangement of lymphatic
drainage. An incomplete horizontal fissure as observed in the present case could be mistaken for a scar or a
pleural line made visible by pneumothorax (12).
IV. Conclusion
Considering the clinical importance of such variations, we as an anatomist opine that prior anatomical
knowledge for the presence of variations in fissures, lobes and broncho-pulmonary segments may be essential
for cardiothoracic surgeons and radiologists.
References
[1]. Standring S. Grays Anatomy. 40
th
Edition. Churchill Livingstone, 2008. pp-993
[2]. Walker WS & Craig SR. A proposed anatomical classification of the pulmonary fissures. J R Coll Surg Edinburgh 1997; 42(4):233-
4.
[3]. Godwin JD & Tarver RD. Accessory Fissures of the Lung. AJR 1985; 144(1):39-47.
[4]. Modgil V, Das S, Suri R K. Anomalous lobar pattern of right lung- A case report. Int J Morphol 2006; 24(1):5-6.
[5]. Meenakshi S, Manjunath K, Balasubramanyam V. Morphological Variations of the Lung Fissures and lobes. The Indian J of Chest
Diseases & Allied Sciences 2004; 46(3): 179-82.
[6]. Das S, Latiff AA, Othman FB et al. Topographical anatomy of anomalous oblique fissure and lingual of the lung. Braz J Morph Sci
2007; 24(3):155-56.
[7]. Rosse C, Gaddum-Rosse P. Hollinsheds Textbook of Anatomy. Philadelphia: Lipincott-Raven; 1997: 441-61.
[8]. Dandy WE. Incomplete pulmonary interlobar fissure sign. Radiology 1978; 1289(1):21-5.
[9]. [9].
[10]. Ellis H. Clinical Anatomy. A revision and applied anatomy for clinical students. 1
0th
ed. USA: Blackwell Publishing, 2002.
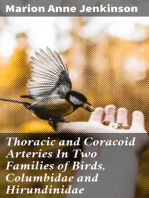
Figure1: Right lung showing the lingual lobe and incomplete curved horizontal fissure.(OF-Oblique fissure,CF-
Curved fissure,A-Anterior border,P-Posterior border,LL-Lingual lobe)
Lingual lobe of right lung- a rare variation
www.iosrjournals.org 102 | Page
Figure2: Medial surface of Right lung showing Lingual lobe.(OF-Oblique fissure,LL-Lingual lobe)
Você também pode gostar
- Anomalous Right Lung Lobes Case ReportDocumento2 páginasAnomalous Right Lung Lobes Case ReportMaría LejandraAinda não há avaliações
- Anatomical Study of Fissures and Lobes of Lung With Their Surgical and Imaging ImportanceDocumento5 páginasAnatomical Study of Fissures and Lobes of Lung With Their Surgical and Imaging ImportanceBIOMEDSCIDIRECT PUBLICATIONSAinda não há avaliações
- Anatomy and Histology of The Lung PDFDocumento30 páginasAnatomy and Histology of The Lung PDFramona100% (1)
- Lobes, Fissures, and Bronchopulmonary SegmentsDocumento13 páginasLobes, Fissures, and Bronchopulmonary SegmentsJansi OrtizAinda não há avaliações
- Chest X-ray Interpretation GuideDocumento101 páginasChest X-ray Interpretation GuideAnna DiaconuAinda não há avaliações
- Chest Imaging: DR - Wasan AliDocumento106 páginasChest Imaging: DR - Wasan AliRm98Ainda não há avaliações
- Chest X-RayDocumento101 páginasChest X-RayYuke04Ainda não há avaliações
- Pemeriksaan Fisik ParuDocumento17 páginasPemeriksaan Fisik ParuMuhammad Luthfi AziziAinda não há avaliações
- Hobai 2012Documento22 páginasHobai 2012CristianpalmarAinda não há avaliações
- Anatomical Considerations in Bronchoscopy - Journal of Thoracic Disease 2017Documento5 páginasAnatomical Considerations in Bronchoscopy - Journal of Thoracic Disease 2017MICHAEL AMARILLO CORREAAinda não há avaliações
- Anatomy of Lungs Histology of Airways by Dr. DilrukshiDocumento33 páginasAnatomy of Lungs Histology of Airways by Dr. DilrukshiOmar Ali AyoubkhanAinda não há avaliações
- Relevant Thoracic Anatomy: Jed A. GordenDocumento13 páginasRelevant Thoracic Anatomy: Jed A. GordenAndry Wahyudi AgusAinda não há avaliações
- Thoracic Imaging Radiographic BasicsDocumento130 páginasThoracic Imaging Radiographic BasicsIsak ShatikaAinda não há avaliações
- ABC ChestDocumento4 páginasABC ChestSintounAinda não há avaliações
- Cephalometric Evaluation and Measurement of The Upper Airway PDFDocumento13 páginasCephalometric Evaluation and Measurement of The Upper Airway PDFSoe San KyawAinda não há avaliações
- Lung Anatomy Guide: Structures, Lobes, and SegmentsDocumento47 páginasLung Anatomy Guide: Structures, Lobes, and SegmentsAmna YousafAinda não há avaliações
- Dissertation On Copd - by - Shivbalak (2013)Documento108 páginasDissertation On Copd - by - Shivbalak (2013)ShivBalakChauhanAinda não há avaliações
- Lumbarization of First Sacral VertebraDocumento4 páginasLumbarization of First Sacral VertebraangellisimalAinda não há avaliações
- Erdogmus Et Al 2014 - BonesDocumento8 páginasErdogmus Et Al 2014 - Bonesmattlight07Ainda não há avaliações
- XrayDocumento28 páginasXrayPravinAinda não há avaliações
- Ncbi - Nlm.nih - Gov-Anatomy and Physiology of Respiratory System Relevant To AnaesthesiaDocumento17 páginasNcbi - Nlm.nih - Gov-Anatomy and Physiology of Respiratory System Relevant To AnaesthesiaMyo KoAinda não há avaliações
- tmp3FED TMPDocumento3 páginastmp3FED TMPFrontiersAinda não há avaliações
- Bolu Seminar in Lungs 2Documento34 páginasBolu Seminar in Lungs 2Bamgbose OpeyemiAinda não há avaliações
- Part A: Surface Anatomy and Palpation of The Viscera of The Thorax and AbdomenDocumento14 páginasPart A: Surface Anatomy and Palpation of The Viscera of The Thorax and AbdomenHammad -ullahAinda não há avaliações
- Lobulated Spleen With A Fissure On Diaphragmatic Surface: RD RDDocumento7 páginasLobulated Spleen With A Fissure On Diaphragmatic Surface: RD RDShantu ShirurmathAinda não há avaliações
- AIPGMEE 2011 Question Paper With Answers PDFDocumento32 páginasAIPGMEE 2011 Question Paper With Answers PDFgayathri67% (3)
- Echocardiographic and morphological correlations in tetralogy of FallotDocumento11 páginasEchocardiographic and morphological correlations in tetralogy of FallotLuiggui PeraltaAinda não há avaliações
- 549-2. Article Text - Manuscript-2768-1-10-20151106Documento5 páginas549-2. Article Text - Manuscript-2768-1-10-20151106Estanislao MartinAinda não há avaliações
- How To Read X-RayDocumento8 páginasHow To Read X-RayPeterson Wachira HscAinda não há avaliações
- 2 1 Diseases of The Respiratory System Radiological Pathology DRDocumento43 páginas2 1 Diseases of The Respiratory System Radiological Pathology DRNatnael GetahunAinda não há avaliações
- Reduced Bronchial Subdivisions in BronchiectasisDocumento15 páginasReduced Bronchial Subdivisions in BronchiectasisyikuiAinda não há avaliações
- Chest X-Ray: Confirm DetailsDocumento14 páginasChest X-Ray: Confirm DetailsNosheen HafeezAinda não há avaliações
- LAKH SINGH JI Report 1 ST WithImages 202309263 2xinheritx1xinheritx - PDF 2Documento2 páginasLAKH SINGH JI Report 1 ST WithImages 202309263 2xinheritx1xinheritx - PDF 2dinusinghkAinda não há avaliações
- Case Report: Identification of The Transverse Mesocolon and Root of Small Bowel Mesentery A New Sign of PneumoperitoneumDocumento3 páginasCase Report: Identification of The Transverse Mesocolon and Root of Small Bowel Mesentery A New Sign of PneumoperitoneumKrsna DharmasyaAinda não há avaliações
- Pediatric Point-of-Care Lung UltrasonographyDocumento8 páginasPediatric Point-of-Care Lung UltrasonographycristianAinda não há avaliações
- 1229 6490 1 PB PDFDocumento10 páginas1229 6490 1 PB PDFSitti_HazrinaAinda não há avaliações
- Ojmi 2017101715394062Documento7 páginasOjmi 2017101715394062Proimagem Santa InêsAinda não há avaliações
- Bobillo Perez2019Documento21 páginasBobillo Perez2019Nisa Hermina PutriAinda não há avaliações
- Respiratory System 2011Documento99 páginasRespiratory System 2011Izzah Atqa100% (1)
- 28 Vidhya EtalDocumento5 páginas28 Vidhya EtaleditorijmrhsAinda não há avaliações
- Anatomy of the LungDocumento29 páginasAnatomy of the LungIoana GuțăAinda não há avaliações
- Chest X-Ray GuideDocumento49 páginasChest X-Ray GuideFadli Amali100% (1)
- 01 Surface Anatomy and Surface Landmarks For Thoracic SurgerDocumento17 páginas01 Surface Anatomy and Surface Landmarks For Thoracic SurgerStefanAinda não há avaliações
- Left Bronchus SyndromeDocumento3 páginasLeft Bronchus SyndromephobicmdAinda não há avaliações
- Essential Radio Logical Anatomy For The MRCS 0521728088Documento178 páginasEssential Radio Logical Anatomy For The MRCS 0521728088ranko98Ainda não há avaliações
- Jurnal ForensikDocumento15 páginasJurnal ForensikZoehelmy HusenAinda não há avaliações
- Anatomy 2Documento43 páginasAnatomy 2bikedet268Ainda não há avaliações
- Chest X-Ray FindingsDocumento169 páginasChest X-Ray FindingsВладимир КурпаянидиAinda não há avaliações
- Cervical Rib - A Short Case Study On Features, Incidence and Clinical CorrelationDocumento4 páginasCervical Rib - A Short Case Study On Features, Incidence and Clinical CorrelationInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Case Report: Pulmonary Sequestration: A Case Report and Literature ReviewDocumento4 páginasCase Report: Pulmonary Sequestration: A Case Report and Literature Reviewjo_jo_maniaAinda não há avaliações
- Thoracic and Coracoid Arteries In Two Families of Birds, Columbidae and HirundinidaeNo EverandThoracic and Coracoid Arteries In Two Families of Birds, Columbidae and HirundinidaeAinda não há avaliações
- Thoracic Radiology: A Guide for BeginnersNo EverandThoracic Radiology: A Guide for BeginnersIacopo CarboneAinda não há avaliações
- Lung Transplantation: Evolving Knowledge and New HorizonsNo EverandLung Transplantation: Evolving Knowledge and New HorizonsGanesh RaghuAinda não há avaliações
- Extracranial Carotid and Vertebral Artery Disease: Contemporary ManagementNo EverandExtracranial Carotid and Vertebral Artery Disease: Contemporary ManagementAinda não há avaliações
- Lung Disease in Rheumatoid ArthritisNo EverandLung Disease in Rheumatoid ArthritisAryeh FischerAinda não há avaliações
- The Effect of Instructional Methods and Locus of Control On Students' Speaking Ability (An Experimental Study in State Senior High School 01, Cibinong Bogor, West Java)Documento11 páginasThe Effect of Instructional Methods and Locus of Control On Students' Speaking Ability (An Experimental Study in State Senior High School 01, Cibinong Bogor, West Java)International Organization of Scientific Research (IOSR)Ainda não há avaliações
- Study The Changes in Al-Ahwaz Marshal Using Principal Component Analysis and Classification TechniqueDocumento9 páginasStudy The Changes in Al-Ahwaz Marshal Using Principal Component Analysis and Classification TechniqueInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Effects of Formative Assessment On Mathematics Test Anxiety and Performance of Senior Secondary School Students in Jos, NigeriaDocumento10 páginasEffects of Formative Assessment On Mathematics Test Anxiety and Performance of Senior Secondary School Students in Jos, NigeriaInternational Organization of Scientific Research (IOSR)100% (1)
- Youth Entrepreneurship: Opportunities and Challenges in IndiaDocumento5 páginasYouth Entrepreneurship: Opportunities and Challenges in IndiaInternational Organization of Scientific Research (IOSR)100% (1)
- Project Based Learning Tools Development On Salt Hydrolysis Materials Through Scientific ApproachDocumento5 páginasProject Based Learning Tools Development On Salt Hydrolysis Materials Through Scientific ApproachInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Necessary Evils of Private Tuition: A Case StudyDocumento6 páginasNecessary Evils of Private Tuition: A Case StudyInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Philosophical Analysis of The Theories of Punishment in The Context of Nigerian Educational SystemDocumento6 páginasPhilosophical Analysis of The Theories of Punishment in The Context of Nigerian Educational SystemInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Students' Perceptions of Grammar Teaching and Learning in English Language Classrooms in LibyaDocumento6 páginasStudents' Perceptions of Grammar Teaching and Learning in English Language Classrooms in LibyaInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Comparison of Selected Anthropometric and Physical Fitness Variables Between Offencive and Defencive Players of Kho-KhoDocumento2 páginasComparison of Selected Anthropometric and Physical Fitness Variables Between Offencive and Defencive Players of Kho-KhoInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Need of Non - Technical Content in Engineering EducationDocumento3 páginasNeed of Non - Technical Content in Engineering EducationInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Child Mortality Among Teenage Mothers in OJU MetropolisDocumento6 páginasChild Mortality Among Teenage Mothers in OJU MetropolisInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Geohydrological Study of Weathered Basement Aquifers in Oban Massif and Environs Southeastern Nigeria: Using Remote Sensing and Geographic Information System TechniquesDocumento14 páginasGeohydrological Study of Weathered Basement Aquifers in Oban Massif and Environs Southeastern Nigeria: Using Remote Sensing and Geographic Information System TechniquesInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Development of Dacum As Identification Technique On Job Competence Based-Curriculum in High Vocational EducationDocumento5 páginasDevelopment of Dacum As Identification Technique On Job Competence Based-Curriculum in High Vocational EducationInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Enhancing Pupils' Knowledge of Mathematical Concepts Through Game and PoemDocumento7 páginasEnhancing Pupils' Knowledge of Mathematical Concepts Through Game and PoemInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Comparison of Psychological Variables Within Different Positions of Players of The State Junior Boys Ball Badminton Players of ManipurDocumento4 páginasComparison of Psychological Variables Within Different Positions of Players of The State Junior Boys Ball Badminton Players of ManipurInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Comparison of Explosive Strength Between Football and Volley Ball Players of Jamboni BlockDocumento2 páginasComparison of Explosive Strength Between Football and Volley Ball Players of Jamboni BlockInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Factors Affecting Success of Construction ProjectDocumento10 páginasFactors Affecting Success of Construction ProjectInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- A Review On Refrigerants, and Effects On Global Warming For Making Green EnvironmentDocumento4 páginasA Review On Refrigerants, and Effects On Global Warming For Making Green EnvironmentInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Study of Effect of Rotor Speed, Combing-Roll Speed and Type of Recycled Waste On Rotor Yarn Quality Using Response Surface MethodologyDocumento9 páginasStudy of Effect of Rotor Speed, Combing-Roll Speed and Type of Recycled Waste On Rotor Yarn Quality Using Response Surface MethodologyInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Advancing Statistical Education Using Technology and Mobile DevicesDocumento9 páginasAdvancing Statistical Education Using Technology and Mobile DevicesInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Parametric Optimization of Single Cylinder Diesel Engine For Specific Fuel Consumption Using Palm Seed Oil As A BlendDocumento6 páginasParametric Optimization of Single Cylinder Diesel Engine For Specific Fuel Consumption Using Palm Seed Oil As A BlendInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Lipoproteins and Lipid Peroxidation in Thyroid DisordersDocumento6 páginasLipoproteins and Lipid Peroxidation in Thyroid DisordersInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Comparative Effect of Daily Administration of Allium Sativum and Allium Cepa Extracts On Alloxan Induced Diabetic RatsDocumento6 páginasComparative Effect of Daily Administration of Allium Sativum and Allium Cepa Extracts On Alloxan Induced Diabetic RatsInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Microencapsulation For Textile FinishingDocumento4 páginasMicroencapsulation For Textile FinishingInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Application of Xylanase Produced by Bacillus Megaterium in Saccharification, Juice Clarification and Oil Extraction From Jatropha Seed KernelDocumento8 páginasApplication of Xylanase Produced by Bacillus Megaterium in Saccharification, Juice Clarification and Oil Extraction From Jatropha Seed KernelInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Core Components of The Metabolic Syndrome in Nonalcohlic Fatty Liver DiseaseDocumento5 páginasCore Components of The Metabolic Syndrome in Nonalcohlic Fatty Liver DiseaseInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Research Analysis On Sustainability Opportunities and Challenges of Bio-Fuels Industry in IndiaDocumento7 páginasResearch Analysis On Sustainability Opportunities and Challenges of Bio-Fuels Industry in IndiaInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Auxin Induced Germination and Plantlet Regeneration Via Rhizome Section Culture in Spiranthes Sinensis (Pers.) Ames: A Vulnerable Medicinal Orchid of Kashmir HimalayaDocumento4 páginasAuxin Induced Germination and Plantlet Regeneration Via Rhizome Section Culture in Spiranthes Sinensis (Pers.) Ames: A Vulnerable Medicinal Orchid of Kashmir HimalayaInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Investigation of Wear Loss in Aluminium Silicon Carbide Mica Hybrid Metal Matrix CompositeDocumento5 páginasInvestigation of Wear Loss in Aluminium Silicon Carbide Mica Hybrid Metal Matrix CompositeInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Essays in ExistentialismDocumento4 páginasEssays in Existentialismafibaixzyhpqmc100% (2)
- HPC - 2022-JIAF - Guide-1.1Documento60 páginasHPC - 2022-JIAF - Guide-1.1Emmanuel LompoAinda não há avaliações
- 2004 Swamee, Prabhata K. Rathie, Pushpa N. - Exact Solutions For Normal Depth ProblemDocumento9 páginas2004 Swamee, Prabhata K. Rathie, Pushpa N. - Exact Solutions For Normal Depth Problemjosue.angelo9459Ainda não há avaliações
- Sheikh Yusuf Al-Qaradawi A Moderate Voice From TheDocumento14 páginasSheikh Yusuf Al-Qaradawi A Moderate Voice From ThedmpmppAinda não há avaliações
- Humboldt Scientific, Inc.: Normal Stress (Psi)Documento9 páginasHumboldt Scientific, Inc.: Normal Stress (Psi)Dilson Loaiza CruzAinda não há avaliações
- Speakout E3 B1+ U2 - Teachers BookDocumento20 páginasSpeakout E3 B1+ U2 - Teachers BookCarolinaAinda não há avaliações
- Determinants of Cash HoldingsDocumento26 páginasDeterminants of Cash Holdingspoushal100% (1)
- MWSS v. CADocumento15 páginasMWSS v. CAAlexander AbonadoAinda não há avaliações
- Socio Cultural Issues in The PHDocumento2 páginasSocio Cultural Issues in The PHNanami MumuzunoAinda não há avaliações
- Homework #3 - Coursera CorrectedDocumento10 páginasHomework #3 - Coursera CorrectedSaravind67% (3)
- 2018 CML Updates and Case Presentations: Washington University in ST Louis Medical SchoolDocumento113 páginas2018 CML Updates and Case Presentations: Washington University in ST Louis Medical SchoolIris GzlzAinda não há avaliações
- Political Science Most Important Questions Part 1 PDFDocumento2 páginasPolitical Science Most Important Questions Part 1 PDFJayateerth KulkarniAinda não há avaliações
- Flow Through AnnulusDocumento7 páginasFlow Through Annulusamir_hayfaAinda não há avaliações
- DIASS - Quarter3 - Module1 - Week1 - Pure and Applied Social Sciences - V2Documento18 páginasDIASS - Quarter3 - Module1 - Week1 - Pure and Applied Social Sciences - V2Stephanie Tamayao Lumbo100% (1)
- Report Daftar Penerima Kuota Telkomsel Dan Indosat 2021 FSEIDocumento26 páginasReport Daftar Penerima Kuota Telkomsel Dan Indosat 2021 FSEIHafizh ZuhdaAinda não há avaliações
- (Stem - Pc11T-Iie-1) : Self-Learning Home Task (SLHT) 5Documento7 páginas(Stem - Pc11T-Iie-1) : Self-Learning Home Task (SLHT) 5Naddy RetxedAinda não há avaliações
- Communicative Approach - ChomskyDocumento4 páginasCommunicative Approach - ChomskyMiss AbrilAinda não há avaliações
- 101 Poisons Guide for D&D PlayersDocumento16 páginas101 Poisons Guide for D&D PlayersmighalisAinda não há avaliações
- Kinder DLP Lesson-Exemplar-Week-25-Day-2Documento16 páginasKinder DLP Lesson-Exemplar-Week-25-Day-2Leonor BagnosAinda não há avaliações
- The Structure and Function of Large Biological Molecules: BiologyDocumento32 páginasThe Structure and Function of Large Biological Molecules: BiologyUyyykllAinda não há avaliações
- Pro ManualDocumento67 páginasPro ManualAlan De La FuenteAinda não há avaliações
- Arrest of Leila de Lima (Tweets)Documento74 páginasArrest of Leila de Lima (Tweets)Edwin MartinezAinda não há avaliações
- Prambanan Temple LegendDocumento1 páginaPrambanan Temple LegendClara NadaAinda não há avaliações
- Senior Java Developer With 4 Years Experience ResumeDocumento5 páginasSenior Java Developer With 4 Years Experience ResumedivaAinda não há avaliações
- Chap 006Documento50 páginasChap 006Martin TrịnhAinda não há avaliações
- Sid The Science Kid - The Ruler of Thumb Cd1.avi Sid The Science Kid - The Ruler of Thumb Cd2.aviDocumento27 páginasSid The Science Kid - The Ruler of Thumb Cd1.avi Sid The Science Kid - The Ruler of Thumb Cd2.avisheena2saAinda não há avaliações
- Civet CoffeeDocumento8 páginasCivet CoffeeAn NhiênAinda não há avaliações
- HDPS 1303 - 930425105424Documento6 páginasHDPS 1303 - 930425105424Cheryl LimAinda não há avaliações
- Code of EthicsDocumento8 páginasCode of EthicsviorelAinda não há avaliações
- Interpretative Translation Theory EvaluationDocumento13 páginasInterpretative Translation Theory EvaluationAnastasia MangoAinda não há avaliações