Você também pode gostar
- Approach in Lymphadenopathy in ChildrenDocumento14 páginasApproach in Lymphadenopathy in Childrennahiry100% (1)
- Problem-based Approach to Gastroenterology and HepatologyNo EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisAinda não há avaliações
- Herpes Zoster (Shingles) : Muhammad Abdullah Dept. of Dermatology DHQ Hospital FaisalabadDocumento26 páginasHerpes Zoster (Shingles) : Muhammad Abdullah Dept. of Dermatology DHQ Hospital FaisalabadwaleedAinda não há avaliações
- (Human Immunodeficiency Virus) &: Acquired Immune Deficiency SyndromeDocumento61 páginas(Human Immunodeficiency Virus) &: Acquired Immune Deficiency SyndromeGufron MustofaAinda não há avaliações
- Meningitis in Children 1204809002482509 3Documento48 páginasMeningitis in Children 1204809002482509 3Ali FalihAinda não há avaliações
- Microbiology - Bacteria Summary (Updated)Documento26 páginasMicrobiology - Bacteria Summary (Updated)moZZeltovAinda não há avaliações
- Measles Otherwise Known As Rubeola or Morbilli Is ADocumento2 páginasMeasles Otherwise Known As Rubeola or Morbilli Is AKAREEM WAHEEDAinda não há avaliações
- ID Bug chart-DKDocumento92 páginasID Bug chart-DKNeil M D'SouzaAinda não há avaliações
- Pyrexia of Unknown OriginDocumento55 páginasPyrexia of Unknown OriginsanjeevAinda não há avaliações
- Bacterial MeningitisDocumento1 páginaBacterial MeningitisDavid HylandAinda não há avaliações
- Fever With Rash SeminarDocumento98 páginasFever With Rash SeminarSYAZRIANA SUHAIMIAinda não há avaliações
- Day 1 BacteriaDocumento251 páginasDay 1 BacteriaLisa NetherlandAinda não há avaliações
- Dracunculus MedinensisDocumento1 páginaDracunculus MedinensisEm KayAinda não há avaliações
- MKSAP13 Infectious DiseasesDocumento75 páginasMKSAP13 Infectious DiseasesDr Sumant Sharma100% (3)
- SpirochaetesDocumento31 páginasSpirochaetesblue_blooded23Ainda não há avaliações
- DiphteriaDocumento64 páginasDiphteriaOmarAinda não há avaliações
- Id ModuleDocumento4 páginasId ModuleKumar AdityaAinda não há avaliações
- Microbiology (Notes From Uworld)Documento2 páginasMicrobiology (Notes From Uworld)Nanda MinndinAinda não há avaliações
- PyomeningitisDocumento54 páginasPyomeningitisRiya BagdiAinda não há avaliações
- Blood and Tissue ProtozoaDocumento32 páginasBlood and Tissue ProtozoaFort SalvadorAinda não há avaliações
- Central Nervous System Infections: Gonzalo B. Roman JR.,MD.,FPSPDocumento72 páginasCentral Nervous System Infections: Gonzalo B. Roman JR.,MD.,FPSPBenjamin PrabhuAinda não há avaliações
- CNS InfectionDocumento10 páginasCNS InfectionShunqing ZhangAinda não há avaliações
- Systemic Lupus Erythematosus (SLE)Documento39 páginasSystemic Lupus Erythematosus (SLE)Nadya SabrinaAinda não há avaliações
- Anti-Fungal DrugsDocumento2 páginasAnti-Fungal Drugssarguss14Ainda não há avaliações
- @PIDs Curs 200903Documento43 páginas@PIDs Curs 200903Mohammad_Islam87Ainda não há avaliações
- 1.acute Respiratory Disease: DDX: Kawasaki, Strep. InfectionDocumento5 páginas1.acute Respiratory Disease: DDX: Kawasaki, Strep. InfectionSheryl Layne Lao-SebrioAinda não há avaliações
- PediatricsDocumento31 páginasPediatricsLuai Tuma KhouryAinda não há avaliações
- Infections in Pregnancy FinalDocumento67 páginasInfections in Pregnancy FinalkashafAinda não há avaliações
- Pertusis TreatmentDocumento20 páginasPertusis TreatmentJaipratap SinghAinda não há avaliações
- Gilut Herpes ZosteRDocumento24 páginasGilut Herpes ZosteRdimasahadiantoAinda não há avaliações
- Harrisons: Introduction To Infectious DiseasesDocumento3 páginasHarrisons: Introduction To Infectious Diseasesapi-3704562Ainda não há avaliações
- Malassezia Furfur An-An Ap-Ap Naturally Found On The SkinDocumento48 páginasMalassezia Furfur An-An Ap-Ap Naturally Found On The SkinNikki ValerioAinda não há avaliações
- Enterovirus & PoliomyelitisDocumento17 páginasEnterovirus & PoliomyelitisAbdulsalam HashiAinda não há avaliações
- Differential Diagnosis Fever With RashDocumento15 páginasDifferential Diagnosis Fever With RashJeetat OngAinda não há avaliações
- Tyhpoid FeverDocumento6 páginasTyhpoid FeverMade Oka Heryana100% (1)
- Skin PathologyDocumento3 páginasSkin Pathologychrisp7Ainda não há avaliações
- SketchyDocumento3 páginasSketchybellAinda não há avaliações
- Mycoviro Fungal Agent of DiseasesDocumento6 páginasMycoviro Fungal Agent of DiseasesShanAinda não há avaliações
- Nri1201 Hiv Poster PDFDocumento1 páginaNri1201 Hiv Poster PDFalfredoibc100% (1)
- CMV VirusDocumento8 páginasCMV VirusKalpavriksha1974Ainda não há avaliações
- Opportunistic Infections PDFDocumento88 páginasOpportunistic Infections PDFironbuang100% (1)
- Chlamydiae: Dr. Aye Mi San Assistant LecturerDocumento32 páginasChlamydiae: Dr. Aye Mi San Assistant LecturerNaing Lin SoeAinda não há avaliações
- Bates Chapter 8 Lung and ThoraxDocumento15 páginasBates Chapter 8 Lung and ThoraxAdrian CaballesAinda não há avaliações
- Opportunistic Amoeba Facultative ParasitesDocumento25 páginasOpportunistic Amoeba Facultative ParasitesLizeth Querubin100% (10)
- DR Solis - Midterms - Preventive Pediatrics 1&2 & HandoutsDocumento12 páginasDR Solis - Midterms - Preventive Pediatrics 1&2 & HandoutschristianAinda não há avaliações
- Edwards Down SyndromeDocumento5 páginasEdwards Down Syndromeapi-346355246Ainda não há avaliações
- Medication ChartDocumento4 páginasMedication ChartShanon BelleAinda não há avaliações
- Study Notes Respiratory SystemDocumento19 páginasStudy Notes Respiratory SystemAnde Mangkuluhur Azhari ThalibbanAinda não há avaliações
- MictobiologyDocumento26 páginasMictobiologySaransh GhimireAinda não há avaliações
- TogaviridaeDocumento60 páginasTogaviridae2013SecB50% (2)
- Treatment and Prognosis of Common Variable ImmunodeficiencyDocumento11 páginasTreatment and Prognosis of Common Variable ImmunodeficiencyJoaoAinda não há avaliações
- Mycobacterium Tuberculosis and Tuberculosis - TodarDocumento18 páginasMycobacterium Tuberculosis and Tuberculosis - TodarTanti Dewi WulantikaAinda não há avaliações
- Deepshikha Chhetri Msc. FSNDocumento50 páginasDeepshikha Chhetri Msc. FSNDaiane SantanaAinda não há avaliações
- Unit 2 - Physiological Reaction To InjuryDocumento90 páginasUnit 2 - Physiological Reaction To InjuryFabian Chapima100% (1)
- Gram Negative SpirochetesDocumento50 páginasGram Negative SpirochetesYeshiwas FelekeAinda não há avaliações
- Bacterial InfectionDocumento41 páginasBacterial InfectionUmmi Rinandari100% (1)
- Materi 5Documento15 páginasMateri 5navytiaraAinda não há avaliações
- Surgery Papillary Thyroid CADocumento15 páginasSurgery Papillary Thyroid CAMelissa LabadorAinda não há avaliações
- Cestode SDocumento38 páginasCestode SJang JangAinda não há avaliações
- Polycystic Kidneys: Adult PKD: ComplicationsDocumento1 páginaPolycystic Kidneys: Adult PKD: ComplicationsUsman Ali AkbarAinda não há avaliações
- Urinary Tract Infection & PyelonephritisDocumento3 páginasUrinary Tract Infection & PyelonephritisUsman Ali AkbarAinda não há avaliações
- Renal Tubular Acidosis Summary - AdjDocumento1 páginaRenal Tubular Acidosis Summary - AdjUsman Ali AkbarAinda não há avaliações
- Chronic Renal Failure: Concise Long Case ApproachDocumento3 páginasChronic Renal Failure: Concise Long Case ApproachUsman Ali AkbarAinda não há avaliações
- DialysisDocumento2 páginasDialysisUsman Ali AkbarAinda não há avaliações
- Obstructive Airway Disease: Dr. Khalid Al-Mobaireek King Khalid University HospitalDocumento53 páginasObstructive Airway Disease: Dr. Khalid Al-Mobaireek King Khalid University HospitalUsman Ali AkbarAinda não há avaliações
- GI Bleeding Team Work - 2nd EditionDocumento9 páginasGI Bleeding Team Work - 2nd EditionUsman Ali AkbarAinda não há avaliações
- Recurrent VomitingDocumento16 páginasRecurrent VomitingUsman Ali AkbarAinda não há avaliações
- DR Othman Alharbi, MBBS FRCPC Assistance Professor & Consultant Gastroenterology College of Medicine King Saud UniversityDocumento18 páginasDR Othman Alharbi, MBBS FRCPC Assistance Professor & Consultant Gastroenterology College of Medicine King Saud UniversityUsman Ali AkbarAinda não há avaliações
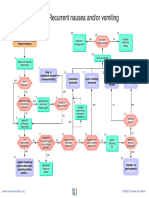
- Recurrent Nausea Andor VomitingDocumento8 páginasRecurrent Nausea Andor VomitingUsman Ali AkbarAinda não há avaliações
- Untold Stanza... : - Nasim Alam (N-61)Documento1 páginaUntold Stanza... : - Nasim Alam (N-61)Usman Ali AkbarAinda não há avaliações
- King Khalid University Hospital Department of Obstetrics & Gyncology Course 481Documento40 páginasKing Khalid University Hospital Department of Obstetrics & Gyncology Course 481Usman Ali AkbarAinda não há avaliações
- Anaemia in PregnancyDocumento13 páginasAnaemia in PregnancyUsman Ali AkbarAinda não há avaliações
- Cord ProlapseDocumento2 páginasCord ProlapseUsman Ali AkbarAinda não há avaliações
- Organophosphate PoisoningDocumento23 páginasOrganophosphate PoisoningUsman Ali AkbarAinda não há avaliações
- Through The Strange WindsDocumento5 páginasThrough The Strange WindsUsman Ali AkbarAinda não há avaliações
- Alas!! EmpytinessDocumento2 páginasAlas!! EmpytinessUsman Ali AkbarAinda não há avaliações
- Subject: Permission For Badminton Court NID, Multan: TH THDocumento1 páginaSubject: Permission For Badminton Court NID, Multan: TH THUsman Ali AkbarAinda não há avaliações
- GRAM NEGATIVE RODS (5) Fastidious Organisms From Animal Sources (A)Documento1 páginaGRAM NEGATIVE RODS (5) Fastidious Organisms From Animal Sources (A)Usman Ali AkbarAinda não há avaliações
- Lect 1:: M2Pasysl21 Urinary SystemDocumento4 páginasLect 1:: M2Pasysl21 Urinary SystemUsman Ali AkbarAinda não há avaliações
- Death and The Mother For MergeDocumento4 páginasDeath and The Mother For MergeUsman Ali AkbarAinda não há avaliações
- When Hope DiesDocumento2 páginasWhen Hope DiesUsman Ali AkbarAinda não há avaliações
- Urinary Incontinence Following Gynaecological SurgeryDocumento6 páginasUrinary Incontinence Following Gynaecological SurgeryDwickyAinda não há avaliações
- Cambridge International General Certificate of Secondary EducationDocumento9 páginasCambridge International General Certificate of Secondary EducationUkauka UkaukaAinda não há avaliações
- The Tonsils (Waldeyer's Ring) - Lingual - Pharyngeal - Palatine - Tubal - TeachMeAnatomyDocumento4 páginasThe Tonsils (Waldeyer's Ring) - Lingual - Pharyngeal - Palatine - Tubal - TeachMeAnatomywachito ricoAinda não há avaliações
- Sex and Sexual FunctionDocumento9 páginasSex and Sexual FunctionimanolkioAinda não há avaliações
- ClearStart Quick Start InstructionsDocumento3 páginasClearStart Quick Start InstructionsHisWellness100% (1)
- What Is Dairy RanchingDocumento3 páginasWhat Is Dairy RanchingBright SamuelAinda não há avaliações
- Early Journal Content On JSTOR, Free To Anyone in The WorldDocumento6 páginasEarly Journal Content On JSTOR, Free To Anyone in The Worldnopal10Ainda não há avaliações
- I. Review of Respiratory System A.ppt 2Documento115 páginasI. Review of Respiratory System A.ppt 2arielleortuosteAinda não há avaliações
- About HyenaDocumento24 páginasAbout HyenaRiswan Hanafyah Harahap0% (1)
- Trilemma Adventures BestiaryDocumento17 páginasTrilemma Adventures BestiaryZamak50% (2)
- BeekeepingDocumento17 páginasBeekeepingApollon Phebo0% (1)
- Model Test One Structure and Written ExpressionDocumento10 páginasModel Test One Structure and Written ExpressionEka KurniatiAinda não há avaliações
- NEET 2017 Syllabus CoreDocumento4 páginasNEET 2017 Syllabus CoreusavelAinda não há avaliações
- Milia AriaDocumento8 páginasMilia AriaAtsabitFarisAinda não há avaliações
- Trial SPM SBP 2010 Biology Marking SchemeDocumento24 páginasTrial SPM SBP 2010 Biology Marking SchemeMr.D-SIM100% (6)
- Comparison of The YMCA Cycle SubDocumento2 páginasComparison of The YMCA Cycle SubBryan Allen Q. ValleAinda não há avaliações
- Tutorial 1.1 - Measuring Disease Occurence (Morbidity) - Students - UpdateDocumento3 páginasTutorial 1.1 - Measuring Disease Occurence (Morbidity) - Students - UpdateFebriansyah 'ebhi'100% (1)
- Herpes Antidote UnlockedDocumento125 páginasHerpes Antidote Unlockedfcuevaspr180% (5)
- Sexual SelfDocumento19 páginasSexual SelfErica SisgonAinda não há avaliações
- Lacunar Infarct - Radiology Reference Article - RadiopaediaDocumento8 páginasLacunar Infarct - Radiology Reference Article - RadiopaediaRismanto TorsioAinda não há avaliações
- BetaStar 1206Documento2 páginasBetaStar 1206api-3697331Ainda não há avaliações
- 5a - Osteology of Thorax - Intercostal SpacesDocumento68 páginas5a - Osteology of Thorax - Intercostal SpacesINTERNET MONEY HACKAinda não há avaliações
- Piis0894731715003879 PDFDocumento49 páginasPiis0894731715003879 PDFDuoc Kien VangAinda não há avaliações
- Dairy FarmingDocumento1 páginaDairy FarmingyogasanaAinda não há avaliações
- Parasitic Disease (Scabies)Documento13 páginasParasitic Disease (Scabies)Brijesh Singh YadavAinda não há avaliações
- Sunita BhoiteDocumento8 páginasSunita Bhoiteprajakta kuralkarAinda não há avaliações
- OlfactionDocumento12 páginasOlfactionbakex645Ainda não há avaliações
- Sterek - A Mating MoonDocumento79 páginasSterek - A Mating MoonPaola GarciaAinda não há avaliações
- Parasite Identification Slides v2.0Documento25 páginasParasite Identification Slides v2.0Sam Petruda100% (3)
- Gas Exchange in Humans (Multiple Choice) QP PDFDocumento12 páginasGas Exchange in Humans (Multiple Choice) QP PDFSyakir Fahmie100% (2)
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNo EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineAinda não há avaliações
- The Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsNo EverandThe Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsNota: 4.5 de 5 estrelas4.5/5 (6)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisNo EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisNota: 4 de 5 estrelas4/5 (9)
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicNo EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicAinda não há avaliações
- The Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthNo EverandThe Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthAinda não há avaliações
- Fatal Conveniences: The Toxic Products and Harmful Habits That Are Making You Sick—and the Simple Changes That Will Save Your HealthNo EverandFatal Conveniences: The Toxic Products and Harmful Habits That Are Making You Sick—and the Simple Changes That Will Save Your HealthNota: 4 de 5 estrelas4/5 (7)
- There Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceNo EverandThere Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceNota: 4.5 de 5 estrelas4.5/5 (15)
- The Truth about Wuhan: How I Uncovered the Biggest Lie in HistoryNo EverandThe Truth about Wuhan: How I Uncovered the Biggest Lie in HistoryNota: 4 de 5 estrelas4/5 (6)
- Sickening: How Big Pharma Broke American Health Care and How We Can Repair ItNo EverandSickening: How Big Pharma Broke American Health Care and How We Can Repair ItNota: 4 de 5 estrelas4/5 (9)
- The Hair Color Mix Book: More Than 150 Recipes for Salon-Perfect Color at HomeNo EverandThe Hair Color Mix Book: More Than 150 Recipes for Salon-Perfect Color at HomeNota: 3.5 de 5 estrelas3.5/5 (7)
- The Inescapable Immune Escape PandemicNo EverandThe Inescapable Immune Escape PandemicNota: 5 de 5 estrelas5/5 (1)
- Epidemics and Society: From the Black Death to the PresentNo EverandEpidemics and Society: From the Black Death to the PresentNota: 4.5 de 5 estrelas4.5/5 (9)
- Vaccines Did Not Cause Rachel's Autism: My Journey as a Vaccine Scientist, Pediatrician, and Autism DadNo EverandVaccines Did Not Cause Rachel's Autism: My Journey as a Vaccine Scientist, Pediatrician, and Autism DadNota: 4.5 de 5 estrelas4.5/5 (3)
- Profiles of the Vaccine-Injured: "A Lifetime Price to Pay"No EverandProfiles of the Vaccine-Injured: "A Lifetime Price to Pay"Nota: 3.5 de 5 estrelas3.5/5 (3)
- War on Ivermectin: The Medicine that Saved Millions and Could Have Ended the PandemicNo EverandWar on Ivermectin: The Medicine that Saved Millions and Could Have Ended the PandemicNota: 4 de 5 estrelas4/5 (7)
- Make America Healthy Again: How Bad Behavior and Big Government Caused a Trillion-Dollar CrisisNo EverandMake America Healthy Again: How Bad Behavior and Big Government Caused a Trillion-Dollar CrisisAinda não há avaliações
- Summary: The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health by Robert F. Kennedy Jr: Key Takeaways, Summary & Analysis IncludedNo EverandSummary: The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health by Robert F. Kennedy Jr: Key Takeaways, Summary & Analysis IncludedAinda não há avaliações
- Environmental Health and Occupational Health & SafetyNo EverandEnvironmental Health and Occupational Health & SafetyNota: 3.5 de 5 estrelas3.5/5 (9)
- Community-Acquired Pneumonia: Strategies for ManagementNo EverandCommunity-Acquired Pneumonia: Strategies for ManagementAntoni TorresNota: 4.5 de 5 estrelas4.5/5 (2)
- The Wuhan Cover-Up: And the Terrifying Bioweapons Arms RaceNo EverandThe Wuhan Cover-Up: And the Terrifying Bioweapons Arms RaceAinda não há avaliações
- The Atlas of Disease: Mapping Deadly Epidemics and Contagion from the Plague to the CoronavirusNo EverandThe Atlas of Disease: Mapping Deadly Epidemics and Contagion from the Plague to the CoronavirusNota: 4.5 de 5 estrelas4.5/5 (10)
- "Cause Unknown": The Epidemic of Sudden Deaths in 2021 & 2022No Everand"Cause Unknown": The Epidemic of Sudden Deaths in 2021 & 2022Nota: 4.5 de 5 estrelas4.5/5 (19)
- Clean: Overcoming Addiction and Ending America’s Greatest TragedyNo EverandClean: Overcoming Addiction and Ending America’s Greatest TragedyNota: 4 de 5 estrelas4/5 (18)