Você também pode gostar
- Health Management in The Oil and Gas IndustryDocumento44 páginasHealth Management in The Oil and Gas IndustryClaudia TiradoAinda não há avaliações
- WSH Guidelines Statutory Medical Examinations 2013Documento210 páginasWSH Guidelines Statutory Medical Examinations 2013OnaFajardoAinda não há avaliações
- Certified Health And Safety Consultant A Complete Guide - 2020 EditionNo EverandCertified Health And Safety Consultant A Complete Guide - 2020 EditionAinda não há avaliações
- Health Risk Assessment and ManagementDocumento36 páginasHealth Risk Assessment and ManagementChandra PriyandikaAinda não há avaliações
- Building A Safety Culture A Complete Guide - 2020 EditionNo EverandBuilding A Safety Culture A Complete Guide - 2020 EditionAinda não há avaliações
- Ipieca Iogp Medical Emergency Response and Primary Healthcare GuidelineDocumento64 páginasIpieca Iogp Medical Emergency Response and Primary Healthcare GuidelineIman MaanaiyaAinda não há avaliações
- Health, Safety, and Environmental Management in Offshore and Petroleum EngineeringNo EverandHealth, Safety, and Environmental Management in Offshore and Petroleum EngineeringNota: 5 de 5 estrelas5/5 (1)
- Hazardous Substances and Human Health: Exposure, Impact and External Cost Assessment at the European ScaleNo EverandHazardous Substances and Human Health: Exposure, Impact and External Cost Assessment at the European ScaleAinda não há avaliações
- Threat And Risk Assessment A Complete Guide - 2020 EditionNo EverandThreat And Risk Assessment A Complete Guide - 2020 EditionAinda não há avaliações
- culture of safety A Complete Guide - 2019 EditionNo Everandculture of safety A Complete Guide - 2019 EditionNota: 5 de 5 estrelas5/5 (1)
- Safety in the Chemical Laboratory and Industry: A Practical GuideNo EverandSafety in the Chemical Laboratory and Industry: A Practical GuideAinda não há avaliações
- Safety Alert - Elevating Work Platform Fatal AccidentDocumento2 páginasSafety Alert - Elevating Work Platform Fatal AccidentNirmalkumarAinda não há avaliações
- Membership ApplicationDocumento4 páginasMembership ApplicationGabrielAinda não há avaliações
- Permit To Work GuidelinesDocumento12 páginasPermit To Work GuidelinesalanjcherryAinda não há avaliações
- Comparison Auditor OHSAS 18001 IRCA SMK3Documento5 páginasComparison Auditor OHSAS 18001 IRCA SMK3Ricky ARIEF100% (1)
- L 21 The Management of Health & Safety at Work Regulations 1999Documento54 páginasL 21 The Management of Health & Safety at Work Regulations 19991DSBAinda não há avaliações
- CEP2010 Heat TransferDocumento8 páginasCEP2010 Heat TransferamsukdAinda não há avaliações
- 1ngc Guide Nov 14 Spec v622112017511437Documento69 páginas1ngc Guide Nov 14 Spec v622112017511437khalidAinda não há avaliações
- Movile Plataform IncidentDocumento34 páginasMovile Plataform IncidentAnonymous GfPSYi4nAinda não há avaliações
- Greenwich Health & Safety Induction OverviewDocumento27 páginasGreenwich Health & Safety Induction OverviewMin ingAinda não há avaliações
- LUS-HSE-WG3-446-004.03 - Incident Reporting & InvestigationDocumento13 páginasLUS-HSE-WG3-446-004.03 - Incident Reporting & InvestigationamalAinda não há avaliações
- First Aid Program OSHA Compliant From GDIDocumento14 páginasFirst Aid Program OSHA Compliant From GDIGrant Davis100% (2)
- Road Safety Audit FindingsDocumento3 páginasRoad Safety Audit FindingsShivinder BhandariAinda não há avaliações
- Water blasting SWMSDocumento5 páginasWater blasting SWMSjohney2Ainda não há avaliações
- Major Accident Investigation - How To Plan OneDocumento12 páginasMajor Accident Investigation - How To Plan Oneamineamine67Ainda não há avaliações
- Hazard and Risk RegisterDocumento2 páginasHazard and Risk RegisterTheresa BrooksAinda não há avaliações
- GN For Contractor - BiDocumento122 páginasGN For Contractor - Bitoyakatob186Ainda não há avaliações
- Hse PlanDocumento99 páginasHse Planjayesh utekarAinda não há avaliações
- Assessment of Human Factors On Oil SpillsDocumento53 páginasAssessment of Human Factors On Oil SpillsflouzanAinda não há avaliações
- Health and Medical Monitoring Group ProcedureDocumento14 páginasHealth and Medical Monitoring Group ProcedurenickAinda não há avaliações
- Systems in Focus 0409Documento32 páginasSystems in Focus 0409ylaala8010Ainda não há avaliações
- Implementation of A QMS Within The MRF IndustryDocumento35 páginasImplementation of A QMS Within The MRF IndustryAlexis RancesAinda não há avaliações
- Unit Diploma Nebosh DniDocumento32 páginasUnit Diploma Nebosh DniScribdTranslationsAinda não há avaliações
- FAS08-111 Standard FinalDocumento12 páginasFAS08-111 Standard FinalAnn Beck100% (1)
- RKABDocumento5 páginasRKABMuhammad DailamiAinda não há avaliações
- Leading indicators for occupational health and safety in miningDocumento56 páginasLeading indicators for occupational health and safety in miningrome_n21Ainda não há avaliações
- Basic Elements of A Successful Safety and Health Program: Frank Dobson, CHSTDocumento46 páginasBasic Elements of A Successful Safety and Health Program: Frank Dobson, CHSTRoslanAinda não há avaliações
- Safety Critical Task Analysis and BowtiesDocumento6 páginasSafety Critical Task Analysis and BowtiesMuhammad ButtAinda não há avaliações
- HSEMS PresentationDocumento21 páginasHSEMS PresentationVeera RagavanAinda não há avaliações
- Examiners Report Unit D - September 2009 Unit DDocumento10 páginasExaminers Report Unit D - September 2009 Unit DЮрий СиливончикAinda não há avaliações
- Topic 4 Hazard Identification PDFDocumento15 páginasTopic 4 Hazard Identification PDFDiyana OsmanAinda não há avaliações
- Engineering Kinetics (PVT) LTD: Task Risk AssessmentDocumento3 páginasEngineering Kinetics (PVT) LTD: Task Risk AssessmentandreAinda não há avaliações
- 108 1 Participatory Vulnerability Analysis GuideDocumento35 páginas108 1 Participatory Vulnerability Analysis Guideenemas13Ainda não há avaliações
- How To Manage Whs RisksDocumento30 páginasHow To Manage Whs RisksMuStafaAbbasAinda não há avaliações
- GRI 403 - Occupational Health and Safety 2018 PresentationDocumento28 páginasGRI 403 - Occupational Health and Safety 2018 PresentationCostas JacovidesAinda não há avaliações
- Emergency Response Plan: Berrima Cement WorksDocumento44 páginasEmergency Response Plan: Berrima Cement WorksDanu HenantyoAinda não há avaliações
- Hazard Assessment For PPE - XX-DRAFTDocumento4 páginasHazard Assessment For PPE - XX-DRAFTWayne VanderhoofAinda não há avaliações
- Legal and Other Requirements Register April 45001Documento18 páginasLegal and Other Requirements Register April 45001john osullivanAinda não há avaliações
- 17 Subcon RequirementsDocumento38 páginas17 Subcon RequirementsMohammed MinhajAinda não há avaliações
- Nebosh Diploma Unit DniDocumento34 páginasNebosh Diploma Unit DniScribdTranslationsAinda não há avaliações
- N 06300 IP1038 Human Factors Competancy Assurance Rev 0 Dec 2012 PDFDocumento12 páginasN 06300 IP1038 Human Factors Competancy Assurance Rev 0 Dec 2012 PDFsubragkAinda não há avaliações
- Manua Public Health Management Chemical IncidentsDocumento101 páginasManua Public Health Management Chemical IncidentsteresaAinda não há avaliações
- Effective Safety Management SystemsDocumento34 páginasEffective Safety Management SystemsAmir SherafatipourAinda não há avaliações
- Ohsas 18001Documento27 páginasOhsas 18001tahseenhassantirmiziAinda não há avaliações
- A Guide To Malaria Management Programmes in The Oil and Gas IndustryDocumento28 páginasA Guide To Malaria Management Programmes in The Oil and Gas IndustryMaxwell C Jay KafwaniAinda não há avaliações
- Effective Safety Management Systems: by George RobothamDocumento33 páginasEffective Safety Management Systems: by George RobothamLoganathan DharmarAinda não há avaliações
- BI 10-02133, March 23 2020, SAFETY STATISTICSDocumento2 páginasBI 10-02133, March 23 2020, SAFETY STATISTICSHaleemUrRashidBangashAinda não há avaliações
- Branch of Egyptian Projects Co.: Monthly Safety Statistics For: Jan, 2020Documento1 páginaBranch of Egyptian Projects Co.: Monthly Safety Statistics For: Jan, 2020HaleemUrRashidBangashAinda não há avaliações
- 01 Safety Statistics by Haleem Ur Rashid, BI 10-02185Documento3 páginas01 Safety Statistics by Haleem Ur Rashid, BI 10-02185HaleemUrRashidBangashAinda não há avaliações
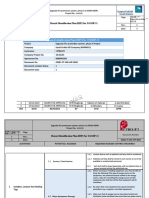
- Hazard Identification Plan (Hip) For Adgosp-2: Upgrade Fire Protection System, Phase Ii at Saoo Gosps Project No.Documento27 páginasHazard Identification Plan (Hip) For Adgosp-2: Upgrade Fire Protection System, Phase Ii at Saoo Gosps Project No.HaleemUrRashidBangashAinda não há avaliações
- Branch of Egyptian Projects Co.: Monthly Safety Statistics For: Jan, 2020Documento1 páginaBranch of Egyptian Projects Co.: Monthly Safety Statistics For: Jan, 2020HaleemUrRashidBangashAinda não há avaliações
- Hazard Identification Plan (Hip) For Adgosp-2: Upgrade Fire Protection System, Phase Ii at Saoo Gosps Project No.Documento27 páginasHazard Identification Plan (Hip) For Adgosp-2: Upgrade Fire Protection System, Phase Ii at Saoo Gosps Project No.HaleemUrRashidBangashAinda não há avaliações
- Weekly Safety Meeting Minutes & StatsDocumento3 páginasWeekly Safety Meeting Minutes & StatsHaleemUrRashidBangash100% (2)
- BI 10-02133, WEEK 06, Safety Statistics Reoport NDocumento1 páginaBI 10-02133, WEEK 06, Safety Statistics Reoport NHaleemUrRashidBangash100% (1)
- Weekly Safety Meeting Minutes & StatsDocumento3 páginasWeekly Safety Meeting Minutes & StatsHaleemUrRashidBangash100% (2)
- Weekly Safety Meeting Minutes & StatsDocumento3 páginasWeekly Safety Meeting Minutes & StatsHaleemUrRashidBangash100% (2)
- 20) Hazard Identification Plan (HIP) For UGOSP-11 29-01-2020Documento27 páginas20) Hazard Identification Plan (HIP) For UGOSP-11 29-01-2020HaleemUrRashidBangash100% (2)
- 5) Hazard Identification Plan (HIP) For SHGOSP-2 29-01-2020Documento36 páginas5) Hazard Identification Plan (HIP) For SHGOSP-2 29-01-2020HaleemUrRashidBangashAinda não há avaliações
- Hazard Identification Plan (HIP) Rev 01 For SAOO GOSPsDocumento31 páginasHazard Identification Plan (HIP) Rev 01 For SAOO GOSPsHaleemUrRashidBangashAinda não há avaliações
- Hazard Identification Plan (Hip) For Adgosp-2: Upgrade Fire Protection System, Phase Ii at Saoo Gosps Project No.Documento27 páginasHazard Identification Plan (Hip) For Adgosp-2: Upgrade Fire Protection System, Phase Ii at Saoo Gosps Project No.HaleemUrRashidBangashAinda não há avaliações
- 13) Hazard Identification Plan (HIP) For ABGOSP-3 29-01-2020Documento31 páginas13) Hazard Identification Plan (HIP) For ABGOSP-3 29-01-2020HaleemUrRashidBangashAinda não há avaliações
- 14) Hazard Identification Plan (HIP) For UGOSP-9 29-01-2020Documento31 páginas14) Hazard Identification Plan (HIP) For UGOSP-9 29-01-2020HaleemUrRashidBangash100% (1)
- Hazard Identification Plan (Hip) For Adgosp-1: Upgrade Fire Protection System, Phase Ii at Saoo Gosps Project No.Documento27 páginasHazard Identification Plan (Hip) For Adgosp-1: Upgrade Fire Protection System, Phase Ii at Saoo Gosps Project No.HaleemUrRashidBangashAinda não há avaliações
- 13) Hazard Identification Plan (HIP) For ABGOSP-3 29-01-2020Documento31 páginas13) Hazard Identification Plan (HIP) For ABGOSP-3 29-01-2020HaleemUrRashidBangashAinda não há avaliações
- 9) Hazard Identification Plan (HIP) For ABGOSP-5 29-01-2020Documento36 páginas9) Hazard Identification Plan (HIP) For ABGOSP-5 29-01-2020HaleemUrRashidBangashAinda não há avaliações
- 11) Hazard Identification Plan (HIP) For SHGOSP-5 29-01-2020Documento36 páginas11) Hazard Identification Plan (HIP) For SHGOSP-5 29-01-2020HaleemUrRashidBangashAinda não há avaliações
- 5) Hazard Identification Plan (HIP) For SHGOSP-2 29-01-2020Documento36 páginas5) Hazard Identification Plan (HIP) For SHGOSP-2 29-01-2020HaleemUrRashidBangashAinda não há avaliações
- 9) Hazard Identification Plan (HIP) For ABGOSP-5 29-01-2020Documento36 páginas9) Hazard Identification Plan (HIP) For ABGOSP-5 29-01-2020HaleemUrRashidBangashAinda não há avaliações
- 5) Hazard Identification Plan (HIP) For SHGOSP-2 29-01-2020Documento36 páginas5) Hazard Identification Plan (HIP) For SHGOSP-2 29-01-2020HaleemUrRashidBangashAinda não há avaliações
- 9) Hazard Identification Plan (HIP) For ABGOSP-5 29-01-2020Documento36 páginas9) Hazard Identification Plan (HIP) For ABGOSP-5 29-01-2020HaleemUrRashidBangashAinda não há avaliações
- 4) Hazard Identification Plan (HIP) For ADGOSP-6 29-01-2020Documento36 páginas4) Hazard Identification Plan (HIP) For ADGOSP-6 29-01-2020HaleemUrRashidBangashAinda não há avaliações
- Hazard Identification Plan (HIP) Rev 01 For SAOO GOSPsDocumento31 páginasHazard Identification Plan (HIP) Rev 01 For SAOO GOSPsHaleemUrRashidBangashAinda não há avaliações
- 9) Hazard Identification Plan (HIP) For ABGOSP-5 29-01-2020Documento36 páginas9) Hazard Identification Plan (HIP) For ABGOSP-5 29-01-2020HaleemUrRashidBangashAinda não há avaliações
- 4) Hazard Identification Plan (HIP) For ADGOSP-6 29-01-2020Documento36 páginas4) Hazard Identification Plan (HIP) For ADGOSP-6 29-01-2020HaleemUrRashidBangashAinda não há avaliações
- 9) Hazard Identification Plan (HIP) For ABGOSP-5 29-01-2020Documento36 páginas9) Hazard Identification Plan (HIP) For ABGOSP-5 29-01-2020HaleemUrRashidBangashAinda não há avaliações
- 4) Hazard Identification Plan (HIP) For ADGOSP-6 29-01-2020Documento36 páginas4) Hazard Identification Plan (HIP) For ADGOSP-6 29-01-2020HaleemUrRashidBangashAinda não há avaliações
- Unemployment QuestionnaireDocumento4 páginasUnemployment QuestionnaireAnonymous 2gGScOaS7100% (5)
- Work Order Plastering ProjectDocumento9 páginasWork Order Plastering ProjectOm Krish Ram100% (1)
- Researching About Yourself: Lesson IiDocumento8 páginasResearching About Yourself: Lesson IiKey Cylyn JalaAinda não há avaliações
- Stonehill Corp Officers Cannot Challenge Search of Corporate OfficesDocumento63 páginasStonehill Corp Officers Cannot Challenge Search of Corporate OfficesLexa ClarkeAinda não há avaliações
- Insurance Need AnalysisDocumento8 páginasInsurance Need AnalysisRajesh Chowdary ChintamaneniAinda não há avaliações
- Integrated Contextual ModelDocumento23 páginasIntegrated Contextual ModelSahana Sameer Kulkarni0% (1)
- Conflict ManagementDocumento16 páginasConflict ManagementBisrat DaAinda não há avaliações
- MGT201 Chapter 13Documento32 páginasMGT201 Chapter 13natchy18Ainda não há avaliações
- Ricardo Semler - Maverick - SummaryDocumento9 páginasRicardo Semler - Maverick - SummaryHasanErkelAinda não há avaliações
- Why Study at International Nurse TrainingDocumento6 páginasWhy Study at International Nurse TrainingjpanayAinda não há avaliações
- Vacancy Announcement - Project Coordinator, Governance at Janwani, MCCIA PuneDocumento4 páginasVacancy Announcement - Project Coordinator, Governance at Janwani, MCCIA PunenaimkeruwalaAinda não há avaliações
- Manual Handling Mini EbookDocumento15 páginasManual Handling Mini EbookJohnPaulBascoAinda não há avaliações
- A Technical Report Work On Siwes UndertaDocumento70 páginasA Technical Report Work On Siwes UndertaAbdullahi AwwalAinda não há avaliações
- 2020 Assignment 2Documento6 páginas2020 Assignment 2mohamedAinda não há avaliações
- FNB Pension Fund Irp5Documento1 páginaFNB Pension Fund Irp5Vovo SolutionsAinda não há avaliações
- Cash Receipts Process Flowchart: Receives Payment Receive Bank Statement andDocumento11 páginasCash Receipts Process Flowchart: Receives Payment Receive Bank Statement andLara Camille CelestialAinda não há avaliações
- RA RESPIRATORYTHERAPIST MANILA Sep2018 PDFDocumento24 páginasRA RESPIRATORYTHERAPIST MANILA Sep2018 PDFPhilBoardResultsAinda não há avaliações
- Fox S Frames of ReferenceDocumento10 páginasFox S Frames of ReferenceMilanSimkhadaAinda não há avaliações
- Child Labor PPT 1Documento9 páginasChild Labor PPT 1Moiz KhanAinda não há avaliações
- Marlow Navigation vs. CabatayDocumento9 páginasMarlow Navigation vs. CabatayAlvin Halcon100% (1)
- ANC Manifesto 2019Documento68 páginasANC Manifesto 2019Mail and GuardianAinda não há avaliações
- 1277 1 PDFDocumento1 página1277 1 PDFFritz G.E.Ainda não há avaliações
- Flexible Budget and Variances Practice Questions 3Documento364 páginasFlexible Budget and Variances Practice Questions 3Saram NadeemAinda não há avaliações
- Rumki PDFDocumento41 páginasRumki PDFShelveyElmoDiasAinda não há avaliações
- HRM in InfosysDocumento11 páginasHRM in Infosysguptarahul27550% (4)
- (Research Paper) Hossein Esmaeil KhorsandDocumento287 páginas(Research Paper) Hossein Esmaeil KhorsandMadiha DashAinda não há avaliações
- Critical Review of Performance Management System at Telenor PakistanDocumento7 páginasCritical Review of Performance Management System at Telenor PakistanFaisal Ahmad Jafri0% (1)
- Environmental Analysis Siemens Ltd-IndiaDocumento15 páginasEnvironmental Analysis Siemens Ltd-Indiacatchrekhacool100% (1)
- Wal-Mart's Computerized Scheduling Raises Ethical DilemmasDocumento8 páginasWal-Mart's Computerized Scheduling Raises Ethical DilemmasAnwar RabiaAinda não há avaliações
- Report of The Special Group On Targeting Ten Million Employment Opportunities Per Year Over The Tenth Plan PeriodDocumento180 páginasReport of The Special Group On Targeting Ten Million Employment Opportunities Per Year Over The Tenth Plan PerioddeputykrishanAinda não há avaliações