news and views
Akt2 relaxes podocytes in chronic kidney disease
Jochen Reiser
npg
2013 Nature America, Inc. All rights reserved.
A signaling cascade is activated in podocytes to induce survival and cope with stress during advanced glomerular
disease, a new study shows. The findings may also explain why the immunosuppressor sirolimus, an inhibitor of this
pathway, can cause proteinuria in a subset of patients with chronic kidney disease (pages 12881296).
The loss of proteins into the urine, or proteinuria, often occurs at early stages of chronic
kidney disease (CKD), a condition that affects
about 500 million people worldwide, and this
loss is a driver of both morbidity and mortality. Kidney podocytes are the gatekeepers in
renal ultrafiltration, ensuring that proteins
larger than albumin are essentially kept in
the circulation and solutes and other aqueous products are being routed for excretion
in the urine. Proteinuria occurs upon damage to podocytes that results in simplification
of their foot processes, a term called effacement, which, if not reversed, can lead to loss
of podocytes through detachment, necrosis
and apoptosis1. After loss of a critical number of podocytes, progression of renal disease
ensues with an increase in serum creatinine
and loss of functional nephrons, which poses
an additional overload in the remaining
kidney cells, causing metabolic and mechanical stress and finally leading to their death. To
date, effective therapies that completely halt
or reverse the pathological changes resulting from advanced proteinuria and podocyte
injury are still lacking.
In this issue of Nature Medicine, Canaud et al.2
found a crucial role for mammalian target of
rapamycin (mTOR) and the downstream target
Akt2 in the maintenance of podocytes during
advanced glomerular diseases. The authors
identify a counterbalancing pathway in podocytes that becomes operational as kidney cell
mass is progressively lost (Fig. 1). In particular, activation of the kinase Akt2 by mTORC2
is essential for podocytes to cope with stress
and survive in patients with severe nephron
reduction. Mechanistically, Akt2 reduces the
activity of the small GTPase Rac-1, whose
overactivation is associated with the onset of
podocyte foot process effacement3,4. As prolonged treatment with the immunosuppressor sirolimus (an mTOR inhibitor) seems to
inhibit both mTOR complexes (mTORC1 and
mTORC2)5,6, the findings have clinical implications for human CKD, as sirolimus can cause
podocyte injury and proteinuria in individuals
Jochen Reiser is at the Department of Medicine,
Rush University, Chicago, Illinois, USA.
e-mail: jochen_reiser@rush.edu
1212
with reduced nephron mass, but not in patients
with preserved renal function.
Podocytes are key elements of the filtration
apparatus, and their function depends on prosurvival signals that include phosphoinositide 3-kinasedependent Akt signaling7; the
molecular pathways that counteract the stress
imposed upon injury of the failing kidney filter,
however, are largely unknown. In an analysis
of human kidney biopsies from patients with
different types of CKD, the authors found
that Akt2 was mainly expressed in podocytes,
whereas Akt1 was predominant in tubules2.
By combining experimental mouse models of nephron reduction with genetic deletion of Akt1, Akt2 and Rictor (as a surrogate
of mTORC2 deletion), they showed that Akt2,
but not Akt1, has a pivotal role in podocyte
adaptation under increased workload caused
by nephron reduction2. Inactivation of Akt-2
mediated signaling resulted in podocyte apoptosis and foot process effacement after both
experimental and aging-induced nephron
reduction, leading to severe proteinuria and
glomerulosclerosis in these mice. Podocytes
of mice lacking Akt2 displayed cytoskeleton
changes owing to increased signaling by Rac1
(ref. 2), whose activity can be in part regulated
by Akt2 (ref. 8). Although mice with podocytespecific inactivation of Rictor also showed
reduced levels of Akt2 phosphorylation and
podocyte foot process effacement, they had
only mild proteinuria, which suggests a compensatory effect, possibly through Raptor.
Overall, these findings indicate that phosphorylation of Akt2 at Ser473 confers protection
during nephron loss by promoting podocyte
survival and cytoskeleton integrity, which are
necessary for their function.
Canaud et al.2 found that disruption of this
adaptive pathway via sirolimus caused glomerular lesions and albuminuria only in kidneytransplanted patients with severe nephron
reduction, possibly explaining the often heavy
proteinuria found in these patients treated with
this agent9. Therefore, mTOR inhibitors, such
as sirolimus, should be used with caution in
patients with nephron reduction, to preserve
the activity of the mTORC2-Akt2 axis and
prevent podocyte apoptosis. Staining of Akt2
can be used to differentiate inactive and active
forms on renal biopsies and can potentially be
developed as a prognostic marker, and Akt2
could be used as a therapeutic target to maintain glomerular functions during chronic renal
disease. The results of the study by Canaud
etal.2 are truly exciting and provide an intriguing hypothesis on the involvement of mTORC2
in sirolimus-induced proteinuria by identifying
a protective role for Akt2.
In addition to characterizing kidney biopsy
samples from patients who had received transplants, the authors investigated AKT2 status in
samples from patients with CKD and reduced
estimated glomerular filtration rates, in which
they also showed marked AKT phosphorylation
in podocytes. However, the data should be interpreted with caution, as the chronic pathological
changes that occur during CKD in nontransplanted kidneys are very different from those
observed in kidney transplant recipients, and
as such may not be the right model of nephron
loss. Furthermore, many variables, other than
immunosuppression, such as donor criteria,
ischemia times and hemodynamic aspects of
the kidney graft, could influence AKT2 signaling, directly or indirectly, even though the
authors tried to control for most of them. The
quantification of signaling pathways in kidney
biopsy samples can also be cumbersome, and an
involvement for mTORC1 in sirolimus-induced
proteinuria should not be ruled out, despite the
lack of downstream signals in the study2 and in
previous work, as it could also contribute to the
homeostasis of a damaged kidney by inducing
cell growth and proliferation.
Although Canaud et al.2 experimentally demonstrated the need for Akt2 and
mTORC2 in podocyte stress function, the lack
of mTORC1 in podocytes also causes severe
sclerosis even in otherwise normal mice, which
was aggravated when mTORC2 was concomitantly inactivated10. The study by Canaud
et al.2 suggests a linear connection between
sirolimus, the mTORC2-Akt2 axis in podocyte,
and disease and proteinuria; however, the data
from podocyte-specific mTORC2 deletion
seem to differ with respect to the onset, timing
and severity of histological lesions, as well as
with respect to proteinuria from the podocytespecific Akt2 deletion2. Until the role of
mTORC1 is clarified in this setting, we should
volume 19 | number 10 | OCTOBER 2013 nature medicine
news and views
Healthy kidney
Nephron reduction
(CKD)
Sirolimus treatment
during CKD
Podocyte
Overload
mTORC1
mTORC2
mTORC2
mTORC1
Marina Corral Spence
2013 Nature America, Inc. All rights reserved.
Akt2
npg
Sirolimus
Akt2 P
mTORC2
Akt2
Rac1
Rac-1
Rac-1
Podocyte survival
and function
Accelerated proteinuria
and podocyte stress
adaptation
Proteinuria
Normal renal
function
Retardation of CKD
Progression of
CKD and
renal failure
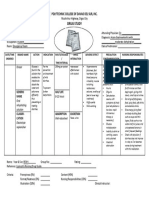
Figure 1 Podocyte function under conditions of nephron reduction. In healthy kidney, podocyte
numbers are stable and no proteinuria occurs (left). Under this condition, mTORC1 and mTORC2
activities are not upregulated, and Akt2 and podocyte Rac-1 activities remain low, which is typically
the case in healthy kidneys. Canaud et al.2 show that upon nephron reduction (middle), such as in
CKD, podocytes are adapting to the stress of cell loss and undergo mTORC2-mediated phosphorylation
of AKT2, which in turn downregulates Rac-1 activity, delaying kidney disease progression. However,
this adaptive response is abrogated by treatment with the immunosuppressor sirolimus, an mTOR
inhibitor that blocks mTORC1 and mTORC2 and that is widely used in transplantation (right). This
triggers a signaling blockade that aggravates proteinuria and nephron loss, which possibly explains
why patients with already established kidney disease treated with sirolimus can develop proteinuria
and renal failure.
keep in mind that mTORC2 activation may not
be the only player in podocyte protection, and
although the clinical effects of sirolimus on the
mTORC2-Akt2 axis are substantial, this drug is
mainly known as an inhibitor of mTORC1.
Despite these open questions, Canaud et al.2
not only shed light into the mechanism of a
drug widely used in transplantation but also
suggest that podocyte protection is possible by
directly targeting the podocytes function via
nature medicine volume 19 | number 10 | OCTOBER 2013
stabilization of Akt2 signaling, which limits
Rac1 activation, an early step in dysregulation of podocytes causing effacement and
proteinuria11. Because restoring the normal
podocyte structure and lowering proteinuria
increases podocyte survival12, it will be interesting to see whether early events damaging
podocytes in kidneys with normal renal mass
will also lead to the activation of Akt2 signals, or whether the oncoming Akt2 signal is
truly the last attempt for an otherwise dying
podocyte to counterbalance deleterious renal
effects. The US National Institute of Diabetes
and Digestive and Kidney Diseases (NIDDK)
has recently solicited applications to establish a large cohort of patients with primary
glomerular disease. The development of biomarkers such as Akt2 phosphorylation in renal
tissue is an example of going beyond renal
biopsy as the standard means of establishing
clinical diagnosis and prognosis toward the
development of new molecular diagnostic
tools for CKD.
COMPETING FINANCIAL INTERESTS
The author declares competing financial interests:
details are available in the online version of the paper
(doi:10.1038/nm.3357).
1. Reiser, J. & Sever, S. Annu. Rev. Med. 64, 357366
(2013).
2. Canaud, G. et al. Nat. Med. 19, 12881296 (2013).
3. Wei, C. et al. Nat. Med. 14, 5563 (2008).
4. Nagase, M. & Fujita, T. Nat. Rev. Nephrol. 9, 8698
(2013).
5. Sarbassov, D.D. et al. Mol. Cell 22, 159168
(2006).
6. Laplante, M. & Sabatini, D.M. Cell 149, 274293
(2012).
7. Huber, T.B. et al. Mol. Cell Biol. 23, 49174928
(2003).
8. Nozaki, S. et al. Cell Signal. 25, 13611371
(2013).
9. Diekmann, F. et al. Transplant. Rev. (Orlando) 26,
2729 (2012).
10. Gdel, M. et al. J. Clin. Invest. 121, 21972209
(2011).
11. Kistler, A.D. et al. Kidney Int. 81, 10531055
(2012).
12. Yaddanapudi, S. et al. J. Clin. Invest. 121, 39653980
(2011).
1213
Você também pode gostar
- tmpCE8C TMPDocumento19 páginastmpCE8C TMPFrontiersAinda não há avaliações
- tmpEFCC TMPDocumento6 páginastmpEFCC TMPFrontiersAinda não há avaliações
- Tmp1a96 TMPDocumento80 páginasTmp1a96 TMPFrontiersAinda não há avaliações
- tmp6F0E TMPDocumento12 páginastmp6F0E TMPFrontiersAinda não há avaliações
- tmpF178 TMPDocumento15 páginastmpF178 TMPFrontiersAinda não há avaliações
- tmp80F6 TMPDocumento24 páginastmp80F6 TMPFrontiersAinda não há avaliações
- tmp3CAB TMPDocumento16 páginastmp3CAB TMPFrontiersAinda não há avaliações
- tmpFFE0 TMPDocumento6 páginastmpFFE0 TMPFrontiersAinda não há avaliações
- tmpE7E9 TMPDocumento14 páginastmpE7E9 TMPFrontiersAinda não há avaliações
- tmpE3C0 TMPDocumento17 páginastmpE3C0 TMPFrontiersAinda não há avaliações
- Tmpa077 TMPDocumento15 páginasTmpa077 TMPFrontiersAinda não há avaliações
- tmpF407 TMPDocumento17 páginastmpF407 TMPFrontiersAinda não há avaliações
- tmpF3B5 TMPDocumento15 páginastmpF3B5 TMPFrontiersAinda não há avaliações
- tmp6382 TMPDocumento8 páginastmp6382 TMPFrontiersAinda não há avaliações
- tmp37B8 TMPDocumento9 páginastmp37B8 TMPFrontiersAinda não há avaliações
- tmp72FE TMPDocumento8 páginastmp72FE TMPFrontiersAinda não há avaliações
- tmpC0A TMPDocumento9 páginastmpC0A TMPFrontiersAinda não há avaliações
- tmp8B94 TMPDocumento9 páginastmp8B94 TMPFrontiersAinda não há avaliações
- tmp9D75 TMPDocumento9 páginastmp9D75 TMPFrontiersAinda não há avaliações
- tmp60EF TMPDocumento20 páginastmp60EF TMPFrontiersAinda não há avaliações
- tmp998 TMPDocumento9 páginastmp998 TMPFrontiersAinda não há avaliações
- tmpD1FE TMPDocumento6 páginastmpD1FE TMPFrontiersAinda não há avaliações
- tmp4B57 TMPDocumento9 páginastmp4B57 TMPFrontiersAinda não há avaliações
- tmpA0D TMPDocumento9 páginastmpA0D TMPFrontiersAinda não há avaliações
- tmpC30A TMPDocumento10 páginastmpC30A TMPFrontiersAinda não há avaliações
- tmp2F3F TMPDocumento10 páginastmp2F3F TMPFrontiersAinda não há avaliações
- Tmp75a7 TMPDocumento8 páginasTmp75a7 TMPFrontiersAinda não há avaliações
- tmpB1BE TMPDocumento9 páginastmpB1BE TMPFrontiersAinda não há avaliações
- tmp27C1 TMPDocumento5 páginastmp27C1 TMPFrontiersAinda não há avaliações
- tmp3656 TMPDocumento14 páginastmp3656 TMPFrontiersAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Increased ICPDocumento7 páginasIncreased ICPK-La BreanneAinda não há avaliações
- Mitral RegurgitationDocumento22 páginasMitral Regurgitationrameshbmc100% (1)
- 426 C1 OsceDocumento21 páginas426 C1 Osceaini natashaAinda não há avaliações
- The Latest Mania: Selling Bipolar Disorder: EssayDocumento4 páginasThe Latest Mania: Selling Bipolar Disorder: EssayTula MouriñoAinda não há avaliações
- WebberDocumento8 páginasWebberHusainiAinda não há avaliações
- Nutrition and Aging P.110: - Risk For Malnutrition or OvernutritionDocumento21 páginasNutrition and Aging P.110: - Risk For Malnutrition or OvernutritionChester NicoleAinda não há avaliações
- Flow Trac SystemDocumento4 páginasFlow Trac Systempolar571Ainda não há avaliações
- Dyspnea Orthopnea PND PDFDocumento3 páginasDyspnea Orthopnea PND PDFNurulAlviFauzianaAinda não há avaliações
- Topical Antimicrobial Agents For Burn Wounds: David G. GreenhalghDocumento10 páginasTopical Antimicrobial Agents For Burn Wounds: David G. GreenhalghKimberlyLaw95Ainda não há avaliações
- Endoscopy and Microendoscopy of The Lacrimal Drainage SystemDocumento60 páginasEndoscopy and Microendoscopy of The Lacrimal Drainage SystemhwalijeeAinda não há avaliações
- ENG 40-Mineralni VodiDocumento24 páginasENG 40-Mineralni VodiNayden YotovAinda não há avaliações
- Nclex Past QuestionsDocumento452 páginasNclex Past Questionsjyka100% (21)
- Final Programme A4 - IPOS 2023 - CompressedDocumento60 páginasFinal Programme A4 - IPOS 2023 - CompressedFlorinaAinda não há avaliações
- ICU Admission Orders Page 1 of 5Documento5 páginasICU Admission Orders Page 1 of 5ramzicard943Ainda não há avaliações
- Measles (Campak, Rubeola, Gabak, Kerumut)Documento20 páginasMeasles (Campak, Rubeola, Gabak, Kerumut)Ami UtamiatiAinda não há avaliações
- Fdar Cabg 3nesurgicalDocumento5 páginasFdar Cabg 3nesurgicalMary Margareth GonzalesAinda não há avaliações
- Counselling-GATHER ApproachDocumento23 páginasCounselling-GATHER ApproachAnilkumar JaraliAinda não há avaliações
- Pysche OSCE - EPSE ExaminationDocumento1 páginaPysche OSCE - EPSE ExaminationAmber WangAinda não há avaliações
- Nursing Care Plan: (T: 38.4°C) PR: 145bpmDocumento6 páginasNursing Care Plan: (T: 38.4°C) PR: 145bpmAnne Ruth OlinAinda não há avaliações
- Anatomy of The Urinary SystemDocumento24 páginasAnatomy of The Urinary Systemgaylmm100% (2)
- DaVitaHealthCarePartnersInc 10K 20140221Documento212 páginasDaVitaHealthCarePartnersInc 10K 20140221Wallace Min0% (1)
- AptosDocumento2 páginasAptosMelisaCitraIkaAinda não há avaliações
- Evolutionary Theory and Cognitive Therapy PDFDocumento2 páginasEvolutionary Theory and Cognitive Therapy PDFDeniseAinda não há avaliações
- Hyperemesis GravidarumDocumento17 páginasHyperemesis GravidarumHo PingAinda não há avaliações
- Serous Fluids AnalysisDocumento15 páginasSerous Fluids AnalysisMustafa Khandgawi100% (1)
- 01 NCM 106 Intravenous TherapyDocumento19 páginas01 NCM 106 Intravenous TherapyDwight YmsonAinda não há avaliações
- Nursing Careplan Inadequate Tissue PerfusionDocumento2 páginasNursing Careplan Inadequate Tissue PerfusionAudrey LewisAinda não há avaliações
- Meridian Flush Empowerments Levels 3&4 Manual PDFDocumento8 páginasMeridian Flush Empowerments Levels 3&4 Manual PDFJoyce Lozano100% (2)
- Ds OresolDocumento1 páginaDs OresolShannie Padilla100% (1)
- Children With Special NeedsDocumento22 páginasChildren With Special NeedsNur AskinahAinda não há avaliações