Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- AnaphylaxisDocumento16 páginasAnaphylaxisEdgarAinda não há avaliações
- Postpartum HemorrhageDocumento22 páginasPostpartum HemorrhageReynaldiReikyHadiwijayaAinda não há avaliações
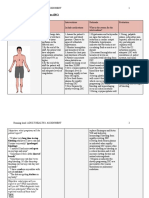
- Nursing Care Plan: St. Anthony's College San Jose, Antique Nursing Department Name: O.J.KDocumento4 páginasNursing Care Plan: St. Anthony's College San Jose, Antique Nursing Department Name: O.J.KKristine YoungAinda não há avaliações
- Pathology and Microbiology-QbDocumento3 páginasPathology and Microbiology-QbSolangkilisaravananAinda não há avaliações
- Postpartum-Haemorrhage 220719 PDFDocumento16 páginasPostpartum-Haemorrhage 220719 PDFMuathAinda não há avaliações
- Int J Lab Hematology - 2017 - Chabot Richards - Does Morphology Matter in 2017 An Approach To Morphologic Clues inDocumento8 páginasInt J Lab Hematology - 2017 - Chabot Richards - Does Morphology Matter in 2017 An Approach To Morphologic Clues inLidija MilkovskaAinda não há avaliações
- NCM 109 Module 3mDocumento25 páginasNCM 109 Module 3mKyle ChuaAinda não há avaliações
- BOTSCH 2009 Retrospective Study of Dogs With ThrombocytopeniaDocumento5 páginasBOTSCH 2009 Retrospective Study of Dogs With ThrombocytopeniaElle Burton-BradleyAinda não há avaliações
- Hematology: CoagulationDocumento40 páginasHematology: CoagulationMuhammad SaeedAinda não há avaliações
- DIC Case StudyDocumento3 páginasDIC Case StudyJuliaAinda não há avaliações
- House, MD QuestionsDocumento2 páginasHouse, MD QuestionsAidan ManciniAinda não há avaliações
- BRS General SurgeryDocumento520 páginasBRS General SurgeryWilliam Wiryawan100% (18)
- Test Drills TwoDocumento15 páginasTest Drills TwoSeanmarie CabralesAinda não há avaliações
- Nic Noc Risk For Bleeding (MB Anik)Documento3 páginasNic Noc Risk For Bleeding (MB Anik)Luthfiy IrfanasruddinAinda não há avaliações
- Guidelines For The Rational Use of Blood Blood ProductsDocumento120 páginasGuidelines For The Rational Use of Blood Blood ProductsHafiz Hamidi100% (1)
- Clinical Aspects, Diagnosis and Management of Loxosceles Spider Envenomation: Literature and Case ReviewDocumento17 páginasClinical Aspects, Diagnosis and Management of Loxosceles Spider Envenomation: Literature and Case ReviewRay Daniel LFAinda não há avaliações
- Fundamentals NotesDocumento23 páginasFundamentals NotesElle R Naceno100% (4)
- IUFDDocumento29 páginasIUFDfasyanneshaAinda não há avaliações
- Disseminated Intravascular CoagulationDocumento29 páginasDisseminated Intravascular CoagulationAnju RadhikaAinda não há avaliações
- 2022 Book TheCoagulationLabyrinthOfCovidDocumento215 páginas2022 Book TheCoagulationLabyrinthOfCovidgustavo orsoliniAinda não há avaliações
- The APACHE II Severity of Disease Classification SystemDocumento2 páginasThe APACHE II Severity of Disease Classification SystemPipipAinda não há avaliações
- Blood Transfusion, Complications and ManagementDocumento14 páginasBlood Transfusion, Complications and ManagementRubini Devi100% (1)
- Sepsis-Syok Septik 5-12-15Documento36 páginasSepsis-Syok Septik 5-12-15Titi Nur IndrawatiAinda não há avaliações
- Cheetsheet 6Documento1 páginaCheetsheet 6Rick Frea92% (12)
- Comprehensive NCLEX Exam 5Documento21 páginasComprehensive NCLEX Exam 5milkah mwauraAinda não há avaliações
- Disseminated Intravascular CoagulationDocumento17 páginasDisseminated Intravascular Coagulationr DAinda não há avaliações
- Oncology TestDocumento32 páginasOncology TestPhilip Gene II MalacasAinda não há avaliações
- 398 - Amniotic Fluid EmbolismDocumento8 páginas398 - Amniotic Fluid EmbolismAggrawal AnilAinda não há avaliações
- Haematological History and Examination 18092012-2Documento8 páginasHaematological History and Examination 18092012-2Shahin KazemzadehAinda não há avaliações
- Final Hand Book of Covid 19 AFMCDocumento174 páginasFinal Hand Book of Covid 19 AFMCPadmapriya SrinivasanAinda não há avaliações