Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1091)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Cell Cycle and Cell DivisionDocumento8 páginasCell Cycle and Cell Divisionbhupeshgalani100% (2)
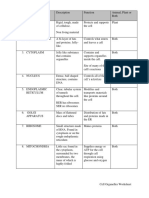
- Cell Organelles WorksheetDocumento8 páginasCell Organelles WorksheetJohn OsborneAinda não há avaliações
- Biological Macromolecules: Nucleic Acids Proteins Carbohydrates LipidsDocumento1 páginaBiological Macromolecules: Nucleic Acids Proteins Carbohydrates LipidsJoan PamatAinda não há avaliações
- Hema 2 - Prelim Topic 1-Intro To HemostasisDocumento4 páginasHema 2 - Prelim Topic 1-Intro To HemostasisLowenstein JenzenAinda não há avaliações
- The Cell Biology PDFDocumento66 páginasThe Cell Biology PDFSamina PachaAinda não há avaliações
- Yoshinori Ohsumi - Autophagy From Beginning To EndDocumento2 páginasYoshinori Ohsumi - Autophagy From Beginning To Endcesiahdez0% (1)
- Jadwal Pemberian ObatDocumento1 páginaJadwal Pemberian ObatRegita Ayu LestariAinda não há avaliações
- MR Supple All 2014Documento429 páginasMR Supple All 2014Regita Ayu LestariAinda não há avaliações
- CAC Synthetic PristaneDocumento1 páginaCAC Synthetic PristaneRegita Ayu LestariAinda não há avaliações
- Pristane, A Non-Antigenic Adjuvant, Induces MHC Class II-Restricted, Arthritogenic T Cells in The RatDocumento19 páginasPristane, A Non-Antigenic Adjuvant, Induces MHC Class II-Restricted, Arthritogenic T Cells in The RatRegita Ayu LestariAinda não há avaliações
- A C A D e M I C S C I e N C e SDocumento6 páginasA C A D e M I C S C I e N C e SRegita Ayu LestariAinda não há avaliações
- Calculation of AUC Using The Trapezoidal Rule: Time C C AUCDocumento2 páginasCalculation of AUC Using The Trapezoidal Rule: Time C C AUCRegita Ayu Lestari100% (1)
- XI Botany ChapterWise Prvs Questions HssliveDocumento25 páginasXI Botany ChapterWise Prvs Questions Hsslivejithu63% (8)
- Figures Citrus Essential Oils in Aromatherapy Therapeutic Effects and MechanismsDocumento23 páginasFigures Citrus Essential Oils in Aromatherapy Therapeutic Effects and MechanismsTariq Jamil FaridiAinda não há avaliações
- Apoptosis-Oncogenes-Tumor Suppressors & Cancer - ICS PresentationDocumento30 páginasApoptosis-Oncogenes-Tumor Suppressors & Cancer - ICS PresentationRayAinda não há avaliações
- Bortolato2016 Depresi Pada KankerDocumento50 páginasBortolato2016 Depresi Pada KankerYudha HudayaAinda não há avaliações
- Fragrance With Antiaging Benefits: Naturals-Driven Functionality For Added ValueDocumento6 páginasFragrance With Antiaging Benefits: Naturals-Driven Functionality For Added Valuejasminai_17Ainda não há avaliações
- Meiosis and Sexual ReproductionDocumento48 páginasMeiosis and Sexual Reproductionerdayu86100% (1)
- Assignment 1 Biol 1700 Fall2019 NM Final Robert Mccarney 100615317Documento12 páginasAssignment 1 Biol 1700 Fall2019 NM Final Robert Mccarney 100615317api-490786676Ainda não há avaliações
- Reproduction: Question Paper 3Documento12 páginasReproduction: Question Paper 3hesareeAinda não há avaliações
- Ic103: Materials Chemistry-I: Institute Core Course For Btech ProgramDocumento23 páginasIc103: Materials Chemistry-I: Institute Core Course For Btech ProgramAkash LikharAinda não há avaliações
- Proteins BIOC2069 #1Documento36 páginasProteins BIOC2069 #1erica williamsAinda não há avaliações
- Tabel Perbandingan MSC Dan EksosomDocumento5 páginasTabel Perbandingan MSC Dan EksosomRaisha FathimaAinda não há avaliações
- QCE Bio Chapter 5 - Review - Student - Book - AnswersDocumento5 páginasQCE Bio Chapter 5 - Review - Student - Book - AnswersFransche BeukesAinda não há avaliações
- Sudipta Baur - Mehebub AlamDocumento19 páginasSudipta Baur - Mehebub AlamSudip MajiAinda não há avaliações
- Enzymes Lecture 1 2015animationDocumento80 páginasEnzymes Lecture 1 2015animationSarfaras KKAinda não há avaliações
- B1 Cells EOT MSDocumento3 páginasB1 Cells EOT MSroAinda não há avaliações
- 1st Lec On Endo Physiology by DR RoomiDocumento24 páginas1st Lec On Endo Physiology by DR RoomiMudassar RoomiAinda não há avaliações
- Tuto (SAQ)Documento6 páginasTuto (SAQ)ANIS HUMAIRA ABDUL HAFIZAinda não há avaliações
- Subject: Biochemistry Topic:Lipid Metabolism 2 Lecturer: Dr. Laygo DATE: NOV. 2010Documento11 páginasSubject: Biochemistry Topic:Lipid Metabolism 2 Lecturer: Dr. Laygo DATE: NOV. 2010Std DlshsiAinda não há avaliações
- Gen Bio - BiomoleculesDocumento3 páginasGen Bio - BiomoleculesRamona Grace SimeraAinda não há avaliações
- Textbook On Clinical Ocular Pharmacology & Therapeutics (079-117)Documento39 páginasTextbook On Clinical Ocular Pharmacology & Therapeutics (079-117)Claudia Alejandra Varon100% (1)
- Amino Acids and ProteinDocumento32 páginasAmino Acids and ProteinArchishmaan UdgataAinda não há avaliações
- Molecular Basis of Inheritance, Class 12, Cbse NotesDocumento33 páginasMolecular Basis of Inheritance, Class 12, Cbse NotesSubho Bhattacharya50% (4)
- VIBAR, Justine - Biochem LE 1&2Documento3 páginasVIBAR, Justine - Biochem LE 1&2JustineAinda não há avaliações
- NecrosisDocumento12 páginasNecrosisAneeza AhmadAinda não há avaliações