Você também pode gostar
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- How To Write A Journal ArticleDocumento50 páginasHow To Write A Journal ArticleSaeed Al-Yafei80% (5)
- Lesson Plan - Contemporary Arts From The PhilippinesDocumento4 páginasLesson Plan - Contemporary Arts From The PhilippinesEljay Flores96% (25)
- 22 Self-Actualization Tests & Tools To Apply Maslow's TheoryDocumento34 páginas22 Self-Actualization Tests & Tools To Apply Maslow's TheoryIbrahim HarfoushAinda não há avaliações
- Nephrology MCQsDocumento7 páginasNephrology MCQsSaeed Al-Yafei67% (6)
- Assessment Form 2 PDFDocumento1 páginaAssessment Form 2 PDFAgnes Bansil Vitug100% (1)
- Skelly S Mcqs in Tropical MedicineDocumento29 páginasSkelly S Mcqs in Tropical MedicineSaeed Al-Yafei92% (13)
- Cognitive PsychologyDocumento22 páginasCognitive PsychologySaeed Al-Yafei100% (6)
- How To Write A Scientific Original ArticleDocumento67 páginasHow To Write A Scientific Original ArticleSaeed Al-YafeiAinda não há avaliações
- Speak Out Intermediate Tests Track ListingDocumento1 páginaSpeak Out Intermediate Tests Track Listingbob43% (7)
- What Makes A Good TeacherDocumento4 páginasWhat Makes A Good TeacherJravi ShastriAinda não há avaliações
- Diagnosis of Gastrointestinal Bleeding in AdultsDocumento8 páginasDiagnosis of Gastrointestinal Bleeding in AdultsSaeed Al-YafeiAinda não há avaliações
- Endnote 7 TrainingDocumento84 páginasEndnote 7 TrainingSaeed Al-Yafei100% (2)
- Preparatory Lecture: Confounding and BiasDocumento144 páginasPreparatory Lecture: Confounding and BiasSaeed Al-YafeiAinda não há avaliações
- Probability Calculation in MinesweeperDocumento2 páginasProbability Calculation in MinesweeperBrayan Perez ContrerasAinda não há avaliações
- Exam Steps and Process - Read FirstDocumento3 páginasExam Steps and Process - Read FirstDeejaay2010Ainda não há avaliações
- The Implications of The Dodo Bird Verdict For Training in Psychotherapy Prioritizing Process ObservationDocumento4 páginasThe Implications of The Dodo Bird Verdict For Training in Psychotherapy Prioritizing Process ObservationSebastian PorcelAinda não há avaliações
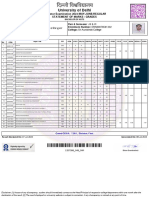
- University of Delhi: Semester Examination 2023-MAY-JUNE:REGULAR Statement of Marks / GradesDocumento2 páginasUniversity of Delhi: Semester Examination 2023-MAY-JUNE:REGULAR Statement of Marks / GradesFit CollegeAinda não há avaliações
- Information Brochure & Guidelines For Filling of Online Application Form For Recruitment of Non-Teaching Positions in Delhi UniversityDocumento106 páginasInformation Brochure & Guidelines For Filling of Online Application Form For Recruitment of Non-Teaching Positions in Delhi UniversityVidhiLegal BlogAinda não há avaliações
- Cambridge Aice Marine Science SyllabusDocumento32 páginasCambridge Aice Marine Science Syllabusapi-280088207Ainda não há avaliações
- Resume 2021 RDocumento3 páginasResume 2021 Rapi-576057342Ainda não há avaliações
- Mslearn dp100 14Documento2 páginasMslearn dp100 14Emily RapaniAinda não há avaliações
- Department of Theatre and Film Studies: Nnamdi Azikiwe UniversityDocumento7 páginasDepartment of Theatre and Film Studies: Nnamdi Azikiwe Universityanon_453956231Ainda não há avaliações
- Structure of Academic TextsDocumento22 páginasStructure of Academic TextsBehappy 89Ainda não há avaliações
- Drivers Ed Homework AnswersDocumento7 páginasDrivers Ed Homework Answersafnogtyaiergwk100% (1)
- Marketing Management Course OutlineDocumento3 páginasMarketing Management Course OutlineShehryar HumayunAinda não há avaliações
- Advisory Assignment Order Junior High SchoolDocumento1 páginaAdvisory Assignment Order Junior High SchoolJaz and Ysha's ChannelAinda não há avaliações
- GCSE New Spec Performance MarksheetDocumento2 páginasGCSE New Spec Performance MarksheetChris PowellAinda não há avaliações
- Algebraic FractionsDocumento11 páginasAlgebraic FractionsSafiya Shiraz ImamudeenAinda não há avaliações
- Building Your Weekly SDR Calendar-Peer Review Assignment-Mohamed AbdelrahmanDocumento3 páginasBuilding Your Weekly SDR Calendar-Peer Review Assignment-Mohamed AbdelrahmanrtwthcdjwtAinda não há avaliações
- Linux AdministrationDocumento361 páginasLinux AdministrationmohdkmnAinda não há avaliações
- Barnard College, Title IX, Dismissal LetterDocumento3 páginasBarnard College, Title IX, Dismissal LetterWhirlfluxAinda não há avaliações
- HR Questions InterviewDocumento54 páginasHR Questions InterviewAlice AliceAinda não há avaliações
- 4-ProjectCharterTemplatePDF 0Documento5 páginas4-ProjectCharterTemplatePDF 0maria shintaAinda não há avaliações
- YPD Guide Executive Summary PDFDocumento2 páginasYPD Guide Executive Summary PDFAlex FarrowAinda não há avaliações
- Bbfa4034 Accounting Theory & Practice 1: MAIN SOURCE of Reference - Coursework Test + Final ExamDocumento12 páginasBbfa4034 Accounting Theory & Practice 1: MAIN SOURCE of Reference - Coursework Test + Final ExamCHONG JIA WEN CARMENAinda não há avaliações
- Virtue Ethics FinalDocumento19 páginasVirtue Ethics FinalAlna JaeAinda não há avaliações
- PHD Ordinance Msubaroda IndiaDocumento15 páginasPHD Ordinance Msubaroda IndiaBhagirath Baria100% (1)
- Project 2 ExampleDocumento6 páginasProject 2 ExampleShalomAinda não há avaliações