Você também pode gostar
- Aerovent, Apovent Atronase, Ipraxa, Ipvent Rhinovent, Rinatecrinovagos, Atrovent, Atrovent HfaDocumento4 páginasAerovent, Apovent Atronase, Ipraxa, Ipvent Rhinovent, Rinatecrinovagos, Atrovent, Atrovent HfaGwyn RosalesAinda não há avaliações
- TelfastDocumento3 páginasTelfastjbahalkehAinda não há avaliações
- Drug StudyDocumento8 páginasDrug StudyGian Era100% (1)
- PethidineDocumento6 páginasPethidineAnonymous NQDRERPcjAinda não há avaliações
- HyoscineDocumento4 páginasHyoscineHana HanaAinda não há avaliações
- Ciprofloxacin CiproDocumento1 páginaCiprofloxacin CiproKristi WrayAinda não há avaliações
- Drug StudyDocumento9 páginasDrug StudyChristine PunsalanAinda não há avaliações
- Med Template - Ipratropium Bromide AtroventDocumento2 páginasMed Template - Ipratropium Bromide AtroventAshlee KeeferAinda não há avaliações
- LansoprazoleDocumento3 páginasLansoprazoleJody FelizioAinda não há avaliações
- Drug Literature For MupirocinDocumento3 páginasDrug Literature For MupirocinKate EvangelistaAinda não há avaliações
- EzetimibeDocumento3 páginasEzetimibeapi-3797941Ainda não há avaliações
- DRUG-STUDY Butorphanol LRDR AngelicaRonquilloDocumento2 páginasDRUG-STUDY Butorphanol LRDR AngelicaRonquillokarl eiron delos santosAinda não há avaliações
- KetoconazoleDocumento2 páginasKetoconazoleMD. DELWAR HOSSAINAinda não há avaliações
- Drug StudyDocumento11 páginasDrug StudyJay VillasotoAinda não há avaliações
- BromhexineDocumento2 páginasBromhexinejulie0% (1)
- Aminophylline GuidelinesDocumento2 páginasAminophylline GuidelinesA. Shamshir A. MoktiAinda não há avaliações
- Drug AdvilDocumento1 páginaDrug AdvilDiana Laura LeiAinda não há avaliações
- ClindamycinDocumento3 páginasClindamycinShaira TanAinda não há avaliações
- IndomethacinDocumento9 páginasIndomethacinQuiKe PvAinda não há avaliações
- DelavirdineDocumento2 páginasDelavirdineRosher Deliman JanoyanAinda não há avaliações
- St. Paul University Dumaguete St. Paul University System College of Nursing ISO 9001Documento16 páginasSt. Paul University Dumaguete St. Paul University System College of Nursing ISO 9001Dinarkram Rabreca EculAinda não há avaliações
- Drug Analysis: Submitted By: GALICINAO, Gretta Shalou GDocumento9 páginasDrug Analysis: Submitted By: GALICINAO, Gretta Shalou GggalicinaoAinda não há avaliações
- AtroventDocumento1 páginaAtroventSheri490100% (1)
- Drug StudyDocumento6 páginasDrug StudyChickz HunterAinda não há avaliações
- Pharma CardsDocumento5 páginasPharma CardsazancheAinda não há avaliações
- Anes Drugs TableDocumento20 páginasAnes Drugs TableKathleen Grace ManiagoAinda não há avaliações
- Longifene ... Longifene-... Stimulone: Available BrandsDocumento2 páginasLongifene ... Longifene-... Stimulone: Available BrandsJustin Raul Dela CuadraAinda não há avaliações
- Brand Name: Bambec Generic Name: Bambuterol HCL Indication: Bronchial AsthmaDocumento2 páginasBrand Name: Bambec Generic Name: Bambuterol HCL Indication: Bronchial AsthmaianecunarAinda não há avaliações
- EvistaDocumento18 páginasEvistaBrankoPopovićAinda não há avaliações
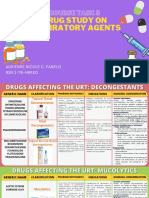
- Course Task 8 Drug Study On Respiratory AgentsDocumento23 páginasCourse Task 8 Drug Study On Respiratory AgentsAdrienne Nicole PaneloAinda não há avaliações
- Rathna Drug Card in (Lovenox)Documento1 páginaRathna Drug Card in (Lovenox)erdos13Ainda não há avaliações
- Daptomycin (Cubicin)Documento1 páginaDaptomycin (Cubicin)Adrianne BazoAinda não há avaliações
- Prazosin Tablet (Prazosin)Documento6 páginasPrazosin Tablet (Prazosin)Chenta Bulan MerinduAinda não há avaliações
- Indomethacin 392Documento17 páginasIndomethacin 392Mahadie Hasan JahadAinda não há avaliações
- Magnesium SulfateDocumento1 páginaMagnesium SulfateSilinna May Lee Sanico0% (1)
- Drug OmeprazoleDocumento1 páginaDrug OmeprazoleSrkocherAinda não há avaliações
- Pentabio PDFDocumento7 páginasPentabio PDFDicky KurniawanAinda não há avaliações
- Albuterol Pediatric Drug CardDocumento2 páginasAlbuterol Pediatric Drug CardAnthonyMedinaAinda não há avaliações
- C C C Vertigo,: Electrolyte and Water Balance AgentDocumento12 páginasC C C Vertigo,: Electrolyte and Water Balance AgentEarl Tony TrinidadAinda não há avaliações
- AtivanDocumento1 páginaAtivanSheri490Ainda não há avaliações
- Ferrous SulfateDocumento2 páginasFerrous SulfateKylahAinda não há avaliações
- TrazodoneDocumento20 páginasTrazodoneAjay MehtaAinda não há avaliações
- Obstetric Nursing Care PlanDocumento12 páginasObstetric Nursing Care PlanJass Mira Bueno100% (1)
- BrivaracetamDocumento110 páginasBrivaracetamBendisDacicaAinda não há avaliações
- PhenobarbitalDocumento1 páginaPhenobarbitalJesrel DelotaAinda não há avaliações
- Duphaston PDFDocumento4 páginasDuphaston PDFmarcusjanaAinda não há avaliações
- Adults and Children 15 Y Pediatric 6 - 14 YDocumento2 páginasAdults and Children 15 Y Pediatric 6 - 14 YFildehl Janice Bomediano Catipay100% (1)
- OxytocinDocumento2 páginasOxytocinshefawAinda não há avaliações
- PrevacidDocumento1 páginaPrevacidAdrianne BazoAinda não há avaliações
- Procreative Health Is The Moral Obligation of Parents To Have The Healthiest Children Through All Natural and Artificial Means AvailableDocumento9 páginasProcreative Health Is The Moral Obligation of Parents To Have The Healthiest Children Through All Natural and Artificial Means AvailableShiela Mae GalisaAinda não há avaliações
- NarcanDocumento31 páginasNarcanmahmoud fuqahaAinda não há avaliações
- Side Effects of Pregabalin DrugDocumento20 páginasSide Effects of Pregabalin DrugtulipcatcherAinda não há avaliações
- Glycerin: (Gli-Ser-In)Documento2 páginasGlycerin: (Gli-Ser-In)Aryanto DedyAinda não há avaliações
- Drug StudyDocumento4 páginasDrug StudyCharlyn Mae BirondoAinda não há avaliações
- Summary of Key BLS Components For Adults Children and InfantDocumento26 páginasSummary of Key BLS Components For Adults Children and Infantjulesubayubay5428Ainda não há avaliações
- Dokumen - Tips Common Cold Allergic Rhinitispharmaceutical C P e Program Common ColdDocumento27 páginasDokumen - Tips Common Cold Allergic Rhinitispharmaceutical C P e Program Common ColdVerqueza OdzongAinda não há avaliações
- Drug StudyDocumento7 páginasDrug Studykamirure02Ainda não há avaliações
- Asthma SimDocumento3 páginasAsthma SimwysosylwAinda não há avaliações
- Sas1 ClinpharDocumento7 páginasSas1 ClinpharAlyssa Marie Petonio BialaAinda não há avaliações
- ARSM Horn Repertoire 2017 OnwardsDocumento1 páginaARSM Horn Repertoire 2017 Onwardshappyscottlee3438Ainda não há avaliações
- TCL EURO Price List From March 2016Documento16 páginasTCL EURO Price List From March 2016happyscottlee3438Ainda não há avaliações
- These Music Exams by Clara Taylor, ABRSMDocumento48 páginasThese Music Exams by Clara Taylor, ABRSMhappyscottlee3438Ainda não há avaliações
- ARSM Horn Repertoire 2017 OnwardsDocumento1 páginaARSM Horn Repertoire 2017 Onwardshappyscottlee3438Ainda não há avaliações
- ARSM Double Bass 2017 OnwardsDocumento1 páginaARSM Double Bass 2017 Onwardshappyscottlee3438Ainda não há avaliações
- New ARSM Programme Form (Specimen) 2017 OnwardsDocumento2 páginasNew ARSM Programme Form (Specimen) 2017 Onwardshappyscottlee3438Ainda não há avaliações
- ARSM Viola Repertoire 2017 OnwardsDocumento2 páginasARSM Viola Repertoire 2017 Onwardshappyscottlee3438Ainda não há avaliações
- ARSM Singing Repertoire 2017 OnwardsDocumento8 páginasARSM Singing Repertoire 2017 Onwardshappyscottlee3438Ainda não há avaliações
- ARSM Flute Repertoire 2017 OnwardsDocumento2 páginasARSM Flute Repertoire 2017 Onwardshappyscottlee3438Ainda não há avaliações
- New ARSM Programme Form (Specimen) 2017 OnwardsDocumento2 páginasNew ARSM Programme Form (Specimen) 2017 Onwardshappyscottlee3438Ainda não há avaliações
- ARSM Cello Repertoire 2017 OnwardsDocumento1 páginaARSM Cello Repertoire 2017 Onwardshappyscottlee3438Ainda não há avaliações
- ARSM Tuba Repertoire 2017 OnwardsDocumento1 páginaARSM Tuba Repertoire 2017 Onwardshappyscottlee3438Ainda não há avaliações
- ARSM Violin Repertoire 2017 OnwardsDocumento2 páginasARSM Violin Repertoire 2017 Onwardshappyscottlee3438100% (1)
- ARSM Trombone Repertoire 2017 OnwardsDocumento2 páginasARSM Trombone Repertoire 2017 Onwardshappyscottlee3438Ainda não há avaliações
- ARSM Trumpet Repertoire 2017 OnwardsDocumento1 páginaARSM Trumpet Repertoire 2017 Onwardshappyscottlee3438Ainda não há avaliações
- ARSM Recorder Repertoire 2017 OnwardsDocumento2 páginasARSM Recorder Repertoire 2017 Onwardshappyscottlee3438Ainda não há avaliações
- ARSM Saxophone Repertoire 2017 OnwardsDocumento1 páginaARSM Saxophone Repertoire 2017 Onwardshappyscottlee3438Ainda não há avaliações
- ARSM Baritone Euphonium 2017 OnwardsDocumento1 páginaARSM Baritone Euphonium 2017 Onwardshappyscottlee3438Ainda não há avaliações
- ARSM Percussion 2017 OnwardsDocumento1 páginaARSM Percussion 2017 Onwardshappyscottlee3438Ainda não há avaliações
- ARSM Bassoon Repertoire 2017 OnwardsDocumento1 páginaARSM Bassoon Repertoire 2017 Onwardshappyscottlee3438Ainda não há avaliações
- ARSM Oboe Repertoire 2017 OnwardsDocumento1 páginaARSM Oboe Repertoire 2017 Onwardshappyscottlee3438Ainda não há avaliações
- ARSM eFlatHorn 2017 OnwardsDocumento1 páginaARSM eFlatHorn 2017 Onwardshappyscottlee3438Ainda não há avaliações
- ARSM Clarinet Repertoire 2017 OnwardsDocumento2 páginasARSM Clarinet Repertoire 2017 Onwardshappyscottlee3438Ainda não há avaliações
- ARSM Guitar Repertoire 2017 OnwardsDocumento2 páginasARSM Guitar Repertoire 2017 Onwardshappyscottlee3438100% (1)
- New ABRSM ARSM Syllabus 2017 OnwardsDocumento13 páginasNew ABRSM ARSM Syllabus 2017 Onwardshappyscottlee343850% (2)
- ARSM Organ Repertoire 2017 OnwardsDocumento1 páginaARSM Organ Repertoire 2017 Onwardshappyscottlee3438Ainda não há avaliações
- ARSM Piano Repertoire 2017 OnwardsDocumento3 páginasARSM Piano Repertoire 2017 Onwardshappyscottlee343875% (4)
- ARSM Harpsichord Repertoire 2017 OnwardsDocumento1 páginaARSM Harpsichord Repertoire 2017 Onwardshappyscottlee3438Ainda não há avaliações
- ARSM Harp Repertoire 2017 OnwardsDocumento1 páginaARSM Harp Repertoire 2017 Onwardshappyscottlee3438Ainda não há avaliações
- New ABRSM ARSM Marking Criteria 2017Documento1 páginaNew ABRSM ARSM Marking Criteria 2017happyscottlee3438100% (1)
- Note Regarding Retiring DoctorsDocumento3 páginasNote Regarding Retiring DoctorsnamankumaragrawalAinda não há avaliações
- Berkshire HRTDocumento7 páginasBerkshire HRTpiAinda não há avaliações
- Bowen Family TheoryDocumento320 páginasBowen Family Theorytonifieraru100% (14)
- BIS A2000 - Operating ManualDocumento102 páginasBIS A2000 - Operating Manualgabygg06Ainda não há avaliações
- Discharge Planning: MedicationDocumento3 páginasDischarge Planning: MedicationLeasAinda não há avaliações
- Ilovepdf Merged PDFDocumento134 páginasIlovepdf Merged PDFhelalAinda não há avaliações
- Water and Electrolyte Balance Case StudyDocumento3 páginasWater and Electrolyte Balance Case Studyzamadula100% (3)
- StrabismusDocumento20 páginasStrabismusmerycoAinda não há avaliações
- Dental AssistantDocumento2 páginasDental Assistantapi-78993102Ainda não há avaliações
- Antepartum HemorrhageDocumento48 páginasAntepartum HemorrhageJoshua EvansAinda não há avaliações
- DSWD Guidelines For Residential FacilitiesDocumento12 páginasDSWD Guidelines For Residential FacilitiesCharlene Ordoñez Dela CruzAinda não há avaliações
- Richa Kothari PDFDocumento4 páginasRicha Kothari PDFChinta Ula RanaAinda não há avaliações
- VA DoD Management of Concussion Mild Traumatic Brain InjuryDocumento112 páginasVA DoD Management of Concussion Mild Traumatic Brain InjurycirtestAinda não há avaliações
- Points From Accupuncture AtlasDocumento1 páginaPoints From Accupuncture AtlasdishkuAinda não há avaliações
- Mayur - 01Documento2 páginasMayur - 01mukesh jambukiyaAinda não há avaliações
- Format N Assessment Isb533Documento9 páginasFormat N Assessment Isb533Anis HayatiAinda não há avaliações
- Daftar Pustaka OaDocumento2 páginasDaftar Pustaka OaCut Naja SoviaAinda não há avaliações
- Perbedaan Kadar Hbsag Sampel Serum Dan Plasma Metode Clia Pada PendonorDocumento7 páginasPerbedaan Kadar Hbsag Sampel Serum Dan Plasma Metode Clia Pada PendonorAAK DHGRiski MaulanaAinda não há avaliações
- Chronic Obstructive Pulmonary DiseaseDocumento36 páginasChronic Obstructive Pulmonary DiseaseHazel ManuelAinda não há avaliações
- Health 10 Q1W1Documento25 páginasHealth 10 Q1W1Gladys Pangasinan AngalaAinda não há avaliações
- Chapter 4 Marketing Department: Company 1-Apollo Hospitals Enterprises LTD (Apollo)Documento20 páginasChapter 4 Marketing Department: Company 1-Apollo Hospitals Enterprises LTD (Apollo)TYB92BINDRA GURSHEEN KAUR R.Ainda não há avaliações
- Sample Written Program For Respiratory ProtectionDocumento45 páginasSample Written Program For Respiratory ProtectionSergio MacedoAinda não há avaliações
- Directions: Choose The Letter of The Correct Answer. Write Your Answer On A Separate Sheet. STRICTLY NO Erasures and Write Capital Letters Only!Documento3 páginasDirections: Choose The Letter of The Correct Answer. Write Your Answer On A Separate Sheet. STRICTLY NO Erasures and Write Capital Letters Only!Diane CiprianoAinda não há avaliações
- RT Specific ExamDocumento3 páginasRT Specific ExamGoutam Kumar Deb100% (1)
- Global Developmental DelayDocumento2 páginasGlobal Developmental DelayAtlerAinda não há avaliações
- Alternative Treatment Strategies For Pseudo-Class III Malocclusion With Mild AsymmetryDocumento17 páginasAlternative Treatment Strategies For Pseudo-Class III Malocclusion With Mild AsymmetrySchwan AbdulkareemAinda não há avaliações
- DiphtheriaDocumento11 páginasDiphtheriabrigde_xAinda não há avaliações
- Elliot Hulse - Rational Fasting Diet ManualDocumento43 páginasElliot Hulse - Rational Fasting Diet ManualRyan Franco96% (27)
- Electrostimulatoare Denas MsDocumento43 páginasElectrostimulatoare Denas MsDanOlteanuAinda não há avaliações
- Ebook Atlas of Interventional Orthopedics Procedures Essential Guide For Fluoroscopy and Ultrasound Guided Procedures PDF Full Chapter PDFDocumento68 páginasEbook Atlas of Interventional Orthopedics Procedures Essential Guide For Fluoroscopy and Ultrasound Guided Procedures PDF Full Chapter PDFcharles.schmidt276100% (26)