Você também pode gostar
- IRB Review Protects Human SubjectsDocumento65 páginasIRB Review Protects Human SubjectsClaudia Quiñones RamosAinda não há avaliações
- DocDocumento14 páginasDocSara Montañez BarajasAinda não há avaliações
- ICH GCP & Indian Clinical Trial GuidelineDocumento97 páginasICH GCP & Indian Clinical Trial GuidelineRanjeet PrasadAinda não há avaliações
- Policy: SOP: 404 Continuing ReviewDocumento7 páginasPolicy: SOP: 404 Continuing ReviewHarly SollanoAinda não há avaliações
- Lectura 4Documento8 páginasLectura 4Marissella GutierrezAinda não há avaliações
- The University of Burdwan Institutional Clinical Ethics CommitteeDocumento14 páginasThe University of Burdwan Institutional Clinical Ethics Committeebhramar bAinda não há avaliações
- FMR No 4Documento7 páginasFMR No 4Dwi RatihAinda não há avaliações
- Part 1: What Is An Institutional Review Board?Documento10 páginasPart 1: What Is An Institutional Review Board?Alexandru CosminAinda não há avaliações
- UHSRC Expedited Review ProceduresDocumento4 páginasUHSRC Expedited Review Proceduresz.wAinda não há avaliações
- HC Inspection Process Guidance Document Final Dec 15 2015 3Documento25 páginasHC Inspection Process Guidance Document Final Dec 15 2015 3Dawn CasuncadAinda não há avaliações
- Standard Operating Procedure Trial Master File and 421 Main Evidence in TheDocumento33 páginasStandard Operating Procedure Trial Master File and 421 Main Evidence in Theahmed.bouchenakAinda não há avaliações
- Research and Ethical CommitteeDocumento8 páginasResearch and Ethical Committeefarha naazAinda não há avaliações
- Screening and Enrollment: Standard Operating Procedures For Clinical Research at Kent State UniversityDocumento6 páginasScreening and Enrollment: Standard Operating Procedures For Clinical Research at Kent State UniversityAlberio CygnusAinda não há avaliações
- Guidance For Retrospective Chart Review StudiesDocumento3 páginasGuidance For Retrospective Chart Review StudiesFabio da CostaAinda não há avaliações
- GPC Quality AssuranceDocumento10 páginasGPC Quality Assuranceprintbox.argAinda não há avaliações
- Standard Operating Procedures For Clinical Research CoordinatorsDocumento13 páginasStandard Operating Procedures For Clinical Research Coordinatorsmmohit_990% (1)
- Clinical Trial MonitoringDocumento14 páginasClinical Trial Monitoringsreeraj.guruvayoor100% (1)
- Jira TrainingDocumento22 páginasJira Trainingkasalasurya16Ainda não há avaliações
- QA and monitoring roles in clinical trialsDocumento12 páginasQA and monitoring roles in clinical trialsRenzo FernandezAinda não há avaliações
- SOP 302 SiteQualificationVisitDocumento3 páginasSOP 302 SiteQualificationVisitcnonsowonAinda não há avaliações
- Audit and Inspection in Clinical TrialDocumento57 páginasAudit and Inspection in Clinical TrialRanjeet Prasad100% (2)
- IRB Form ICHGCPE6 PI AttestationDocumento3 páginasIRB Form ICHGCPE6 PI AttestationDeeAinda não há avaliações
- SOP 303 SiteInitiationVisitDocumento3 páginasSOP 303 SiteInitiationVisitna sarvaAinda não há avaliações
- ScientificDocumento4 páginasScientificNarendar ReddyAinda não há avaliações
- Common Types of Research ProjectsDocumento4 páginasCommon Types of Research ProjectsUtpal PandyaAinda não há avaliações
- SOP 302 SiteQualificationVisitDocumento3 páginasSOP 302 SiteQualificationVisitna sarvaAinda não há avaliações
- WHO Guidance Research Methods Health-EDRM 6.4Documento13 páginasWHO Guidance Research Methods Health-EDRM 6.4SAURAV KUMAR VERMAAinda não há avaliações
- CRO Contract Research OrganizationDocumento10 páginasCRO Contract Research OrganizationibrahimAinda não há avaliações
- Audit: Role and Responsibilities of Auditor in Clinical Trial As Per Ich GCPDocumento7 páginasAudit: Role and Responsibilities of Auditor in Clinical Trial As Per Ich GCPGeethika GummadiAinda não há avaliações
- Site Close-Out Visit: Standard Operating Procedures For Clinical Research at Kent State UniversityDocumento4 páginasSite Close-Out Visit: Standard Operating Procedures For Clinical Research at Kent State Universityna sarvaAinda não há avaliações
- Audit Manual Clinical TrialDocumento22 páginasAudit Manual Clinical TrialnikjadhavAinda não há avaliações
- Roles and responsibilities in clinical trialsDocumento3 páginasRoles and responsibilities in clinical trialsyasahswi91Ainda não há avaliações
- Clinical ResearchDocumento2 páginasClinical ResearchEP YaredAinda não há avaliações
- CHEO REB termsDocumento4 páginasCHEO REB termsprabhaAinda não há avaliações
- Irb IecDocumento24 páginasIrb IecvansiAinda não há avaliações
- Clinical Trial ProtocolDocumento30 páginasClinical Trial Protocolanand kumar gondAinda não há avaliações
- NSABB P3CO WG Preliminary Draft Findings and Recommendations RE 21 SEP 2022 NIH NSABB MEETINGDocumento5 páginasNSABB P3CO WG Preliminary Draft Findings and Recommendations RE 21 SEP 2022 NIH NSABB MEETINGBrian O'SheaAinda não há avaliações
- Audits & Inspections CRO Perspective: DR - Prashant BodheDocumento74 páginasAudits & Inspections CRO Perspective: DR - Prashant BodheJayanta DasguptaAinda não há avaliações
- The Sourcebook for Clinical Research: A Practical Guide for Study ConductNo EverandThe Sourcebook for Clinical Research: A Practical Guide for Study ConductNota: 5 de 5 estrelas5/5 (1)
- Methods For Reticulocyte CountingDocumento52 páginasMethods For Reticulocyte CountingAri EcheverríaAinda não há avaliações
- Roles & ResponsibilitiesDocumento14 páginasRoles & ResponsibilitiesSara Montañez BarajasAinda não há avaliações
- Investigational New Drug (Ind) : N.Kanaka Durga DeviDocumento65 páginasInvestigational New Drug (Ind) : N.Kanaka Durga DeviNaresh Kumar Dhanikonda0% (1)
- Gene Therapy Application ProceduresDocumento75 páginasGene Therapy Application Proceduresintanhardianti7Ainda não há avaliações
- SOPDocumento5 páginasSOPJaime HinojosaAinda não há avaliações
- Part 1: Introduction Part 2: Responsibilities by Role Part 3: Summary of Key PointsDocumento13 páginasPart 1: Introduction Part 2: Responsibilities by Role Part 3: Summary of Key PointsFaye BaliloAinda não há avaliações
- Changing Role of A CRADocumento9 páginasChanging Role of A CRASaritaAinda não há avaliações
- Clinical trial documentsDocumento51 páginasClinical trial documentsRitika RaginiAinda não há avaliações
- Good Clinical PracticeDocumento29 páginasGood Clinical Practicerahul.gora9568Ainda não há avaliações
- Global Regulations in Clinical Trials by N.srinivas ICRIDocumento62 páginasGlobal Regulations in Clinical Trials by N.srinivas ICRIravi9247Ainda não há avaliações
- Remote Source Data Verification - EbookDocumento23 páginasRemote Source Data Verification - EbookMichael BonettAinda não há avaliações
- Essential Elements of Clinical TrialDocumento39 páginasEssential Elements of Clinical TrialmisganaAinda não há avaliações
- Sponsor and Principal Investigator: Responsibilities of The SponsorDocumento10 páginasSponsor and Principal Investigator: Responsibilities of The SponsorNoriAinda não há avaliações
- Essential Documents Checklist Clinical Trial InterventionalDocumento3 páginasEssential Documents Checklist Clinical Trial InterventionalPunk Rombus LeeAinda não há avaliações
- Institutional Review Board/Independent Ethics Committee (Irb/Iec)Documento40 páginasInstitutional Review Board/Independent Ethics Committee (Irb/Iec)Swati chauhanAinda não há avaliações
- Essentail Documents For Conduct of A Clinical TrialDocumento26 páginasEssentail Documents For Conduct of A Clinical TrialFarah Aman KhanAinda não há avaliações
- Investigator Responsibilities Good Clinical PracticeDocumento46 páginasInvestigator Responsibilities Good Clinical PracticeNitin ShahAinda não há avaliações
- A Comprehensive and Practical Guide to Clinical TrialsNo EverandA Comprehensive and Practical Guide to Clinical TrialsNota: 3 de 5 estrelas3/5 (1)
- Documentation of Clinical Trial Monitoring: A practical guide compliant with Good Clinical PracticeNo EverandDocumentation of Clinical Trial Monitoring: A practical guide compliant with Good Clinical PracticeNota: 5 de 5 estrelas5/5 (1)
- Regulation versus Litigation: Perspectives from Economics and LawNo EverandRegulation versus Litigation: Perspectives from Economics and LawAinda não há avaliações
- The Duty for Sponor Oversight in Clinical Trials: Practical Guide: 2nd Edition Clinical Data ReviewNo EverandThe Duty for Sponor Oversight in Clinical Trials: Practical Guide: 2nd Edition Clinical Data ReviewAinda não há avaliações
- 2009 SPWshop PocockDocumento31 páginas2009 SPWshop Pocockgopi_dey8649Ainda não há avaliações
- Ones Assignment Method for Solving Traveling Salesman ProblemDocumento8 páginasOnes Assignment Method for Solving Traveling Salesman Problemgopi_dey8649Ainda não há avaliações
- Up Ps CadverDocumento11 páginasUp Ps CadverJeshiAinda não há avaliações
- Insightofindia Quiz 2016-0-123Documento35 páginasInsightofindia Quiz 2016-0-123gopi_dey8649Ainda não há avaliações
- PSUR Instructions - FinalDocumento20 páginasPSUR Instructions - Finalgopi_dey8649Ainda não há avaliações
- IAS Mains Exam Paper 2014 General Studies Paper 2Documento10 páginasIAS Mains Exam Paper 2014 General Studies Paper 2gopi_dey8649Ainda não há avaliações
- Curves in SpaceDocumento7 páginasCurves in Spacegopi_dey8649Ainda não há avaliações
- Vector Analysis Paper I Segment Wise Questions From 1983 To 2011Documento6 páginasVector Analysis Paper I Segment Wise Questions From 1983 To 2011gopi_dey8649Ainda não há avaliações
- NSO Class 8 Solved Sample PaperDocumento8 páginasNSO Class 8 Solved Sample Papergopi_dey8649100% (1)
- Kesavandana Bharti CaseDocumento3 páginasKesavandana Bharti Casegopi_dey8649Ainda não há avaliações
- UPSC IAS Mains Exam Paper 2014 General Studies Paper 1Documento6 páginasUPSC IAS Mains Exam Paper 2014 General Studies Paper 1Santosh AvhadAinda não há avaliações
- Preclinical Research Clinical Research Nda Review Phase I NDA Basic Science ResearchDocumento1 páginaPreclinical Research Clinical Research Nda Review Phase I NDA Basic Science Researchgopi_dey8649Ainda não há avaliações
- Cbse - Biz: Paper Prepared byDocumento3 páginasCbse - Biz: Paper Prepared bygopi_dey8649Ainda não há avaliações
- Maths Book List - BipinDocumento1 páginaMaths Book List - Bipingopi_dey8649Ainda não há avaliações
- Kesavandana Bharti CaseDocumento3 páginasKesavandana Bharti Casegopi_dey8649Ainda não há avaliações
- Visionias PubadDocumento6 páginasVisionias Pubadgopi_dey8649Ainda não há avaliações
- General Studies Economics Part IDocumento22 páginasGeneral Studies Economics Part IbusisubbareddyAinda não há avaliações
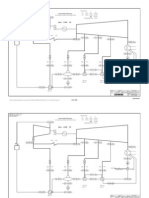
- System Head CurveDocumento1 páginaSystem Head Curvegopi_dey8649Ainda não há avaliações
- KksDocumento78 páginasKksgopi_dey8649Ainda não há avaliações
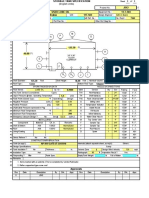
- I2-08-00249-01.3.1 Ed3 c070427 PerformanceDocumento6 páginasI2-08-00249-01.3.1 Ed3 c070427 Performancegopi_dey8649Ainda não há avaliações
- Electricity UntDocumento1 páginaElectricity Untgopi_dey8649Ainda não há avaliações
- Jadavpur BrocureDocumento16 páginasJadavpur Brocuregopi_dey8649Ainda não há avaliações
- Turbine Operation Manual 600 MW DongfangDocumento223 páginasTurbine Operation Manual 600 MW Dongfangkumar_ranjan_373% (11)
- p13036 Lanco 55 MW Ed-1 A121218 Performance PDFDocumento3 páginasp13036 Lanco 55 MW Ed-1 A121218 Performance PDFgopi_dey8649Ainda não há avaliações
- API 650 Tank Design 1Documento5 páginasAPI 650 Tank Design 1robertantoreni100% (9)
- ClarificationSolar PV - Thermal PDFDocumento18 páginasClarificationSolar PV - Thermal PDFgopi_dey8649Ainda não há avaliações
- 01 Cover NoteDocumento1 página01 Cover Notegopi_dey8649Ainda não há avaliações
- System Head CurveDocumento1 páginaSystem Head Curvegopi_dey8649Ainda não há avaliações
- Thailand TripDocumento6 páginasThailand Tripgopi_dey8649Ainda não há avaliações
- FC Vs FBDocumento8 páginasFC Vs FBMiguel SanchesAinda não há avaliações
- Saudi Arabia Power StationDocumento108 páginasSaudi Arabia Power StationEhab HarbAinda não há avaliações
- CNC Meldas 60-60sDocumento300 páginasCNC Meldas 60-60schidambaram kasiAinda não há avaliações
- Newsletter Template NewDocumento4 páginasNewsletter Template Newapi-458544253Ainda não há avaliações
- Indus Water Treaty & Emerging Water IssuesDocumento24 páginasIndus Water Treaty & Emerging Water Issuesu1umarAinda não há avaliações
- Teradata Version DifferencesDocumento3 páginasTeradata Version DifferencesShambuReddy100% (1)
- Daily DAWN News Vocabulary With Urdu Meaning (05 April 2020) PDFDocumento6 páginasDaily DAWN News Vocabulary With Urdu Meaning (05 April 2020) PDFAEO Begowala100% (2)
- Ite 001aDocumento6 páginasIte 001ajoshuaAinda não há avaliações
- 12 Fa02Documento4 páginas12 Fa02corsovaAinda não há avaliações
- Admin Interview Questions and Answers - Robert HalfDocumento2 páginasAdmin Interview Questions and Answers - Robert HalfWaqqas AhmadAinda não há avaliações
- Degx1 Dggx1 Us PartsDocumento24 páginasDegx1 Dggx1 Us PartsJeff RussoAinda não há avaliações
- Questionnaire For Future BLICZerDocumento1 páginaQuestionnaire For Future BLICZerAlejandra GheorghiuAinda não há avaliações
- Methods of Piling ExplainedDocumento3 páginasMethods of Piling ExplainedRajesh KhadkaAinda não há avaliações
- InductorsDocumento13 páginasInductorsManish AnandAinda não há avaliações
- SI Units in Geotechnical EngineeringDocumento7 páginasSI Units in Geotechnical EngineeringfaroeldrAinda não há avaliações
- Ahmad Humayun SohailDocumento6 páginasAhmad Humayun SohailHumayun SohailAinda não há avaliações
- Mobil Pegasus™ 1100 Series Mobil Pegasus™ 1100 Series Mobil Pegasus™ 1100 Series Mobil Pegasus™ 1100 SeriesDocumento3 páginasMobil Pegasus™ 1100 Series Mobil Pegasus™ 1100 Series Mobil Pegasus™ 1100 Series Mobil Pegasus™ 1100 SeriesMudabbir Shan AhmedAinda não há avaliações
- Wa0001Documento8 páginasWa0001varshasharma05Ainda não há avaliações
- Educational Technology & Education Conferences - January To June 2016 - Clayton R WrightDocumento93 páginasEducational Technology & Education Conferences - January To June 2016 - Clayton R WrightEsperanza Román MendozaAinda não há avaliações
- Product Data Sheet: Linear Switch - iSSW - 2 C/O - 20A - 250 V AC - 3 PositionsDocumento2 páginasProduct Data Sheet: Linear Switch - iSSW - 2 C/O - 20A - 250 V AC - 3 PositionsMR. TAinda não há avaliações
- DSSSB 01 2017Documento9 páginasDSSSB 01 2017Praneeta KatdareAinda não há avaliações
- ESG Service Information: BackgroundDocumento6 páginasESG Service Information: BackgroundAbdulSattarAinda não há avaliações
- MCQ in Services MarketingDocumento83 páginasMCQ in Services Marketingbatuerem0% (1)
- Siemens 1LE1 PDFDocumento308 páginasSiemens 1LE1 PDFharold100% (1)
- Library Management System Project ReportDocumento50 páginasLibrary Management System Project ReportSURAJ GAMINGAinda não há avaliações
- Chapter 11B: Survey of Database SystemsDocumento17 páginasChapter 11B: Survey of Database SystemsMurtaza MoizAinda não há avaliações
- Grant Park Platform Bedroom Set Furniture RowDocumento1 páginaGrant Park Platform Bedroom Set Furniture Rowjyzjz6sr65Ainda não há avaliações
- Qcs 2010 Section 5 Part 8 Transportation and Placing of ConcreteDocumento7 páginasQcs 2010 Section 5 Part 8 Transportation and Placing of Concretebryanpastor106Ainda não há avaliações
- Brake Pedals and ValveDocumento4 páginasBrake Pedals and Valveala17Ainda não há avaliações
- Rob Thomas Digital Booklet - Cradle SongDocumento15 páginasRob Thomas Digital Booklet - Cradle SongAgnieszka ŁukowskaAinda não há avaliações